






Abstract
Objective: To explore the feasibility to operate on the right coronary artery and its branches utilizing the right gastroepiploic artery (RGEA) without cardiopulmonary bypass (CPB). All cases were performed since May 1996. Methods: A small mid-line incision including splitting of the lower sternum gave excellent exposure. The inferior surface of the heart was dissected to expose and stabilize the target vessel. The heart rate was controlled with a Diltiazem drip. CPB was not necessary in any case. The right coronary artery was bypassed in four patients, the posterior descending artery branch in five patients and the terminal circumflex of the left coronary artery in one patient. After grafting, patency of the anastomosis was demonstrated by Doppler echocardiogram. Results: No patient had perioperative mortality or complications. No patient had recurrent angina. Color Doppler echocardiographic imaging studies before discharge confirmed patency of the graft in eight of ten cases. In two cases, the gastroepiploic artery could not be visualized. Angiographic visualization was positive in four out of five cases. Conclusions: The gastroepiploic artery is an excellent conduit for vascularization of the inferior aspect of the heart. The operation can be done using a minimally invasive technique and without the use of cardiopulmonary bypass. This approach seems especially applicable in selective reoperative cases.
1 Introduction
The right gastroepiploic artery (RGEA) was first used as an implant for indirect myocardial revascularization approximately three decades ago [1]. Pym has popularized its usage as an arterial conduit for direct coronary artery bypass operations [6]. Ever since, a considerable experience has been accumulated, and the pathophysiology of the gastroepiploic artery has been well documented in the literature [7]. This artery, in the past decade, has been used with cardiopulmonary bypass (CPB) in combination with multiple arterial revascularizations [5,8,9,2]. If the new target is a single vessel on the inferior aspect of the heart, limited access surgery can be offered safely to avoid full sternotomy and CPB, especially in cases of reoperation [4].
We present our initial experience with the RGEA, off pump, in ten patients requiring reoperation for recurrent coronary artery disease. These operations were performed without cardiopulmonary bypass, targeting one vessel – the right coronary artery or its posterior descending and its posterolateral branch and/or the distal branch of the left circumflex coronary artery.
2 Materials and methods
A midline incision extending from the lower fourth of the sternum to midway between the xyphoid and umbilicus was utilized. The peritoneum was entered, the stomach was delivered into the wound, and the area was inspected for adequacy of size and distribution of the RGEA. The xyphoid process was excised at this point and the sternum was divided by oscillating saw in its lower fourth.
This usually entailed removal of the last two sternal wires in reoperative cases. Dissection of the diaphragmatic surface of the heart was performed at this stage, especially in redo cases, and the target vessels identified. In case 8, the circumflex branch had to be grafted, the top edge of the incision was extended in L-shaped towards the left, and the left half of the sternum was divided transversely to gain further access (Fig. 1).
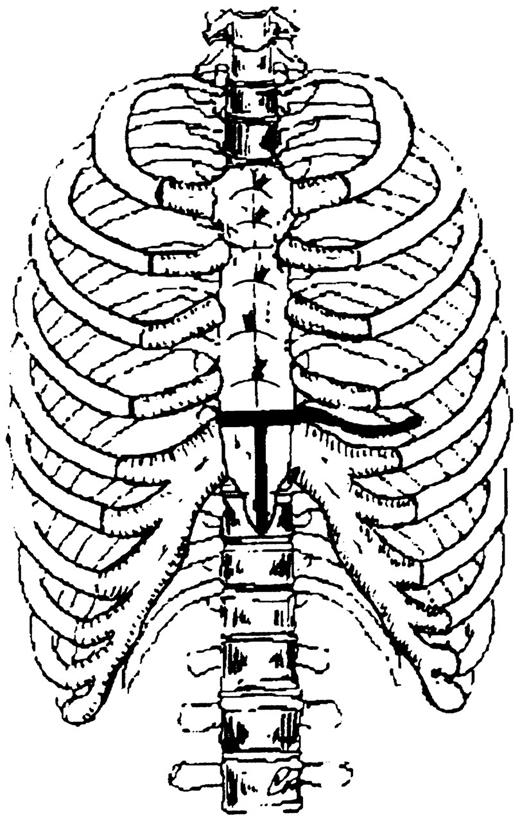
The chest and the incision of the lower third of the sternum is shown. The top of the incision can be extended to the right or to the left, carrying it into the intercostal space.
Harvesting of the RGEA was begun by separately ligating and dividing the omental and gastric branches. Starting from the most accessible part of the RGEA on the greater curvature, the dissection was carried towards the pylorus and towards the left to obtain adequate pedicle length. The pedicle was infiltrated with 1 mg/ml solution of Papaverine before any manipulation. Systemic heparinization was achieved with one-third of the conventional dose of heparin for CPB, and the distal part of the RGEA was ligated and divided. One milligram per milliliter of Papaverine solution was again injected into the graft.
The movement of the heart in reoperative cases is less because of adhesions. To further steady the target coronary artery, pledgeted sutures were placed on the acute marginal border of the right ventricle and gentle traction was applied until adequate immobilization was achieved.
The RGEA pedicle was laid out and swung into the pericardial cavity via a small opening in the central tendon of the diaphragm anterior to the pylorus and the left lobe of the liver (anterior approach).
The target coronary artery was surrounded proximally with 5.0 looping prolene sutures and an arteriotomy was made. A suitable size intraluminal Florester (internal vessel occluder, Biovascular, St. Paul, MN) was then introduced into the coronary artery to achieve a bloodless field. The RGEA to coronary artery anastomosis was then performed using a running 7.0 prolene suture on a beating heart. The pedicle was tacked to the pericardial surface near the anastomosis to prevent tension or twist. The flow pattern in the RGEA was confirmed by Doppler probe confirming a diastolic flow pattern indicating patency of the graft. The flow was also measured with a Doppler flow probe to establish quantitative assessment. Doppler echo was also requested on the first postoperative day (Fig. 2).
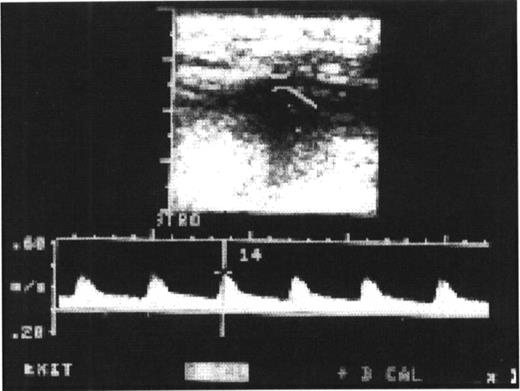
The Doppler echocardiogram postoperatively is showing a good diastolic flow pattern, verifying the patency of the RGEA.
A small drainage tube was placed in the pericardial cavity and the wound was closed in layers including the sternum utilizing the wires.
3 Results
Since July 1996, ten male patients were operated upon from the age of 46–81 years (Table 1). Nine patients out of ten underwent reoperation and one for first time CABG to the right coronary artery. The target vessels included the right coronary artery at the bifurcation, the posterior descending coronary artery, or the terminal circumflex coronary artery by the above-described technique. Preoperative catheterization on these patients had revealed graft occlusion or significant graft stenosis, new disease distal to the graft, or new disease in previously ungrafted vessels. In one case, this procedure was performed for isolated right coronary artery disease as a first time CABG. The postoperative course was uneventful in all cases and gastrointestinal functions resumed within a few hours of surgery.
List of ten male patients postoperative follow-up
All patients were studied either with color Doppler echocardiographic imaging before discharge from the hospital (Table 1) and six patients by postoperative selective angiography (Fig. 3). Postoperative stress test resulted in an exercise of 5–13 METs. In seven cases, the cardiolite imaging scan showed reversible ischemia in other areas of the left coronary artery distribution. Patient 8 had a suboptimal result and had to have a left thoracotomy to regraft the terminal circumflex vessel and it early marginal branch 6 weeks following RGEA bypass.
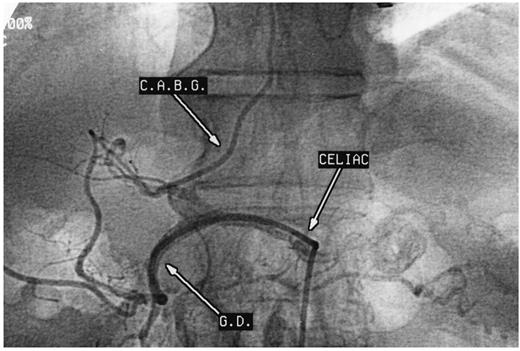
Selective postoperative catheterization of the RGEA with excellent distal filling of the right coronary artery and retrograde filling of the proximally obstructed vein graft.
4 Discussion
The pedicle RGEA has been used as an arterial conduit for Vineberg type of implant [1], as a conduit for coronary artery on the diaphragmatic surface [6, 7, 9]and also to the left anterior descending artery [8].
Minimally invasive techniques are being increasingly used to revascularlze the heart with single-vessel coronary artery disease or with redo coronary artery bypass graft operation [7]. These techniques result in minimal dissection, the use of in situ arterial grafts without utilization of the cardiopulmonary bypass and seem to avoid associated increased mortality and morbidity, particularly in reoperations.
Early and mid-term angiographic patency rates of 96 and 92% have been reported for RGEA. More recently, comparison between RGEA and RIMA for grafting the RCA or its branches has shown a preference for RGEA bypass [3].
Coronary revascularization in single-vessel disease when the target artery is on the diaphragmatic surface of the heart can be undertaken safely without cardiopulmonary bypass [4].
Although this technique was previously described for redo coronary artery bypass graft, either to the RCA or its branches, it can also be used for first time coronary artery bypass to the right coronary artery or its branches, or with extended application to the branches of the terminal circumflex coronary artery. This approach is a viable addition to various minimally invasive techniques for coronary artery bypass graft operations.

{kind=link}
{kind=link}
{kind=link}
{kind=link}