





Abstract
Persistent left superior vena cava (PLSVC) is found in 0.3–2% of the population. Pacemaker implant in PLSVC can be technically challenging. Most operators have hitherto manipulated ventricular leads through the coronary sinus (CS) into the right ventricle (RV). In this case series, we describe the use of standard passive tined ventricular leads implanted into the left ventricular (LV) epicardial veins in PLSVC.
Three patients with PLSVC underwent pacemaker implantation for bradycardia. Contrast injection in the dilated CS identified LV coronary veins. Standard passive tined pacing leads were manoeuvred into these branches using hand-shaped stylets without need for additional equipment. Atrial leads were actively fixed to the anterolateral right atrial wall. There were no procedural complications. Chronic ventricular capture threshold at 6 months of follow-up was 1.0 mV@ 0.4 ms.
Implanting standard leads into the LV veins in PLSVC is safe, effective, and simple without the need for special tools. This is easier than manipulating leads into the RV in PLSVC. Longer-term follow-up and dedicated clinical trials are needed to evaluate the efficacy and safety of this approach.
Novel approach to permanent pacing in persistent left superior vena cava using standard pacemaker leads without additional tools.
Ventricular lead placement in coronary veins instead of the right ventricle, with good medium-term parameters.
Right atrial–left ventricular pacing as a potential application in heart failure.
Introduction
Persistent left superior vena cava (PLSVC) is an uncommon anatomical variant, found in 0.3–2% of the population.1 Its incidence can be as high as 10% when it is associated with other congenital cardiac anomalies.1,2 Not infrequently, the presence of a left-sided SVC is only discovered during pacemaker implantation.
Attempting to implant pacing leads in the right atrium (RA) and right ventricle (RV) through the PLSVC and dilated coronary sinus (CS) can be technically challenging. This is especially so for the RV lead, which has to make an acute turn as it exits from the CS at the postero-inferior aspect of the RA to cross the tricuspid annulus towards the RV apex. Positioning of the RA lead also requires the use of custom-shaped stylets or steerable stylets/sheaths. Active fixation leads are preferred in these cases as they offer better stability.
In the literature, there are case reports detailing the implant of leads in the RA and RV in PLSVC, with some requiring special tools.3–7 Likewise, implantation of specially designed left ventricular (LV) pacing leads using dedicated delivery systems for cardiac resynchronization therapy (CRT) have been described8,9 in patients with PLSVC.
In this paper, we describe a case series of three patients with PLSVC who had pacemakers implanted for bradycardia indications. Standard passive bipolar leads were used for the ventricle, with the leads being positioned in the LV epicardial veins instead of RV. The atrial leads were positioned in the anterolateral RA using standard active fixation bipolar leads. No special tools, sheaths, or delivery systems were required. There were no complications in any of the three cases.
Methods and results
Case 1
A 72-year-old man with diabetes mellitus, hypertension, mild renal impairment, and minor coronary artery disease was referred for symptomatic sinus node dysfunction. He suffered from frequent near-syncopal attacks, and had documented bradycardia of 33 b.p.m. on Holter monitoring. His echocardiogram showed normal LV ejection fraction of 56%.
Upper-limb venogram prior to vascular access showed the presence of a PLSVC, but the decision was made to proceed with pacemaker implant on the left side as the patient was right handed. Following left axillary vein access, contrast injection through a 7F Swan-Ganz balloon catheter showed a dilated CS and a large middle cardiac vein (Figure 1A). A 58 cm Medtronic passive tined pacing lead (model 5054–58) was advanced down the middle cardiac vein, using a hand-shaped stylet with a simple curve within the lead to direct it into a side-branch of that vein. Initial parameters were R-wave 11.8 mV, impedance 1359 Ω, and capture threshold 1.6 V @1.0 ms. A 52 cm Medtronic active lead (model 4076–52) was used for the atrium, again with a hand-shaped stylet to direct the lead to the anterolateral RA wall. Parameters were P-wave 3.4 mV, impedance 476 Ω, and capture threshold 0.9 V@ 0.5 ms. A Medtronic Relia DDDR pulse generator was used. At 6-month follow-up, the parameters for the ventricular lead were R-wave 15.68–22.4 mV, impedance 1282 Ω, and threshold 1.0 [email protected] ms. For the atrial lead: P-wave 4.0–5.6 mV, impedance 400 Ω, and threshold 0.5 V @ 0.5 ms. Atrial pacing was 68.3%, ventricular pacing 2.1%. Post-implant chest X-ray is shown in Figure 2A.
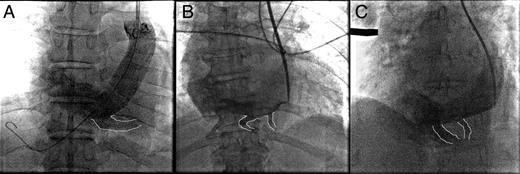
(A–C) Injection of contrast into the dilated CS showing branches of the epicardial venous system (outlined).
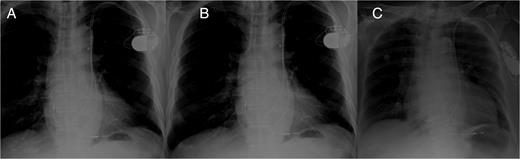
(A–C) Post-implant chest X-ray of Cases 1–3, showing position of the pacing leads.
Case 2
A 77-year-old woman with diabetes mellitus, coronary artery disease, and paroxysmal atrial fibrillation was referred for sinus node dysfunction. She had syncope with 9 s pauses documented on Holter. Echocardiogram showed LV ejection fraction of 60% with LV hypertrophy. Persistent left superior vena cava was noted on left upper limb venogram, but the decision was to proceed with left-sided pacemaker implant as the patient was right handed.
Following left axillary vein access, contrast injection through a 7F Swan-Ganz balloon catheter showed a dilated CS, a middle cardiac vein, and posterolateral vein. (Figure 1B). A 58 cm Medtronic passive pacing lead (model 5054–58) was advanced down the posterolateral cardiac vein, using a hand-shaped curved stylet within the lead to manoeuvre it. Initial parameters were R-wave 13.7 mV, impedance 1123 Ω, and capture threshold 0.8 V @1.0 ms. A 52 cm Guidant active lead (model 4137) was used for the atrium, which was fixed to the anterolateral RA wall in the same way as for Case 1. Parameters were P-wave 2.1 mV, impedance 565 Ω, and capture threshold 1.9 V@ 1.0 ms. A Medtronic Relia DDDR pulse generator was used. At 6-month follow-up, the parameters for the ventricular lead were R-wave 11.2 mV, impedance 704 Ω, and threshold 1.0 [email protected] ms. For the atrial lead: P-wave 2.0–2.8 mV, impedance 554 Ω, and threshold 0.75 V @ 0.4 ms. Atrial pacing was 67.2%, and ventricular pacing <1%. Post- implant chest X-ray is shown in Figure 2B.
Case 3
A 75-year-old woman with diabetes mellitus, hypertension, and persistent atrial fibrillation on warfarin was referred for syncope resulting in traumatic subdural haemorrhage. There were multiple pauses up to 7 s on telemetry monitoring.
Following left axillary vein access, contrast injection through a 7F-long vascular sheath showed a PLSVC, dilated CS, and a large middle cardiac vein (Figure 1C). A 58 cm St Jude Medical passive pacing lead (model 1948/58) was advanced down the middle cardiac vein, using a hand-shaped curved stylet. Initial parameters were R-wave 10.2 mV, impedance 1272 Ω, and capture threshold 1.0 V @1.0 ms. A St Jude Medical Verity VVIR pulse generator was used. At 6-month follow-up, the parameters for the ventricular lead were R-wave 15.7–16.3 mV, impedance 1298 Ω, and threshold 1.0 [email protected] ms. Ventricular pacing was 43%. Post-implant chest X-ray is shown in Figure 2C.
Discussion
There are several case reports in the literature describing the implantation of pacing leads through a PLSVC. Except for CRT cases, the operators have invariably implanted the ventricular lead in the RV apex using active fixation leads.
In CRT cases, all the operators used specially designed LV leads and delivery tools to cannulate the LV venous branches using angioplasty guide wires and techniques; with one exception where the operators used a passive lead designed for the RV.9
In this case series, we demonstrated that placement of a standard passive tined transvenous lead (designed for the RV) into the LV epicardial venous system is technically feasible, relatively easy, and yields good results. This was achieved without the need for special leads designed for CRT or dedicated delivery tools. All that is required is shaping of the stylet that comes packaged with the passive lead in order to direct it into the vein of choice. While the results are encouraging, this case series is not a clinical trial designed to evaluate the safety and efficacy of this approach vis-à-vis the use of standard LV leads in the coronary veins or passive tined leads in the RV in the setting of PLSVC. The longer-term results and performance of the RV lead in the coronary veins is unknown.
This approach is less tedious than trying to manipulate the pacing lead through a tortuous angulated course from the CS, through the tricuspid valve and into the RV. There is also possibly a lower risk of lead dislodgement in placing the lead in the LV veins because there is less tension in the lead. Positioning a standard passive ventricular lead in the coronary veins is made easier in the setting of PLSVC because the veins are dilated and the route taken by the lead is more direct.
Although there was initial concern that the pacing thresholds may be high in the epicardial position as compared with the endocardial position, we have found that chronically (6-month follow-up), the capture thresholds were excellent, at 1.0 mV @ 0.4 ms for all three cases. This is despite the thresholds being slightly high at implant. Certainly, the possible subsequent loss of ventricular capture in the longer run is of concern in patients with atrioventricular block, and long-term follow-up will give us a clearer picture. That being said, short of overt lead dislodgements, pacing parameters usually remain stable three months after implant.
In using a passive tined lead, there is a theoretical possibility of the tines preventing the pacing poles from making contact with the myocardial tissue and thereby leading to high thresholds. This may be the explanation for the slightly higher capture thresholds we observed at implant; but this seems to resolve with time as the lead ‘settles in’, leading to excellent parameters chronically as we have shown. At present, there are LV leads already in use that possess passive tines on the lead body for lead stability. Examples include the Medtronic 4396, and Boston-Scientific Easytrak 2, and Easytrak 3.
Since there is no need to use dedicated LV lead delivery systems and special LV leads, there are no additional costs involved compared with a traditional pacemaker implant.
Pacing the ventricle from the LV may also confer advantages as compared with RV apical pacing. Some studies have showed that LV pacing is associated with better haemodynamics and cardiac output.10–13 We were not able to demonstrate in these cases whether chronic pacing from the LV had any effect on the cardiac size and function since the percentage of ventricular pacing was very low in two out of the three cases. In case 3, where the percentage of ventricular pacing was 43%, there was no cardiac enlargement or deterioration of systolic function on follow-up echocardiogram 6 months after implant.
With the demonstration of feasibility of using standard pacing leads in the LV venous system, there is potential for application in heart failure using RA–LV sequential pacing. There are already studies showing that LV pacing yields equivalent outcomes to biventricular pacing in heart failure patients with left bundle branch block and normal atrioventricular conduction.14–16 If this is the case, a standard dual-chamber pacemaker with the atrial lead in the RA and ventricular lead in the LV venous system might be an economical means of providing CRT in chronic heart failure patients with left bundle branch block but preserved atrioventricular conduction. This might even be a practical means to provide CRT to large numbers of heart failure patients in developing countries, where access to such therapies is limited mostly by affordability. Patients with normal anatomy (i.e. without PLSVC) will require LV delivery sheaths and tools to access the CS and epicardial veins; which may erode some of the cost savings with such an approach. Nonetheless, this may still work out to be more economical than a standard CRT device.
Conclusion
In patients with PLSVC, placement of a standard passive tined pacing lead in the LV epicardial veins is safe, effective, and technically simple. It does not require special tools or leads and yields good results at 6 months' follow-up. Longer-term follow-up and dedicated clinical trials are needed to evaluate the efficacy and safety of this approach.
Conflict of interest: none declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}