





Abstract
The optimal revascularization strategy for severe coronary artery disease (CAD) in women remains controversial. Despite differences between women and men in the development of CAD, there remains a paucity of comparative real-world observational evidence comparing percutaneous coronary intervention (PCI) to coronary artery bypass grafting (CABG) in women.
We evaluated short and long-term outcomes of PCI and CABG in women with severe CAD.
We conducted a propensity score-matched retrospective cohort study using linked clinical and administrative databases in Ontario, Canada to obtain records of women with left main, 3-vessel disease, or 2-vessel disease with proximal left anterior descending artery involvement undergoing PCI or CABG from April 1st, 2012 to December 31st, 2021. Patients who were >80 years of age and patients who underwent urgent or emergent procedures were excluded for the primary analysis. The primary outcome was a composite of myocardial infarction, stroke, repeat revascularization, and death (MACCE). Secondary outcomes included the individual components of MACCE and a composite of readmission for MI, heart failure, and stroke. Following multiple imputation and propensity score-matching, the Cox proportional hazards model and Fine-Gray sub-distribution hazard model with robust variance estimators accounting for death as a competing risk were used to evaluate long-term outcomes.
In the primary cohort, 2469 patients underwent PCI and 3,721 patients underwent CABG. After propensity score matching, including by coronary disease territory, 2,033 well-balanced pairs were identified, with standardized mean differences <0.10 for all covariates. In-hospital death and stroke were significantly lower with PCI than with CABG (0.7% vs 1.5%, p=0.036) and (<0.2% vs 1.4%, p<0.001), respectively, and there was no difference in perioperative MI between PCI and CABG (1.1% vs 0.6%, p=0.121). At a median (IQR) of 5.1 (2.9-7.5) years, major adverse cardiac and cerebrovascular events (MACCE) was higher with PCI compared with CABG (37.7% vs 23.3%, HR 1.79, [95% CI: 1.66-1.91], p<0.001) (Figure 1). All-cause mortality was higher with PCI compared with CABG (17.8% vs 13.4%, HR 1.33, [95% CI: 1.21-1.45], p<0.001) (Figure 2). The composite readmission outcome (MI, heart failure, stroke) was higher with PCI compared with CABG (16.2% vs 11.2%, HR 1.42, [95% CI: 1.37-1.48], p<0.001).
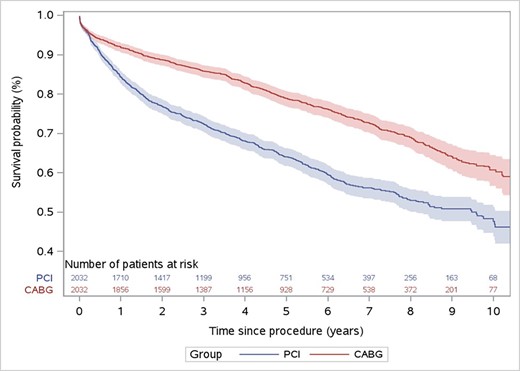
MACCE free survival
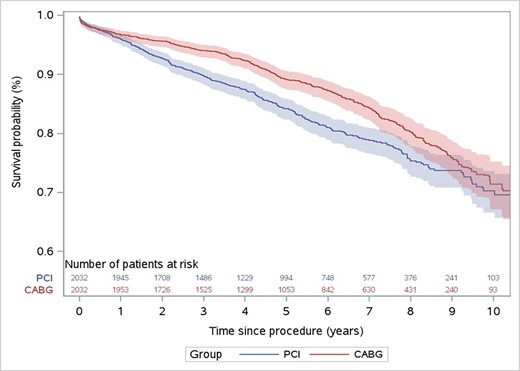
Overall survival
Author notes
Funding Acknowledgements: Type of funding sources: Private grant(s) and/or Sponsorship. Main funding source(s): This research is funded by a partnership between the Canadian Cardiovascular Society (CCS) and Bayer Inc. and by Weill Cornell Medicine Institutional Funds.


{kind=link}