





Abstract
Nowadays, trans-septal (TS) puncture is a relatively safe and straightforward procedure in experienced hands. However, in the presence of a thick, aneurysmatic or extremely elastic fossa ovalis crossing the septum might be challenging. We here describe the use of a novel guidewire that permits easy and safe ‘over the wire’ TS access during atrial fibrillation ablation.
Introduction
Catheter ablation has become a widely accepted therapy for atrial fibrillation (AF). This procedure requires trans-septal (TS) access with one or more punctures as the triggers of this arrhythmia are mostly located in the pulmonary veins. 1 Nowadays, TS puncture is a relatively safe procedure in experienced hands and the left atrium (LA) can be easily accessed in most cases. However, in the presence of a thick, aneurysmatic or extremely elastic fossa ovalis (FO) crossing the septum might prove challenging for the operator. In these cases, the use of a novel nitinol J-shaped guidewire might prove helpful and safe in gaining LA access.
Case report
A 59-year-old man was referred to our centre for radiofrequency pulmonary vein isolation ablation because of highly symptomatic and drug refractory paroxysmal AF. The pre-procedural transoesophageal echocardiography (TEE) showed an anatomically intact FO with no patent foramen ovalis. The same examination excluded the presence of thrombi in the LA and estimated its size around 45 mm. The patient also underwent a computed tomography scan the day before the procedure in the purpose of merging morphological and electroanatomical information during ablation. We thus proceeded to real-time three-dimensional TEE-guided TS puncture with the patient in total sedation. Before starting catheterization, the TEE probe was introduced and optimal imaging of the FO was obtained. After having introduced a quadripolar catheter in the coronary sinus for the purpose of pacing during ablation, we placed via the right femoral vein an 8 Fr TS sheath (SL0, St Jude Medical, MN, USA) in the right atrium. Through the latter, we advanced Brockenbrough TS needle (BRK-1) and positioned it against the FO. This was confirmed under echocardiographical imaging by applying slight pressure on the septum to obtain typical ‘tenting’ effect of the FO. However, despite ideal location of the puncture site, the septum could not be crossed. Further attempts using different needle orientation, changing site of puncture, trying different needle types (including BRK-1 extra sharp) or sheath curves, all proved unsuccessful in achieving TS access. Tenting of the FO could be visualized during all attempted punctures underlining each time the correct positioning of the needle in the septum. We thus decided to perform the puncture using a novel J-shaped TS guidewire (Safe Sept, Pressure Products, Inc., USA) ( Figure 1 ). This 0.014 in. diameter nitinol guidewire permits easy access through the septum thanks to its sharp specially designed tip. After having obtained tenting with the TS system under echocardiographical guidance, the guidewire that was advanced through the needle could easily cross the FO ( Figure 2 ). Immediately after accessing the LA, the tip assumes a J shape, making it difficult for the wire to penetrate further tissue. The wire was further advanced in the left superior pulmonary vein (LSPV). Thus, the TS needle along with dilator and sheath could safely be advanced ‘over the wire’ minimizing the risk of damaging LA structures ( Figure 3 ). Furthermore, a radiopaque coil along the shaft of the wire permitted its clear fluoroscopic visualization during every step of advancement in the LA.
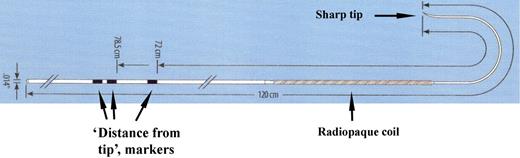
Diagram showing the structure of the Safe Sept J-shaped guidewire.
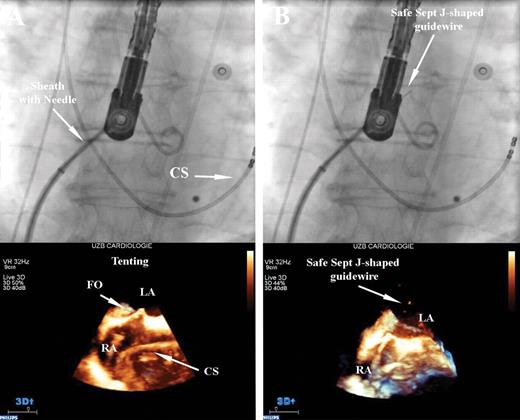
( A ) ‘Tenting’ effect of fossa ovalis during trans-septal puncture. ( B ) Trans-septal puncture with visualization of Safe Sept J-shaped guidewire in the left atrium, and ‘tenting’ of fossa ovalis around the dilator. FO, fossa ovalis; LA, left atrium; RA, right atrium; CS, coronary sinus.
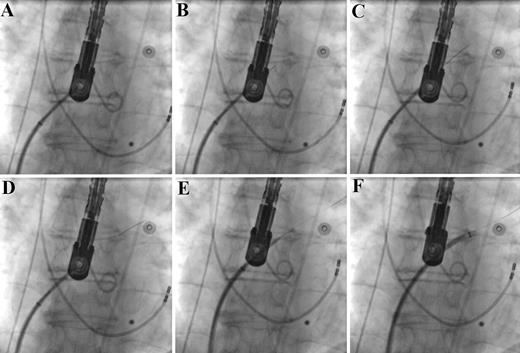
Sequence of antero-posterior X-ray images showing the trans-septal puncture with the Safe Sept J-shaped guidewire: ( A ) trans-septal system positioned against the inter-atrial septum; ( B ) crossing of the septum with the Safe Sept J-shaped guidewire; ( C ) advancement of the guidewire towards the left superior pulmonary vein; ( D ) guidewire placed in the left superior pulmonary vein; ( E ) advancement of the trans-septal system in the left atrium ‘over the wire’; ( F ) retraction of needle and dilator: leaving the sheath in the left atrium under saline flush.
Brief discussion
Trans-septal puncture for AF ablation is relatively safe in experienced hands, and LA can be easily accessed in most cases. 2 Furthermore, when performed under TEE guidance, direct visualization of the FO is obtained minimizing the risk of severe complications. 3 However, when dealing with very resistant, elastic, or aneurysmatic septums, puncturing might prove extremely difficult. In these cases, the J-shaped Safe Sept guidewire might afford TS access in total safety. Its most interesting features are the immediate down curving into a J shape after crossing the septum and the possibility to advance the TS system ‘over the wire’ after the placement of the wire in the LSPV similar to the previously described technique by Cheng using an 0.014 in. angioplasty guidewire inserted in to the needle hub and advanced in the LA. 4 This greatly diminishes the probabilities of accidental penetration of critical anatomical structures such as the aortic root and the posterior wall of the LA.
Conclusion
The Safe Sept guidewire bears the double advantage of: (i) safely gaining LA access when dealing with very elastic or thick septums similar to previously described commercially available radiofrequency perforation devices (TorFlex Transseptal Guiding Sheath, Baylis Medical Company, Inc.) 5 and (ii) minimizing the risk of accidentally damaging critical structures when advancing the TS system ‘over the wire’ in the LA. However, this tool facilitates LA access at the condition that the TS system is positioned at the thinnest part of the FO.
Conflict of interest: none declared.

{kind=link}
{kind=link}
{kind=link}