





Abstract
The DELIVER trial enrolled subjects with acute heart failure (AHF) and preserved ejection fraction (HFpEF) who had elevated biomarkers and cardiac structural abnormalities. Given the benefits of sodium-glucose cotransporter 2 inhibitors (SGLT2i) in AHF, it is important to understand the differences between DELIVER-type and non-DELIVER-type patients and how their classification may shift over time.
This study enrolled patients hospitalized for AHF with LVEF ≥ 50%. Patients with elevated N-terminal pro B-type natriuretic peptide (NT-proBNP ≥ 300 or 600 pg/mL, depending on cardiac rhythm) and cardiac structural abnormalities (enlarged left atrial volume or index, or left ventricular hypertrophy) were classified as DELIVER-type. Patients who did not meet these criteria were classified as non-DELIVER-type. Patients with estimated glomerular filtration rate ≤ 25 mL/min/1.73m2 and those receiving SGLT2i treatment were excluded. Echocardiographic variables were obtained pre-discharge and one year after the index day. All-cause mortality and heart failure hospitalization up to one year were determined by web-based electronic record.
The study included 385 subjects with an average age of 83.7 ± 13.9 years, of whom 53.2% were men. The DELIVER-type group had a higher proportion of atrial fibrillation, larger left atrial volume, thicker left ventricular wall, higher levels of the ratio of early diastolic mitral inflow velocity to early diastolic medial mitral annulus velocity (medial mitral E/e'), and higher pulmonary artery systolic pressure (PASP), as well as more evident haemoconcentration and body weight reduction during hospitalization. Kaplan-Meier curve analysis revealed higher rates of all-cause mortality and hospitalization for heart failure at one year in patients with DELIVER-type (Figure 1). In Cox regression analysis, the DELIVER-type subjects had comparable clinical outcomes after accounting for factors such as age, gender, atrial fibrillation, haemoglobin levels, and estimated glomerular filtration rate, compared to non-DELIVER subjects (hazard ratio and 95% confidence interval of mortality [1.62 (0.81-3.25)]). In one-year follow-up, 41.7% of patients shifted from non-DELIVER type to DELIVER-type, but only 14.6% of DELIVER-type subjects had classification shifting.
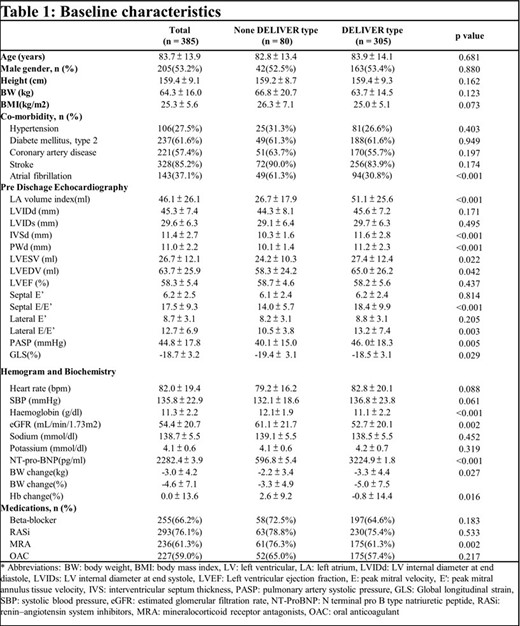
Baseline characteristics
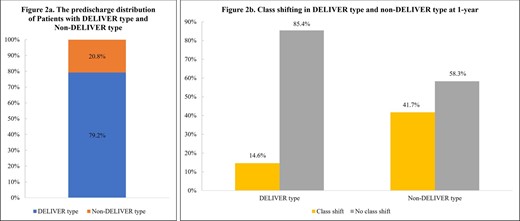
Class shifting in DELIVER type
Author notes
Funding Acknowledgements: None.


{kind=link}