





Abstract
In recent guidelines, non-invasive imaging techniques play a pivotal role in the management of chronic coronary syndrome (CCS). The elderly represent a large percentage of our routine CCS population and risk stratification in this scenario is challenging. The potential of vasodilator stress cardiovascular magnetic resonance (vs-CMR) for this purpose is unknown.
We explored the prognostic value of the ischemic burden, as derived from vs-CMR, in elderly patients with known or suspected CCS.
From the general cohort of 6389 patients with known or suspected CCS submitted to undergo vs-CMR in our health department from 2001 to 2016, we performed a subanalysis of the 1225 patients >70 year-old (mean age 77±5 years, 51% male). Clinical and vs-CMR characteristics were prospectively recorded. The ischemic burden (at stress first-pass perfusion imaging) was computed (using the 17-segment model). The occurrence of major adverse cardiac events (MACE) defined as all-cause death and/or non-fatal myocardial infarction (whichever occurred first) was retrospectively revised using the electronic regional health system registry.
During a median follow-up of 2.7 years, 203 MACEs were registered (17%). Age (77±4 vs. 76±5 years) was not significantly different in patients with and without MACE. Larger left ventricular (LV) end-diastolic and end-systolic volume indexes, more depressed LV ejection fraction, more extensive areas with late gadolinium enhancement and ischemic burden were detected in patients with MACE (p<0.001 for all comparisons). In non-revascularized patients (n=1118), the MACE rate ranged from 13% (in patients with 0–1 ischemic segments) to 35% (in those with >8 ischemic segments, p<0.001 for the trend). In the small subset of revascularized patients (n=107), revascularization exerted a non-significant protective effect only in patients with extensive ischemic burden (>5 segments).
Vasodilator stress CMR represents a valuable tool to stratify risk in elderly patients with known or suspected CCS and might be helpful to guide decision-making.
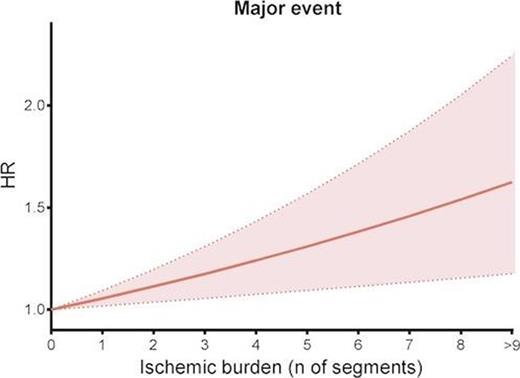
Figure 1
Type of funding source: None


{kind=link}