





Abstract
Adherence to treatment guidelines in heart failure (HF) patients (pts) is of major prognostic importance, but thorough implementation of guidelines in routine care remains insufficient. Introducing hybrid comprehensive telerehabilitation (HCTR) consisting of telecare, telerehabilitation and remote monitoring of implantable devices might be an option to improve adherence to recommendation and can affect the prognosis. Purpose to investigate the association of adherence to HCTR with mortality and hospitalization. Methods The present analysis formed part of TELEREH-HF multicenter, randomized trial that enrolled 850 HF pts (NYHA I-III,LVEF≤40%). Patients were randomized 1:1 to HCTR plus usual care or usual care only and followed up for 14 to 26 months. During the first 9 weeks, pts underwent either an HCTR (1 week in hospital and 8 weeks at home) or usual care. This analysis focuses on pts randomized to HCTR. Adherent pts were those who adhered both to the number of training sessions prescribed and to the duration of the prescribed cycle by at least80%; non-adherent pts, were those who adhered<20% to the prescribed number of training sessions and their duration. The remaining pts were classified as partially adherent.
There were 350 (88.4%) adherent pts, 39 (9.8%) partially adherent pts and 7 (1.8%) non-adherent pts. There were 54 deaths during follow-up in the HCTR arm. Non-adherence or partial adherence was associated with statistically significantly higher risk of cardiovascular (CV) mortality (hazard ratio (HR) = 2.62, p=0.021); all-cause mortality or HF hospitalization (HR=1.71, p=0.038); CV mortality or HF hospitalization (HR=1.89, p=0.014).
The adherence to HCTR was very high. Adherence to HCTR was associated with improved prognosis for CV mortality.
Outcomes by Patients' Adherence to HCTR
| Outcome | Adherent patients (n=350) | Partially adherent and non-adherent patients (n=46) | Hazard ratio 95% Wald CL | p-value | ||
|---|---|---|---|---|---|---|
| N (%) | Event rate at 26 months | N (%) | Event rate at 26 months | |||
| All-cause mortality | 38 (10.9%) | 10.5 | 8 (17.4%) | 17.4 | 1.79 [0.83–3.85] | 0.129 |
| Cardiovascular mortality | 23 (6.6%) | 6.3 | 7 (15.6%) | 15.2 | 2.62 [1.12–6.13] | 0.021 |
| All-cause hospitalization | 201 (57.4%) | 58.3 | 19 (41.3%) | 47.9 | 0.99 [0.62–1.58] | 0.963 |
| Cardiovascular hospitalization | 126 (36.0%) | 38.0 | 11 (23.9%) | 28.1 | 0.84 [0.45–1.55] | 0.569 |
| Heart failure hospitalization | 86 (24.6%) | 25.7 | 13 (28.3%) | 33.8 | 1.6 [0.89–2.86] | 0.113 |
| All-cause mortality or all cause hospitalization | 208 (59.4%) | 59.7 | 23 (50.0%) | 55.3 | 1.16 [0.75–1.78] | 0.505 |
| All-cause mortality or cardiovascular hospitalization | 151 (43.1%) | 43.9 | 17 (37.0%) | 40.9 | 1.08 [0.65–1.78] | 0.761 |
| All-cause mortality or heart failure hospitalization | 105 (30.0%) | 30.6 | 17 (37.0%) | 41.2 | 1.71 [1.03–2.86] | 0.038 |
| Cardiovascular mortality or heart failure hospitalization | 95 (27.1%) | 28.1 | 17 (37.0%) | 41.2 | 1.89 [1.13–3.16] | 0.014 |
| Outcome | Adherent patients (n=350) | Partially adherent and non-adherent patients (n=46) | Hazard ratio 95% Wald CL | p-value | ||
|---|---|---|---|---|---|---|
| N (%) | Event rate at 26 months | N (%) | Event rate at 26 months | |||
| All-cause mortality | 38 (10.9%) | 10.5 | 8 (17.4%) | 17.4 | 1.79 [0.83–3.85] | 0.129 |
| Cardiovascular mortality | 23 (6.6%) | 6.3 | 7 (15.6%) | 15.2 | 2.62 [1.12–6.13] | 0.021 |
| All-cause hospitalization | 201 (57.4%) | 58.3 | 19 (41.3%) | 47.9 | 0.99 [0.62–1.58] | 0.963 |
| Cardiovascular hospitalization | 126 (36.0%) | 38.0 | 11 (23.9%) | 28.1 | 0.84 [0.45–1.55] | 0.569 |
| Heart failure hospitalization | 86 (24.6%) | 25.7 | 13 (28.3%) | 33.8 | 1.6 [0.89–2.86] | 0.113 |
| All-cause mortality or all cause hospitalization | 208 (59.4%) | 59.7 | 23 (50.0%) | 55.3 | 1.16 [0.75–1.78] | 0.505 |
| All-cause mortality or cardiovascular hospitalization | 151 (43.1%) | 43.9 | 17 (37.0%) | 40.9 | 1.08 [0.65–1.78] | 0.761 |
| All-cause mortality or heart failure hospitalization | 105 (30.0%) | 30.6 | 17 (37.0%) | 41.2 | 1.71 [1.03–2.86] | 0.038 |
| Cardiovascular mortality or heart failure hospitalization | 95 (27.1%) | 28.1 | 17 (37.0%) | 41.2 | 1.89 [1.13–3.16] | 0.014 |
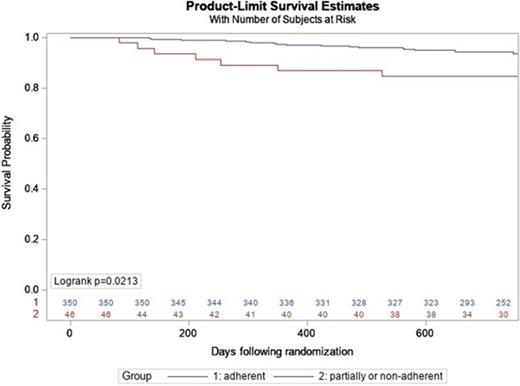
Kaplan-Meier Probability of CV Mortality
Type of funding source: Public grant(s) – National budget only. Main funding source(s): National Centre for Research and Development, Warsaw, Poland


{kind=link}