






Abstract
Three consecutive male patients underwent videoscopic supradiaphragmatic thoracic duct division using the Harmonic Scalpel with a hook blade (Ethicon Endo-Surgery, Cincinnati, OH, USA) for treatment of chyle leaks that developed after left upper lobectomy, graft replacement of a descending aortic aneurysm and thyroidectomy with concomitant partial sternal resection. The thoracic duct was exposed and divided using just the Harmonic Scalpel. The operations lasted 40, 20 and 18 min. No mortality, morbidity or recurrence occurred during follow-up periods of 27, 17 and 9 months. The Harmonic Scalpel with a hook blade can facilitate supradiaphragmatic exposure of the thoracic duct.
1 Introduction
Although rare, chylous leaks occur after thoracic or cervical surgery when the thoracic duct has sustained injury. Surgical treatment, i.e. thoracic duct ligation or division, is carried out for patients who do not respond to conservative therapy [1]. Currently, thoracoscopy is a viable, minimally invasive approach for this procedure [2]. We have been using an ultrasonic coagulator to facilitate thoracoscopic exposure of the thoracic duct at the supradiaphragmatic level and describe below our surgical technique and outcomes.
2 Patients and surgery
A 70-year-old man underwent left upper lobectomy and mediastinal lymph-node dissection for lung cancer, a 66-year-old man had a graft replacement of a descending aortic aneurysm through a left thoracotomy and a 55-year-old man with thyroid cancer and sternal metastasis underwent thyroidectomy and concomitant partial resection of the sternum. Immediately after surgery, each patient developed persistent and copious chylous leakage through the drainage tubes placed in the left thorax or the neck wound, and conservative management, i.e. prohibition of oral nutrition and administration of parenteral hyperalimentation, was commenced. However, each patient continued to discharge 1–1.5 l chyle daily and therefore, surgical management was performed 8, 9 and 11 days after starting conservative care. The lymphangiographic study was not performed preoperatively in each case.
A left upper lobectomy case had undergone mediastinal lymph node sampling, involving deep subcarinal nodes. Moreover, he had a comorbidity of obesity-related poor pulmonary reserve. In a descending aortic graft replacement case, an aortic aneurysm was significantly curved and sifted to the right side. In a cervical chylous leakage case, direct closure of the leak site was performed under local anesthesia, but it failed. The patient's neck wound tissue became significantly edematous due to inflammation, and it seemed difficult to accomplish accurate dissection, identification and ligation of the cervical duct above the leak point. Therefore, re-entry of a left thoracotomy or reoperation in the neck wound was avoided and the present right thoracoscopy approach was instead selected in each case.
All patients were intubated with a double-lumen endotracheal tube for selective left-lung ventilation. After heavy cream was administered via a nasogastric tube, each patient was placed in the left lateral position and a right hemithorax was prepared. Three 5-mm ports were placed for the procedure: the first port for the 5-mm, 30°, rigid thoracoscope (Olympus, Tokyo, Japan) was placed at the eighth intercostal space (ICS) on the mid-axillary line, the second for an endoscopic Kitner dissector (BTD-5, Ethicon Endo-Surgery, Cincinnati, OH, USA) and the third for a 5-mm hook blade of the Harmonic Scalpel (DH 085, Ethicon Endo-Surgery) or an endoscopic clip applier (DCS 12, Ethicon Endo-Surgery) were placed at the sixth and seventh ICSs on the posterior axillary line, respectively. After the right lung had collapsed, the pulmonary ligament was dissected from the mediastinum and the thoracic duct was exposed at the supradiaphragmatic level using the Harmonic Scalpel (Fig. 1, top) . The exposed duct was ligated with the endoscopic clip and divided using the Harmonic Scalpel (Fig. 1, bottom).
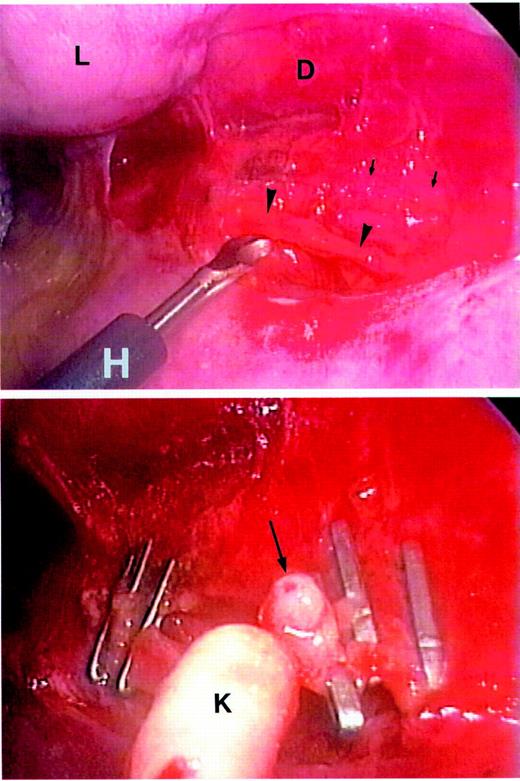
Thoracoscopic view of thoracic duct exposure and division. (Top) The thoracic duct (arrowheads) exposed by a hook blade of the Harmonic Scalpel (H). Arrows indicate vagal nerve. D, descending aorta; L, lung. (Bottom) The divided thoracic duct showing its tubular appearance (arrow). K, endoscopic Kitner dissector.
3 Results
No procedure-related mortality or morbidity ensued. The operations lasted 20 and 18 min for the patients who had undergone lobectomy and thyroidectomy, respectively. It took a little longer (40 min) for the patient who had undergone graft replacement of an aortic aneurysm. All patients had negligible blood loss. Each patient's chylous leakage ceased immediately and their drainage tubes were removed on the first or second postoperative day. As of January 2002, these three patients had been followed up for 27, 17 and 9 months and suffered no recurrence of the chyle leaks.
4 Discussion
The incidence of traumatic chylous leakage after cardiothoracic procedures remains low, in the range of 0.3–0.5% [3]. In the literature, most authors describe that, initially at least, this complication should be managed nonoperatively [4,5]. However, most surgery-related chyle leaks require surgical management [6]. Since it was first described by Lampson in 1948 [7], supradiaphragmatic duct ligation through the right thorax has been recommended by numerous authors.
Although the incidence is unknown, an accessory duct may lie beside the main trunk, because the available pathways were embryologically bilateral and the final course of the thoracic duct is subject to considerable variation [8]. Therefore, the posterior mediastinal space surrounded by the azygos vein, esophagus and descending aorta should be dissected carefully to enable the whole thoracic duct system to be uncovered at the supradiaphragmatic level.
The Harmonic Scalpel generates less heat (below 100 °C) and minimal smoke. Therefore, this device enables gentle tissue dissection with minimal thermal injury and a clear, smokeless endoscopic view. The hook blade was useful in the present technique: the hook with a sharp edge was used to hook and divide the pulmonary ligament and mediastinal pleura, and thereafter the blunt tip of the blade was used to dissect the thoracic duct from the surrounding tissue with perfect hemostasis. Thus, the thoracic duct could be exposed using exclusively the hook blade of the Harmonic Scalpel.
Although our experience is limited, we conclude that the Harmonic Scalpel with a hook blade can be used for thoracoscopic treatment of chylous leakage and it facilitates exposure of the thoracic duct at the supradiaphragmatic level.

{kind=link}