





Abstract
To assess if the dental follicle volume of palatally impacted canines (PICs) affects the relative root position of the adjacent lateral incisors (LIs) and first premolars (FPs).
A retrospective cross-sectional study of 49 patients with unilaterally PICs with dental follicles who had CBCT imaging previously taken. Four orthodontic centers in different countries provided the sample. A mean difference of 5° between the angular measurements (mesiodistal tip, buccolingual inclination, or mesiodistal rotation) of the LI and FP adjacent to the PIC and the controls was considered clinically relevant. A value of 0.05 was set for significance level and a power of 80%. The minimum sample size was determined to be 26 patients. These patients were further assigned to an LI sample (n = 49) and an FP sample (n = 23), dependent on the direct contact of the dental follicle to that adjacent tooth. A manual segmentation technique was used to obtain the volumetric measurements of the dental follicle. Angular measurements of adjacent teeth were then compared to the contralateral nonimpacted side, which acted as the control. A multivariant regression analysis was performed using IBM SPSS software, and statistical significance was set at α = 0.05.
Adequate intra-rater reliability was accomplished. The multivariant regression analysis implied that there is no difference in the mean change in the tip, torque, and rotation of the LI and FP between the impacted and control sides when dental follicle volumes are considered (P = .509 for the LI sample and P = .804 for the FP sample).
CBCT imaging of dental follicle border delimitations, partial volume effect, and scattering are limitations. This is a convenience sample where the FP subsample is small.
The dental follicle volume of the PICs does not seem to influence the relative position of the adjacent LI and FP mesiodistal tip, buccolingual inclination, and mesiodistal rotation. Early intervention could have been suggested to avoid certain malocclusion traits if significant displacements were demonstrated.
Introduction
The maxillary cuspids act as the cornerstones of the upper dental arch, providing the esthetics to create a harmonious smile and ideal function to ensure canine guidance during excursive jaw movements protecting the posterior dentition. In the average individual, the maxillary canines generally erupt around 11.5 years [1]. A tooth impaction occurs when a tooth fails to erupt into the oral cavity and deviates from the normal eruption pattern and timing. The maxillary cuspids are the most frequently impacted teeth following the maxillary/mandibular third molars, occurring in approximately 0.92%–2.2% of the population and are more commonly seen in females 3–4 times as much as males with a ratio of 3:1 [2–4]. Maxillary impacted canines are more often palatally displaced than buccally displaced canines at a ratio of 6:1 and typically present as unilateral impactions, as 17%–45% of palatally impacted canines (PICs) cases present as bilateral impactions [5, 6]. The etiology of maxillary impacted canines is still a debated topic. Considering other contributing factors such as local obstruction and/or pathology, two main theories describe the etiopathogenesis of maxillary impacted canines. Failure to identify and treat impacted maxillary canines can lead to many undesirable outcomes, including displacement, and resorption of the neighboring teeth, canine ankylosis and resorption, dentigerous cyst formation, and recurrent infections. Subsequently, this could compromise tooth vitality and supporting structures such as the periodontium and alveolar bone [7, 8].
The dental follicle comprises a fluid-filled, loose connective tissue sac surrounding the crown of the developing tooth, acting as a source of osteoblasts, cementoblasts, and fibroblasts that aid in forming the periodontium surrounding the dentition. It also initiates the resorptive process of the deciduous tooth root and surrounding bone, which creates the eruption path for the underlying permanent dentition [7]. The previous areas of dental follicular investigation concerning impacted canines primarily focused on root resorption of the adjacent incisors utilizing computed tomography imaging. It was seen that the follicle of the canine does not cause root resorption of the adjacent incisors but is most likely a result of the physical contact of the canine and the incisor, as well as the eruption process of the canine. This was believed to be the reason for the deviation of the adjacent root positions but was not confirmed by the study mentioned above [9–11].
To date, no studies have focused on the relationship between the dental follicle of PICs and the effect on the position of the adjacent teeth. There also have been no studies that have focused on the volumetric measurement of the dental follicle of maxillary canines as they have traditionally been based on a linear measurement in millimeters from the crown of the canine to the periphery of the dental follicle, whether it is 2D imaging or CBCT. With the compressive forces created by the dental follicle during tooth eruption, which could subsequently displace the adjacent teeth roots, this is a unique perspective on the potential effects of the impacted maxillary canine and its associated dental follicle. This could warrant early intervention to manage dental follicles to avoid certain malocclusion traits.
Methods
Ethics approval was granted by each one of the universities from where the samples were collected (Lead university - University of Alberta - Pro00087314).
Sample selection
Data collection for this retrospective cross-sectional study was obtained from a pool of available pretreatment CBCT records of patients with unilateral PICs, where the contralateral normally erupted canine was designated as the control. These records were obtained from four different reference centers:
The University of Alberta Faculty of Medicine and Dentistry - Graduate Orthodontic Clinic (Canada)
Universita degli Studi della Campania Luigi Vanvitelli - Diparmento Multidisciplinare di Specialità Medico-Chirurgiche e Odontoiatriche (Italy)
The Hebrew University - Hadassah School of Dental Medicine (Israel), and the
University of Gothenburg - Sahlgrenska Academy - Department of Orthodontics (Sweden)
The final sample was selected based on the following eligibility criteria:
Inclusion criteria
Unilateral PIC with the presence of the dental follicle.
The dental follicle of the palatally impacted maxillary canine contacting the lateral incisor (LI) and/or the FP.
LI and FP teeth that are fully erupted.
Theontralateral canine fully erupted.
Optimal CBCT imaging includes the maxilla and both impacted and normally erupted contralateral canine and adjacent teeth.
Exclusion criteria
◦ Diagnosed craniofacial congenital anomalies or syndromes.
◦ Pathologies associated with impacted canine or adjacent teeth.
◦ Patients who have reported significant facial trauma.
◦ Previous orthodontic treatments that affect the position of the maxillary dentition.
Sample size calculation
Based on the study by Dekel et al. [12], a mean difference of 5° between the angular measurements of the LI and FP adjacent to the PIC and the controls was considered clinically relevant. From their pilot study, a standard deviation of 6.4° was considered clinically relevant. In other words, the smallest standard deviation to be considered clinically significant when analyzing the potential impact of the dental follicle volume over the adjacent teeth (for any mesiodistal tip, buccolingual inclination, and mesiodistal rotation) was 5°. Any difference smaller than that in any direction was considered not clinically relevant. A value of .05 was set for significance level and a power of 80%. The minimum sample size was determined to be 26 patients.
The scans were taken with a voxel size of 0.25–0.4 mm3 over 2–8.9 s (75–120 kVp; 5 mA) and included the field of view that captured the maxilla and dentition of interest to allow for proper measurements in the study. Three authors measured the stated variables independently after the calibration.
Segmentation of the dental follicle
For this study, volumetric segmentation of the dental follicle of the PIC was performed using the open-source software OsiriX DICOM Viewer (version 13.01). This imaging software has been used in studies involving both the dental and medical fields for volumetric analysis [13–15]. The DICOM files of each patient were obtained and imported into OsiriX, and a manual segmentation process was employed. The decision to use a manual segmentation process was due to the dental follicle's soft tissue nature and the inability of automated processes to discern the borders of the dental follicle. This would often cause the seed voxel to connect undesirable areas and leak into the surrounding structures, such as the oral cavity or other less radiopaque structures. Previous studies had implemented these segmentation techniques on hard tissue structures such as dentition, which had more clarity regarding structural mass and borders. Before the segmentation of the dental follicle, it was determined that the sagittal view of the CBCT provided the clearest view of the dental follicle in relation to the crown of the impacted canine. The axial and coronal views were later used to confirm the accuracy of the segmentation. Manual segmentation involved utilizing tools within OsiriX such as “paintbrush,” “pencil,” and “repulsor” to freehand trace the voxels that generated the dental follicle to highlight the region of interest (referred to as “ROI” on OsiriX). This was repeated for each DICOM image slice-by-slice until the entire dental follicle was captured into the ROI in which the 3D model would be rendered. The crown of the impacted canine was excluded from the ROI to determine the true volume of the dental follicle.
Measurement of the dental follicle
To obtain the measurement of the dental follicle volume, the entire ROI must be established from the DICOM images containing the desired portion, as mentioned in the previous steps. Because a voxel is an isotropic 3D element represented as a cube or box, any voxel highlighted in the ROI will highlight the volume in the sagittal view and the axial and coronal views of the CBCT. In Fig. 1, the area is generated for each slice, as seen in the label indicating that the area is 39.01 mm2, and the volume can be calculated by compiling each slice containing the ROI. The ROI function is accessed in the toolbar where the “ROI Volume” and the “Compute Volume” options can be selected. The volume of the ROI will then be generated in cm3 units. This can be seen in Fig. 2.
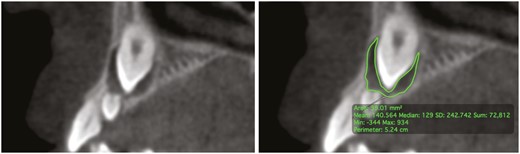
Segmentation of the dental follicle of the maxillary impacted canine using OsiriX DICOM Viewer in the sagittal view of the CBCT. This tracing method was manually repeated and refined for each slice of the DICOM containing the dental follicle.

Completed 3D rendering of the dental follicle of the impacted maxillary canine with the associated volumetric calculation. The photo shows that the dental follicle has a 0.2525 cm3 or 252.5 mm3 volume.
Measurement of the relative position of the adjacent teeth
Establishment of the palatal reference plane
Based on the methodology used by Dekel et al. [12], the palatal plane was used as the reference plane to measure the angular tip, torque, and rotation of the adjacent LI and FP. The palatal plane acts as a stable reference point that can be standardized in the axial, coronal, and sagittal views based on a line that runs through the anterior nasal spine (ANS) to the posterior nasal spine (PNS).
Measurement of the relative position of the lateral incisor
Utilizing the palatal plane as the reference point, the LI adjacent to the PIC and the control side were measured, shown in Fig. 3 and are as follows:
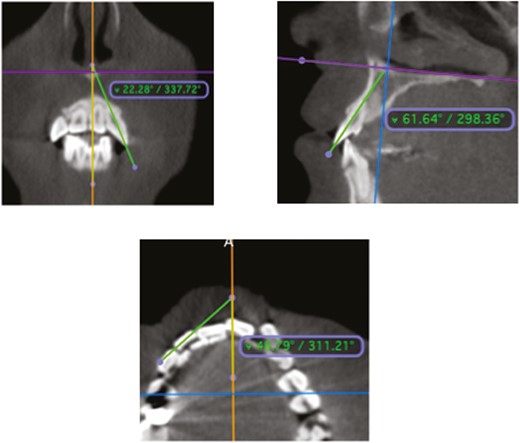
Multiplanar reconstruction views demonstrate the lateral incisor’s angular measurements. (a) Mesiodistal tip, (b) buccolingual inclination, and (c) mesiodistal rotation.
Mesiodistal tip—measured in the coronal view—the angle between the long axis of the LI and mid-palatal plane (yellow line).
Buccolingual inclination—measured in the sagittal view—the angle between the long axis of the LI and palatal plane (purple line).
Mesiodistal rotation—measured in the axial view—the angle between a tangent bisecting the most prominent mesiodistal contour (parallel to the facial surface) of the LI and the mid-palatal plane (yellow line).
Measurement of the relative position of the first premolar
Utilizing the palatal plane as the reference point, the FP adjacent to the PIC and the control side were measured, shown in Fig. 4 and are as follows:
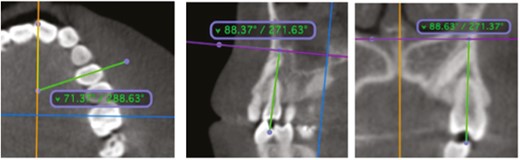
Multiplanar reconstruction views demonstrating the angular measurements of the first premolar. (a) Mesiodistal tip, (b) buccolingual inclination, and (c) mesiodistal rotation.
Mesiodistal tip—measured in the sagittal view—the angle between the long axis of the FP and palatal plane (purple line).
Buccolingual inclination—measured in the coronal view—the angle between the long axis of the FP and mid-palatal plane (yellow line).
Mesiodistal rotation—measured in the axial view—is the angle between a tangent bisecting the buccolingual surface of the FP and the mid-palatal plane (yellow line).
Statistical analysis
Ten randomly selected patients for intra-rater and six for inter-rater reliability were randomly selected from a collected sample pool of 49 patients to determine the method reliability for measuring the dental follicle volume of the impacted maxillary canine. A two-way mixed model intraclass correlation coefficient (ICC) was used to measure agreement between the measurements by the raters [16]. A multivariant regression analysis was used to test the study hypothesis. Statistical analysis was performed using IBM SPSS Statistics for Apple Mac OS (Version 28). The significance level was set to α = 0.05 for all statistical analyses. ICC reliability with a 95% confidence interval (CI) is classified as poor (ICC < 0.50), moderate (0.50 < ICC < 0.75), good (0.75 < ICC < 0.90), and excellent (ICC > 0.90) reliability [16].
Results
Reliability of measurements
The intra-rater ICC for the volumetric measurement of the dental follicle, LI and FP mesiodistal tip, buccolingual inclination, and mesiodistal rotation were all larger than 0.861, with the lowest confidence interval at 0.734. The percent measurement error was less than 10% for all variables except rotation of impacted canine (up to 22.4%—3.3°).
The inter-rater ICC for the volumetric measurement of the dental follicle, LI and FP mesiodistal tip, buccolingual inclination, and mesiodistal rotation were all larger than 0.876, with the lowest confidence interval at 0.707. The percent measurement error was less than 11.4% for all variables.
Overall results
Forty-nine patients with previous CBCT records were assessed for this study. Descriptive statistics can be observed in Table 1.
Descriptive statistics of the volumetric measurements of the dental follicle and angular measurements of the mesiodistal tip, buccolingual inclination, and mesiodistal rotation of the adjacent lateral incisor and first premolar.
| Measurements | N | Mean | Minimum | Maximum | Standard deviation | 95% CI (lower) | 95% CI (upper) |
|---|---|---|---|---|---|---|---|
| Dental follicle volume (mm3) | 49 | 279.6 | 110.7 | 704.1 | 128.9 | 242.5 | 316.6 |
| Lateral incisor tip difference (°) | 49 | 5.6 | −14.7 | 27.1 | 10.1 | 2.7 | 8.5 |
| Lateral incisor torque difference (°) | 49 | 8.6 | −10.6 | 44.2 | 8.7 | 6.1 | 11.1 |
| Lateral incisor rotation difference (°) | 49 | −11.6 | −54.9 | 13.2 | 14.2 | −15.9 | −7.9 |
| First premolar tip difference (°) | 23 | −0.6 | −12.0 | 16.1 | 7.8 | −4.0 | 2.7 |
| First premolar torque difference (°) | 23 | −1.2 | −10.0 | 18.0 | 6.5 | −4.0 | 1.6 |
| First premolar rotation difference (°) | 23 | 3.5 | −24.1 | 37.1 | 15.2 | −3.1 | 10.1 |
| Measurements | N | Mean | Minimum | Maximum | Standard deviation | 95% CI (lower) | 95% CI (upper) |
|---|---|---|---|---|---|---|---|
| Dental follicle volume (mm3) | 49 | 279.6 | 110.7 | 704.1 | 128.9 | 242.5 | 316.6 |
| Lateral incisor tip difference (°) | 49 | 5.6 | −14.7 | 27.1 | 10.1 | 2.7 | 8.5 |
| Lateral incisor torque difference (°) | 49 | 8.6 | −10.6 | 44.2 | 8.7 | 6.1 | 11.1 |
| Lateral incisor rotation difference (°) | 49 | −11.6 | −54.9 | 13.2 | 14.2 | −15.9 | −7.9 |
| First premolar tip difference (°) | 23 | −0.6 | −12.0 | 16.1 | 7.8 | −4.0 | 2.7 |
| First premolar torque difference (°) | 23 | −1.2 | −10.0 | 18.0 | 6.5 | −4.0 | 1.6 |
| First premolar rotation difference (°) | 23 | 3.5 | −24.1 | 37.1 | 15.2 | −3.1 | 10.1 |
Descriptive statistics of the volumetric measurements of the dental follicle and angular measurements of the mesiodistal tip, buccolingual inclination, and mesiodistal rotation of the adjacent lateral incisor and first premolar.
| Measurements | N | Mean | Minimum | Maximum | Standard deviation | 95% CI (lower) | 95% CI (upper) |
|---|---|---|---|---|---|---|---|
| Dental follicle volume (mm3) | 49 | 279.6 | 110.7 | 704.1 | 128.9 | 242.5 | 316.6 |
| Lateral incisor tip difference (°) | 49 | 5.6 | −14.7 | 27.1 | 10.1 | 2.7 | 8.5 |
| Lateral incisor torque difference (°) | 49 | 8.6 | −10.6 | 44.2 | 8.7 | 6.1 | 11.1 |
| Lateral incisor rotation difference (°) | 49 | −11.6 | −54.9 | 13.2 | 14.2 | −15.9 | −7.9 |
| First premolar tip difference (°) | 23 | −0.6 | −12.0 | 16.1 | 7.8 | −4.0 | 2.7 |
| First premolar torque difference (°) | 23 | −1.2 | −10.0 | 18.0 | 6.5 | −4.0 | 1.6 |
| First premolar rotation difference (°) | 23 | 3.5 | −24.1 | 37.1 | 15.2 | −3.1 | 10.1 |
| Measurements | N | Mean | Minimum | Maximum | Standard deviation | 95% CI (lower) | 95% CI (upper) |
|---|---|---|---|---|---|---|---|
| Dental follicle volume (mm3) | 49 | 279.6 | 110.7 | 704.1 | 128.9 | 242.5 | 316.6 |
| Lateral incisor tip difference (°) | 49 | 5.6 | −14.7 | 27.1 | 10.1 | 2.7 | 8.5 |
| Lateral incisor torque difference (°) | 49 | 8.6 | −10.6 | 44.2 | 8.7 | 6.1 | 11.1 |
| Lateral incisor rotation difference (°) | 49 | −11.6 | −54.9 | 13.2 | 14.2 | −15.9 | −7.9 |
| First premolar tip difference (°) | 23 | −0.6 | −12.0 | 16.1 | 7.8 | −4.0 | 2.7 |
| First premolar torque difference (°) | 23 | −1.2 | −10.0 | 18.0 | 6.5 | −4.0 | 1.6 |
| First premolar rotation difference (°) | 23 | 3.5 | −24.1 | 37.1 | 15.2 | −3.1 | 10.1 |
The results of the multivariant regression analysis for the LI sample (n = 49; P = .509 with the outliers and P = .110 without the outliers) and for the FP sample (n = 23; P = .804 with the outliers and P = .892 without the outliers) suggest that there is insufficient evidence to reject the null hypotheses (the compressive forces created by the dental follicle during tooth eruption displace the adjacent teeth); therefore, the differences are not statistically significant.
Discussion
This study aimed to assess how the volume of the dental follicle of the PIC affects the relative position (mesiodistal tip, buccolingual inclination, and mesiodistal rotation) of the adjacent LI and FP. The potential of hydraulic pressure created by the dental follicle content during tooth eruption could potentially displace the adjacent teeth. This is a unique perspective on the potential effects of the PIC and its associated dental follicle. If significant displacements were to be demonstrated, it could warrant early intervention to manage dental follicles to avoid certain malocclusion traits. This was performed by assessing previous CBCT records of patients with unilaterally PICs with OxiriX DICOM Viewer. The collected samples were separated into the LI and FP groups based on actual physical contact of the dental follicle to either or both adjacent teeth. To our knowledge, no studies have directly evaluated the dental follicle in this manner.
Previous studies have generally focused on the radiographic characteristics of the dental follicle and its association with root resorption in the adjacent teeth. Ericson and Bjerklin [11] mentioned that they believe the deviation in adjacent root position is most likely due to the eruptive force of the canine and not by the dental follicle itself. However, they also indicated that they could not confirm if widened dental follicles during maxillary canine eruption increase the risk of adjacent incisor root displacement. A year later, in a CBCT study [17], the same authors focused on whether the dental follicle of the impacted maxillary canines causes root resorption of the neighboring LI based on the dental follicle's width, shape, and proximity. They concluded that there was a significant relationship to be found among those variables of the dental follicle. However, they did conclude that the dental follicle of the maxillary impacted canine caused root resorption of the deciduous canine. Chaushu et al. [18] found that female patients (4.2 times) with enlarged dental follicles wider than 2 mm (8.3 times) and normal LI (5.8 times) were more at risk for severe incisor root resorption. Dagsuyu et al. [19] found that the largest statistically significant dental follicle size (3.51 mm ± 1.19 mm) of maxillary impacted canines was found to be more common in mild resorption (up to half the dentin thickness) cases in the adjacent LIs. Interestingly, the dental follicle size was smaller in moderate resorption (2.60 mm ± 0.60 mm) and severe resorption (2.91 mm ± 1.35 mm), where the resorption encroaches or perforates the pulp. However, they also concluded that they could not confirm that increased dental follicle widths correlate with an increased risk of resorption on the adjacent LI. It is important to note that each of these studies assessed the width of the dental follicle measured as the largest distance from the crown of the maxillary canine to the periphery of the dental follicle on axial CBCT slices. Our study, focusing on overall dental follicle volume, suggested that the volume of the dental follicle of the PIC does not affect the relative position of the adjacent LI and FP.
The LI sample results suggest insufficient evidence (P = .509 with the outliers and P = .110 without the outliers) to reject the null hypothesis; therefore, the differences are not statistically significant. In other words, there is no difference in the change of mesiodistal tip, buccolingual torque, and mesiodistal rotation of the adjacent LI between the impacted and control sides when comparing the volume of the dental follicle as it contacts the LI. Based on the tip, torque, and rotation angular of the adjacent LI, it appears that the data was consistent with the findings of Dekel et al. [12], as the LI had exhibited an overall trending distal crown tip/mesial root tip, palatal crown torque/buccal root torque, and mesiobuccal rotation on the PIC in comparison with the control side without considering the dental follicle. This was also consistent with Liuk et al. [20], who found that the adjacent LI was retroclined and mesiobuccally rotated. However, their findings did not show the mesial root tip seen in our samples or the samples of Dekel et al. [12].
The FP sample results suggest insufficient evidence (P = .804 with the outliers and P = .892 without the outliers) to reject the null hypothesis; therefore, the differences are not statistically significant. In other words, there is no difference in the change of mesiodistal tip, buccolingual torque, and mesiodistal rotation of the adjacent FP between the impacted and control sides when comparing the volume of the dental follicle as it contacts the FP. No general trend was seen in the tip, torque, or rotation when comparing the impacted and control sides without considering the dental follicle. This was inconsistent with Dekel et al. [12], who found that the PIC had caused a mesiobuccal rotation and buccal root torque of the FP dependent on the degree of impaction relative to the FP.
Our samples showcased clear contact of the dental follicle with the LI and/or FP without the physical contact of the crown, which allowed us to assess any involvement of the dental follicle and its associated volume on root displacements. Given that our results suggested no statistical significance in the difference of the relative position of the adjacent LI and FP with the dental follicle volume of the impacted canine compared with the control side, our findings may suggest that the physical contact of the crown of the canine with the neighboring root may be a crucial factor in tooth displacement. As the dental follicle expands, it is noted that the vector of expansion moves toward the path of least resistance. It was seen that the follicle would enlarge toward the palate but more often asymmetrically toward the inter-radicular regions between the adjacent LI and FP. Another factor to consider is if the impacted canine was currently undergoing eruption or was stagnant in position, as the propulsive eruptive mechanism could exert pressure to displace the adjacent teeth. As with most biological/physiological events in the human body, these are multifactorial. Expecting a single factor to be the main culprit is not necessarily fair. Nevertheless, the hydraulic pressure hypothesis was not fully supported.
With future research, it would be interesting to consider analyzing the dental follicles that fall into the extremely large ranges of volumetric measurements seen in this study. Perhaps a threshold volume must be exceeded to create a notable effect on the adjacent teeth' positions. Only 4 of the 49 patient CBCT records gathered for this research project had a dental follicle volume that surpassed 450 mm3. The dental follicle measured from the widest portion spanning from the crown of the maxillary canine to the periphery of the dental follicle measured 2.80 mm on average (based on the axial view of the CBCT), which is within the normal range and negates any suspicion of pathology (i.e. dentigerous cyst).
Another scenario that could be further analyzed includes the angular position of the adjacent central incisor (CI), which was not considered in the present project. Previous studies showed that the CI that is ipsilateral to the maxillary impacted canine is at risk of root resorption to a lesser extent than that of the adjacent LI. Ericson et al. [21] found that 38% of LI and 9% of CI had exhibited root resorption in direct contact with the ectopically erupted maxillary canine for their sample. Chaushu et al. [18] also noted that out of their 96 severely resorbed (at least 1/3 of the root resorbed) maxillary incisor samples, 69 LI and 27 CI were resorbed (2.5:1 ratio). With these findings, it would be interesting to see if there are any pathognomonic changes to the angular position of the CI to the maxillary impacted canine.
Finally, Chaushu et al. [18] reported that impacted maxillary canines with enlarged dental follicles could cause increased severe root resorption. Based on our study results, another factor may be that the enlarged dental follicles do not displace the roots of the laterals. This implies that those large follicles and their content get close to the LI's root and surround them. The combination of these two factors should be investigated in the future.
Limitations
The three investigators measuring the variables had trouble discerning the borders of the dental follicle on the CBCT slices. Many CBCT-related factors play a role in the quality of the image generated, including voxel size, image artifacts, tube current and voltage, fields of view, and imaging software. Voxel sizes of 0.25 mm—0.4 mm were used for the included samples, which may not be accurate or precise enough to capture the details of the dental follicle and surrounding structures. CBCT acquisition parameters can be improved by increasing tube output and exposure time; however, the as low as reasonably achieved (ALARA) principle, as recommended by the ADA and FDA, should be followed to ensure patient safety, where the benefits and risks must be weighed against each other [22, 23].
An essential factor of particular interest that influences the spatial resolution of CBCT images is the partial volume effect/averaging (objects or boundaries of differing densities are less than the size of the voxel). This can lead to an artificial inaccuracy in the resultant volume depending on the structure of interest, which is crucial in our study as the dental follicle of the impacted canines is adjacent to radiodense structures, such as the enamel of the maxillary canine crown and the bone of the maxillary alveolus.
Another factor influencing the spatial resolution of CBCT images is scatter caused by unwanted photons diffracting from their original path after interacting with matter, also known as noise. This noise can affect the density values of different tissues, inflating volumetric measurements. CBCT scans are more prone to scatter than medical CTs and are reduced by decreasing the field of view to capture the ROI [22].
The FP sample size is below the ideal calculated (23 instead of 26).
Ideally, a control group with rotations greater than 5° for both FP and LI samples could have been used to verify that the dental follicle was the sole causative factor. This should be considered in future related studies.
The retrospective nature of the sample selection could generate bias as it is a convenience sample.
Conclusions
There is no statistical difference in the change of mesiodistal tip, buccolingual inclination, and mesiodistal rotation of the adjacent LI between the impacted and control maxillary canine sides when comparing the volume of the dental follicle as it contacts the LI.
There is no statistical difference in the change of mesiodistal tip, buccolingual inclination, and mesiodistal rotation of the adjacent FP between the impacted and control maxillary canine sides when comparing the volume of the dental follicle as it contacts the FP. However, it is important to note that the sample size of the FP is smaller than the required sample size.
The clinical importance of this study is related to the potential that the hydraulic pressure created by the dental follicle content during tooth eruption could potentially displace the adjacent teeth. If significant displacements were demonstrated, early intervention could have been warranted to manage dental follicles to avoid certain malocclusion traits.
Author Contributions
Michael Lam (Conceptualization [Lead], Data curation [Lead], Formal analysis [Lead], Methodology [Lead], Project administration [Lead], Resources [Equal], Validation [Equal], Writing – original draft [Lead], Writing – review & editing [Lead]), Eyal Dekel (Conceptualization [Lead], Data curation [Equal], Formal analysis [Equal], Methodology [Lead], Resources [Lead], Software [Lead], Validation [Equal], Writing – review & editing [Supporting]), Ludovica Nucci (Conceptualization [Supporting], Data curation [Equal], Methodology [Supporting], Resources [Lead], Validation [Equal], Writing – review & editing [Supporting]), Vicenzo Grassia (Data curation [Supporting], Methodology [Supporting], Validation [Supporting], Writing – review & editing [Supporting]), Julia Naoumova (Resources [Lead], Writing – review & editing [Lead]), Camila Pachêco-Pereira (Formal analysis [Supporting], Methodology [Equal], Software [Lead], Writing – review & editing [Lead]), Letizia Perillo (Conceptualization [Supporting], Methodology [Supporting], Resources [Supporting], Supervision [Supporting], Writing – review & editing [Supporting]), Stella Chaushu (Conceptualization [Lead], Formal analysis [Equal], Methodology [Lead], Resources [Supporting], Supervision [Supporting], Writing – review & editing [Equal]), and Carlos Flores-Mir (Conceptualization [Lead], Data curation [Equal], Formal analysis [Equal], Methodology [Equal], Project administration [Lead], Supervision [Lead], Writing – original draft [Lead], Writing – review & editing [Lead])
Conflict of interest
None declared by any of the authors.
Data availability
Some of the data would be available upon request.
References
Author notes
Michael Lam, Eyal Dekel, and Ludovica Nucci Equal contribution.


{kind=link}
{kind=link}
{kind=link}
{kind=link}