





Abstract
Approximately one-third of the patients presenting with non-ST elevation myocardial infarction (NSTEMI) have diabetes. From these, two-thirds have multivessel coronary disease. The impact of completeness of revascularization in this population remains unclear.
To evaluate the contemporary patterns of coronary revascularization among patients with diabetes and NSTEMI, and the clinical outcomes stratified by anatomic completeness of revascularization.
All patients with diabetes and multivessel disease admitted for NSTEMI between April 2009 and March 2020 in Ontario, Canada were included. Patients with previous coronary artery bypass graft surgery (CABG) at any time, percutaneous coronary intervention (PCI) in the previous 90 days, or shock were excluded. Patients were classified in four groups, from the most to the least complete revascularization strategy: CABG, complete revascularization with PCI, incomplete revascularization with PCI, or no revascularization. Outcomes included all-cause death and the composite of all-cause death, myocardial infarction, and stroke. Multivariable Cox regression was used to account for confounding (demographics, comorbidities, left ventricular function, coronary anatomy, laboratory tests, and diabetes treatment).
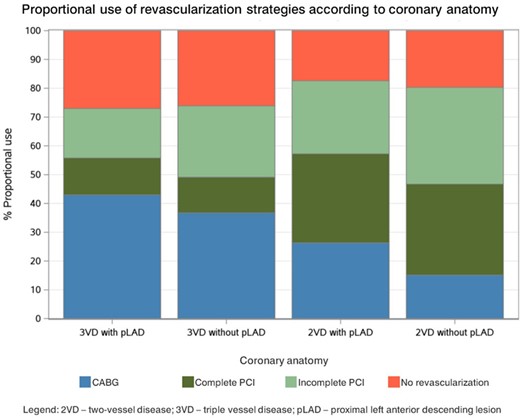
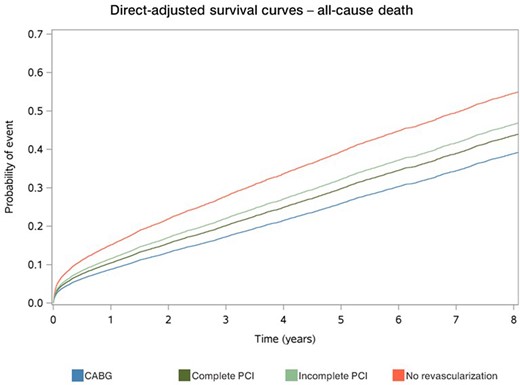
We included 14,511 patients (mean age: 68.7±11.5y; 69.6% males). A total of 4,525 (31.2%) patients were treated with CABG, 3,008 (20.7%) with complete PCI, 3,624 (25.0%) with incomplete PCI and 3,354 (23.1%) were not revascularized. Patients with more complex coronary disease were more frequently treated with CABG, while PCI was more common in those with less complex disease (p<0.001; Fig 1). The mean number of grafts in the CABG group was 3.4±1.0. The mean number of stents in the complete and incomplete PCI groups was 2.4±1.3 and 1.7±0.9, respectively. Adjusted 5-y risks of all-cause death following CABG, complete PCI, incomplete PCI and no revascularization were, respectively, 25.9%, 29.8%, 32.2%, and 39.4%. Over a median follow-up of 5.8ys, CABG was associated with reduced all-cause death compared with complete PCI (HR 0.82; 95%CI 0.75 - 0.90), incomplete PCI (HR 0.73; 95%CI 0.67 - 0.80), or no revascularization (HR 0.54; 95%CI 0.50 - 0.58); p<0.001 for all (Fig 2). Adjusted 5-y risks of the composite endpoint following CABG, complete PCI, incomplete PCI and no revascularization were, respectively, 34.0%, 41.5%, 44.6%, and 52.9%. CABG was associated with reduced rates of the composite endpoint compared with complete PCI (HR 0.75; 95%CI 0.69 - 0.81), incomplete PCI (HR 0.67; 95%CI 0.62 - 0.72), or no revascularization (HR 0.50; 95%CI 0.47 - 0.54); p<0.001 for all.
Author notes
Funding Acknowledgements: Type of funding sources: Public grant(s) – National budget only. Main funding source(s): Canadian Institutes of Health Research


{kind=link}