





Abstract
Paradoxical embolism due to patent foramen ovale (PFO) can cause cryptogenic stroke. Agitated saline contrast transthoracic echocardiography (ASC-TTE) is an essential diagnostic tool for PFOs, and provocation using the Valsalva manoeuvre (VM) is necessary during the examination. Although VM is the standard method, assessing whether sufficient provocation has been achieved can pose challenges for the patients and examining staff. Conversely, a party balloon inflation manoeuvre (PBIM), which we previously reported (1, 2), offered a clear visual confirmation of provocation than conventional VM and showed effectiveness in cases of inadequate provocation. However, collective evaluation of PBIM by group remains unknown.
This study aimed to demonstrate the superiority of PBIM over standard provocative methods, such as conventional or inferior vena cava compression VM, during ASC-TTE.
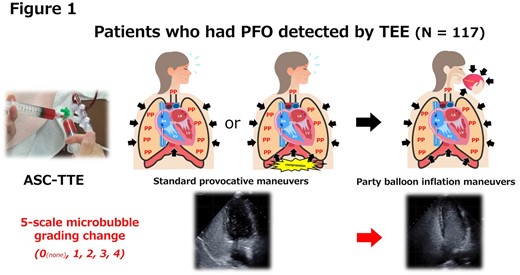
This multicentre registry study was conducted across eight high-volume institutions in Japan. A total of 117 consecutive patients (62.3% men, mean age; 56.2 ± 13.8 years, as of December 31, 2023) in whom paradoxical embolism was suspected and PFO was detected by transesophageal echocardiography, underwent PBIM and standard provocative methods during ASC-TTE. We compared them using a five-point microbubble grade (none or 1–4) using the right-to-left cardiac shunt as the primary endpoint (Figure 1).
PBIM produced microbubble upgrading in 51 (43.6%, yellow panels in Figure 2), no change in 54 (46.1%), and down-grading in 12 (10.3%, blue panels in Figure 2) patients, compared to standard provocative methods. Wilcoxon paired analysis revealed that PBIM had a significantly larger microbubble grade than the standard provocative methods (median 3.0 interquartile range (IQR) [3.0–4.0] vs 3.0 IQR [1.7–4.0], p<0.001). If significant right-to-left shunt was grade ≥2, which was considered as the indication of catheter PFO closure, the pairwise McNemar’s test showed diagnostic performance of significant right-to-left cardiac shunt using PBIM improved from 75.2% to 91.5% (improvement rate; 16.3%, 95% CI; 8.4–24.0, p<0.001). Logistic regression analysis showed insufficient balloon inflation due to inexperience and risk of paradoxical embolism score independently associated with downgrading in PBIM after adjustments for age, sex, clinically relevant variables, and other echocardiographic parameters (odds ratio (OR); 24.0, 95% interquartile range (CI); 3.3–172.1, p<0.01 and OR; 0.60, 95% CI; 0.39–0.91, p<0.05, respectively).
Primary endpoints
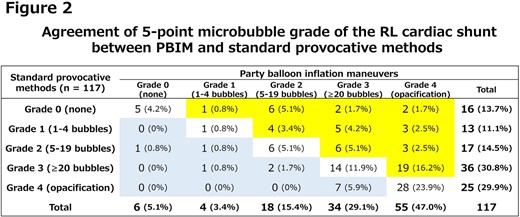
Agreement of 5-point microbubble grade
Author notes
Funding Acknowledgements: Type of funding sources: Private company. Main funding source(s): Abbott Medical Japan LLC (Tokyo, Japan) scholarship fund


{kind=link}