





Case report
A 42-year-old man with an acute inferoposterolateral ST-segment elevation myocardial infarction was resuscitated from out-of-hospital cardiac arrest. After successful primary coronary intervention of an occluded circumflex coronary artery, the patient was referred to the cardiac care unit and treated with therapeutic hypothermia. During the initial cooling phase, the target temperature (33°C) declined accidentally to 31.5°C. Thereafter, frequent episodes of ventricular fibrillation (VF) occurred, requiring multiple external shocks and prolonged cardiac life support by reason of inefficient defibrillation. The 12-lead ECG ( Figure 1 A ) revealed giant Osborn waves in the left precordial and lateral leads (arrows), prolongation of the corrected QT interval (590 ms), ST-segment depression in leads V3 to V6, and pathological Q waves inferiorly. Monitor-lead recording during defibrillation of spontaneous VF episodes showed prominent J-wave deflections and short coupling of the initiating ventricular premature beat ( Figure 1 D , asterisk). With rewarming, the Osborn waves progressively decreased in amplitude ( Figure 1 B ) and disappeared completely ( Figure 1 C ). No further ventricular arrhythmias occurred at a core temperature maintained at 36°C for 48 h, and the patient recovered with favourable neurological outcomes.
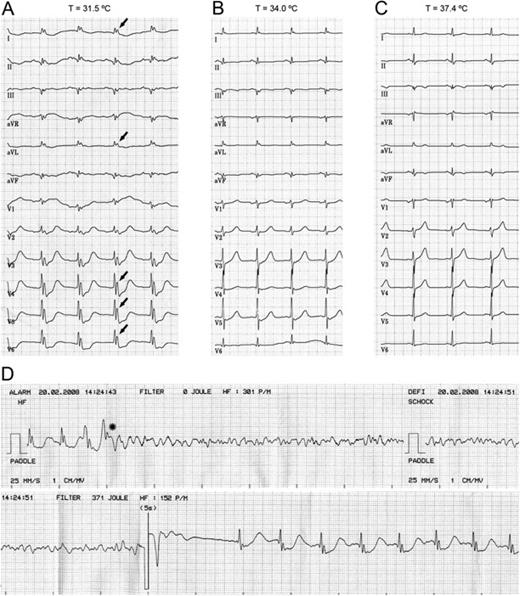
Electrocardiograms of an out-of-hospital cardiac-arrest survivor who experienced multiple episodes of refractory VF during therapeutic hypothermia. The 12-lead ECG obtained at 31.5°C showed QT prolongation and giant Osborn waves in the left lateral leads ( A , arrows), which progressively decreased in amplitude with rewarming ( B , C ). Single-lead recording during VF episodes revealed initiating premature beats with a short coupling related to the preceding prominent J wave ( D , asterisk).
Discussion
Prominent J deflections attributed to hypothermia have been termed Osborn waves in honour of Osborn's landmark description in 1953. 1 Osborn waves most commonly manifest on the inferolateral leads with amplitude inversely related to body temperature. Hypothermia-induced J waves are the result of a marked accentuation of the action potential notch in the epicardium but not in the endocardium, presumably due to the effect of cold temperature to slow the activation kinetics of Ito less than that of the l -type Ca 2+ current. 2 The resulting transmural voltage gradient, in conjunction with slowing of transmural impulse conduction, provides a substrate for Phase-2 re-entry, which may generate a closely coupled extrasystole triggering VF in the ‘cooled’ heart.
Mild therapeutic hypothermia has been shown to improve outcomes in survivors of out-of-hospital cardiac arrest. 3 However, monitoring temperature levels is very important as hypothermia <32°C can cause cardiac arrhythmias including VF, which may be refractory in a particular setting such as myocardial ischaemia.

{kind=link}