





The ESC and EAPC reference centre for cardiac rehabilitation presents its accelerated programme for cardiac rehabilitation brought about by COVID-19
Introduction
Everyone around the world is experiencing challenging times in dealing with the COVID-19 pandemic. It has impacted personal life as much as it has influenced the way we work. Healthcare systems and healthcare professionals are being tested to the limit and the effects will affect us even long after the acute crisis is passed. It is on the other hand impressive to see how fast healthcare organizations such as hospitals are able to reorganize and develop new ways of communicating and reaching patients through tele-medicine.
Just a few months ago, COVID-19 restrictions were announced in Belgium. Suddenly every non-urgent medical contact needed to be postponed and extra caution was advised for many high-risk patients. This led to the discontinuation of ambulatory cardiac rehabilitation (CR) programmes. In this article, the experience of one of the European Association of Preventive Cardiology (EAPC) accredited CR centres (Heart Centre Hasselt, Jessa Hospital) is described. We hope it can inspire other centres in Europe to adopt new methods in order to reach our CR patients by using digital tools.
The not so distant past
In the pre-corona era, the (cardiac) Rehabilitation and Health centre (ReGo) of the Jessa Hospital was functioning as one of the 56 officially recognized CR centres in Belgium. As with many centres in the country, it is located on hospital premises. Led by EAPC president Paul Dendale the centre quickly grew into a comprehensive and well-organized centre and officially became an ESC centre of reference for CR in 2015, together with the University Hospital of Bern. As of last year, these two centres were the first to obtain EAPC Preventive Cardiology Centre Accreditation for Secondary Prevention and Cardiac Rehabilitation. The classic ambulatory CR programme consists of two to three sessions a week with 45 sessions in total. The centre is highly committed to a multidisciplinary approach. Table 1 illustrates the contribution of the different healthcare professionals working at ReGo.
Overview of the activities of the different healthcare professionals involved in CR
| Specialists | Activities |
|---|---|
| Physiotherapist | Physical assessment, power training, endurance training, balance training, education, physical testing, training schedules |
| Rehabilitation specialist/cardiologist | Medical follow-up, ergo spirometry, education |
| Psychologist | Psychological assessment, follow-up, education, smoking cessation, coping strategies |
| Social worker | Patient referral, psychosocial counselling (e.g. returning to work and home-care), introduction sessions |
| Dieticians | Nutritional assessment, counselling, education, follow-up |
| Researchers | Literature studies, initiating and performing research projects |
| Medical assistant | File management, appointments |
| Specialists | Activities |
|---|---|
| Physiotherapist | Physical assessment, power training, endurance training, balance training, education, physical testing, training schedules |
| Rehabilitation specialist/cardiologist | Medical follow-up, ergo spirometry, education |
| Psychologist | Psychological assessment, follow-up, education, smoking cessation, coping strategies |
| Social worker | Patient referral, psychosocial counselling (e.g. returning to work and home-care), introduction sessions |
| Dieticians | Nutritional assessment, counselling, education, follow-up |
| Researchers | Literature studies, initiating and performing research projects |
| Medical assistant | File management, appointments |
Overview of the activities of the different healthcare professionals involved in CR
| Specialists | Activities |
|---|---|
| Physiotherapist | Physical assessment, power training, endurance training, balance training, education, physical testing, training schedules |
| Rehabilitation specialist/cardiologist | Medical follow-up, ergo spirometry, education |
| Psychologist | Psychological assessment, follow-up, education, smoking cessation, coping strategies |
| Social worker | Patient referral, psychosocial counselling (e.g. returning to work and home-care), introduction sessions |
| Dieticians | Nutritional assessment, counselling, education, follow-up |
| Researchers | Literature studies, initiating and performing research projects |
| Medical assistant | File management, appointments |
| Specialists | Activities |
|---|---|
| Physiotherapist | Physical assessment, power training, endurance training, balance training, education, physical testing, training schedules |
| Rehabilitation specialist/cardiologist | Medical follow-up, ergo spirometry, education |
| Psychologist | Psychological assessment, follow-up, education, smoking cessation, coping strategies |
| Social worker | Patient referral, psychosocial counselling (e.g. returning to work and home-care), introduction sessions |
| Dieticians | Nutritional assessment, counselling, education, follow-up |
| Researchers | Literature studies, initiating and performing research projects |
| Medical assistant | File management, appointments |
ReGo has conducted numerous trials in cardiac telerehabilitation during the last 10 years in collaboration with Hasselt University. Multiple technologies have been used such as pedometers, smartphones, smartwatches, social media, or even wearable sensors. One of the first telerehabilitation trials was the TELEREHAB III trial which demonstrated the effectiveness of the addition of telerehabilitation to standard CR.1,2 The intervention used a combination of monitoring physical activity with a hip-worn pedometer and short messaging service to deliver feedback to the patient. Later, a smartphone application (HeartHab) was developed as a comprehensive patient-tailored app to support cardiac telerehabilitation. HeartHab covers various modules related to CR such as monitoring risk factors (blood pressure, weight, glucose, cholesterol, etc.), medication management, physical activity training, e-coaching via specially designed videos, and symptom monitoring.3
The Sweaty Heart trial was a demonstration project funded by the Erasmus programme of the European Union. In this trial, the Google FIT application was used to monitor the step count of patients. Subsequently, patients received feedback, motivational messages and tips via email based on the step count results.
At the moment, Jessa Hospital is collaborating with Hasselt University in the HORIZON 2020 funded Coroprevention project: an international, multicentre, randomized controlled trial conducted in hospitals in six countries (Germany, Greece, Finland, Italy, Poland, and Portugal,) which will assess the effectiveness of a mobile application-supported nurse-led secondary prevention program for coronary artery disease patients.
Reorganization by force
On 13 March, the Belgian government announced a first wave of measures to limit the further spread of COVID-19 virus. A first measure taken at ReGo that day was the discontinuation of ambulatory rehabilitation for heart failure patients, lung patients, and patients after recent surgery. On the 16 March, the government restrictions were increased even further and ReGo decided to discontinue ambulatory cardiac and pulmonary rehabilitation altogether. Rehabilitation of hospitalized patients (i.e. breathing exercise and mobilization in the room) was continued but with the necessary precautions. Immediately after the closure, all 240 active patients were contacted remotely for a telephone consultation by one of the team members. The goal of this first contact was to explain the current situation, assess the needs of the patient and determine a contact frequency for telerehabilitation. Most patients (75%) agreed to participate remotely and agreed to a weekly follow-up contact. Ever since the closure an additional 86 patients were enrolled in the programme. During telephone consultations, patients receive tailored advice and are guided by different members of the team, depending on their needs. Questions and complaints are discussed at weekly team meetings and follow-up of these questions is mainly done by the cardiologist/rehabilitation specialist, e.g. questions regarding medication and returning to work.
A week after the full closure ReGo launched a series of telerehabilitation videos that patients are referred to during the telephone consultation, i.e. videos on low intensity training, moderate intensity training, balance training, exercise with a home trainer, and breathing exercises. The videos can be viewed on the centre’s website.4 They were viewed about 700 times in the first month.
Early April ReGo expanded the web section with additional online tips and tools for patients to use during the lock-up under the heading: ‘healthy in your house’. Topics are dedicated to nutrition, physical activity, and mental health. About 100 individual patients consulted these pages in the first 2 weeks after the launch.
A further 2 weeks later the CR team started with group sessions using livestreams, on physical activity, dietary advice, psychological support, smoking cessation, and medical advice. Patients are able to ask questions using a chat function or they can speak directly with the healthcare professional when equipped with a microphone. For each session, 5–10 patients are invited to participate. There are one to five streams each week for every topic. An overview of the different measures is illustrated in Figure 1.
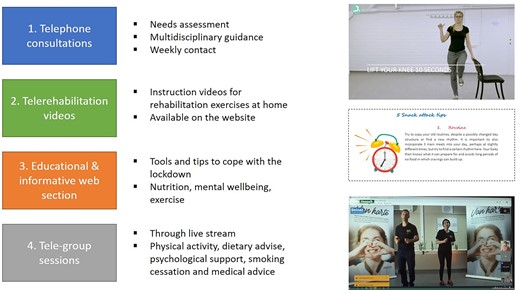
Overview of differentmeasures taken by ReGo to provide telerehabilitation.
Post lockdown: return to the new normal
Ambulatory CR will not be able to completely return to normal for a long time. Hence, the Jessa Hospital will keep performing individual and group sessions through telephone and video consultations in the forthcoming months. Regular rehabilitation will be planned using separate tracks for (possible) COVID positive patients and non-COVID patients, as described in Table 2. The ambulatory rehabilitation will first start with the most urgent patients and those that are not performing any form of (tele-)rehabilitation yet. There will be no more patients allowed than 1 per 15 m2 and they will always be scheduled together with the same group. Besides the regular cardiac and pulmonary rehabilitation, a separate programme will be installed for COVID pathology with persisting respiratory symptoms.
Trajectories for ambulatory CR of COVID positive and COVID negative patients
COVID-positive patients
|
COVID-positive patients
|
Trajectories for ambulatory CR of COVID positive and COVID negative patients
COVID-positive patients
|
COVID-positive patients
|
Dr Martijn Scherrenberg
Hasselt University, Heartcentre Hasselt, Jessa
Hospital Stadsomvaart 11, 3500 Hasselt, Belgium.
Tel: +32 11 33 77 01, email: [email protected]
Kim Bonné, MsC
Revalidatie- en Gezondheidscentrum (ReGo),
Heartcentre Hasselt, Jessa Hospital Stadsomvaart 11, 3500 Hasselt,
Belgium.
Tel: +32 11 33 77 01, email: [email protected]
Prof. Dr Paul Dendale
EAPC president, Hasselt University,
Heartcentre Hasselt, Jessa Hospital Stadsomvaart 11, 3500 Hasselt,
Belgium.
Tel: +32 11 33 70 73, email:[email protected]
Conflict of interest: none declared.
References
References are available as supplementary material at European Heart Journal online.





{kind=link}