





Abstract
Type of funding sources: None.
Post coronary artery bypass grafting (CABG), coronary angiography (CAG) is the gold standard for graft assessment to check the presence of occlusion or stenosis. Despite this, CAGs after a CABG in the nation are only conducted if patients show ischemic signs. Alternative to CAG, transit time flow measurement (TTFM) can be utilized to determine overall quality of blood flow in grafts. TTFM has yet been utilized to assess graft patency despite its availability in the nation.
This study aims to provide TTFM profiles from CABG surgeries, including characterizing the differences in TTFM parameters between failed and normal grafts, as well as determining the association of TTFM parameters and related clinical factors to the likelihood of graft failure and major adverse cardiac events (MACE).
279 patients were admitted to the cardiology centre from 1 January 2017 to 31 December 2019. Mann-Whitney test was used to compare the differences in TTFM parameters across different graft types, as well as between failed and normal grafts. To determine the likelihood of a graft being normal or failed based on established TTFM parameter cutoffs, χ² test was used. Lastly, multivariate logistic regression was used to determine the association between TTFM parameters and MACE, specifically angina, myocardial infarction, and death.
Different graft types exhibited significant differences in TTFM parameters, particularly pulsatility index (PI) and diastolic filling (%DF). Arterial grafts presented with higher quality of blood flow compared to venous grafts, with left-sided grafts (especially LIMA-LAD) being the graft type of highest quality (Refer to Fig.1).
However, there were no differences in TTFM parameters between failed and normal grafts (PI P = 0.893; DF% P = 0.143). Despite this, there was a greater number of failed grafts with PI > 5 (6.6%) compared to PI < 5 (2.6%) (χ²=4.021, P = 0.045).
Multivariate analysis showed no significant association between TTFM parameters and prevalence of MACE. Instead, an increased risk of graft failure is associated with the female gender (P = 0.031), history of congestive heart failure (P = 0.025) and poor renal function (P = 0.034). Also, an increased risk of MACE is associated with a history of coronary intervention (P = 0.041), left coronary dominance (P = 0.018) and renal function (P = 0.009).
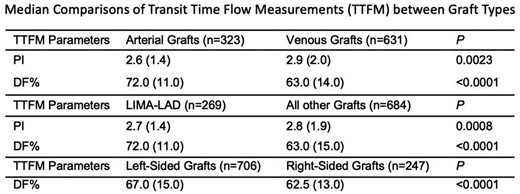
Abstract Figure. Fig1.Median comparison TTFM Parameters
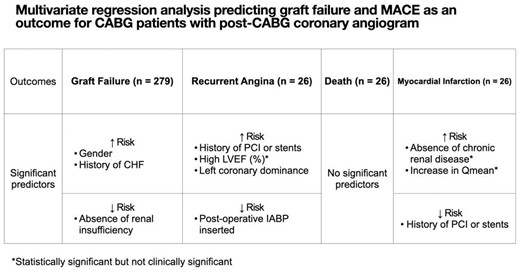
Abstract Figure. Fig2. Multivariate analysis models


{kind=link}