





The use of three-dimensional intracardiac echocardiography (3D ICE) has demonstrated its feasibility in guiding transcatheter tricuspid valve interventions for both percutaneous repair and direct annuloplasty.1–4 However, transfemoral (TF) navigation of the ICE catheter and simultaneous implantation of the device can be challenging for interventional cardiologists. Therefore, we propose a novel approach and intraprocedural protocol in which the echocardiographer can manipulate both 3D ICE via a transjugular (TJ) approach and transoesophageal echocardiography (TEE) during tricuspid transcatheter edge-to-edge repair (T-TEER). Figure 1A–G show all steps of the T-TEER procedure monitored with both TEE and 3D ICE. 3D ICE can improve the quality of images obtained with TEE by showing more details of the anatomic structures and overcoming the imaging limitations caused by a poor TEE window. In particular, 3D ICE was found to be useful in the grasping phase given the high anatomical imaging detail related to the tricuspid valve leaflets (Figure 1F). This innovative method allows the echocardiographer to monitor the entire imaging process by switching from TEE to ICE (Figure 1H–M). This increases the feasibility of the procedure and allows the interventional cardiologist to focus on the interventional manoeuvres. This collaborative approach not only streamlines workflow but also optimizes individual expertise and potentially improves patient outcomes. This setup is designed to place the 3D handpiece for ICE at the correct height at the side of the echocardiographer to ensure convenient access and to handle both 3D ICE and TEE with optimal manoeuvrability (Figure 1M). This setup allows for seamless integration of imaging modalities, enabling real-time assessment and guidance during T-TEER procedures. A sterile field is created to ensure the highest standards of safety for the procedure (Figure 1I–M). Figure 1N–Q show the relative positions of the TEE device and the ICE probe under fluoroscopy. Of note, the TEE probe in the mid-oesophageal position (Figure 1P) is on the left side and posterior compared with the ICE probe placed in the right atrium; this difference in position results in less favourable visualization of the tricuspid valve with TEE. In conclusion, the novel approach using both 3D ICE via the TJ approach and TEE has significant potential for guiding T-TEER. By allowing the echocardiographer to simultaneously manipulate both modalities, the procedure improves image quality and thus contributes to better patient outcomes in tricuspid valve interventions.
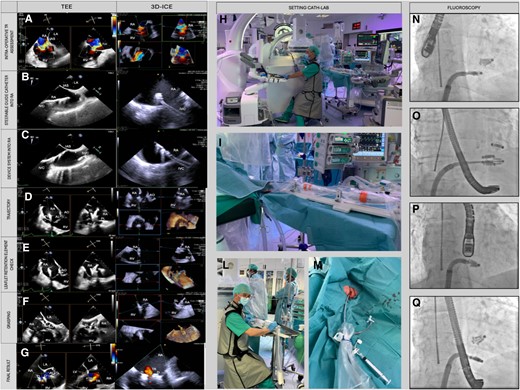
Combining echocardiographer-guided 3D ICE and TEE in T-TEER. The left panel compares the same step of the T-TEER monitored with both TEE and 3D ICE. (A) Colour flow imaging with both modalities. (B) The insertion of the guiding catheter into the right atrium. (C) The insertion of the device into the right atrium. (D) The steering of the implant catheter to obtain a straight trajectory on the tricuspid valve. (E) The retention elements of the device for independent grasping. (F) Leaflet insertion into the device is assessed with TEE and ICE imaging. (G) The assessment of residual regurgitation. Central panel shows the cath lab setup with the echocardiographer able to switch between 3D ICE and TEE (H–L). (I and M) The use of TJ access for positioning the 3D ICE probe with a standard valved straight introducer sheath. Right panel show TEE and ICE probe position under fluoroscopy. The position of devices from right oblique projection (N and O) and antero-posterior projection (P and Q), with the TEE probe in mid-oesophageal position in N and P and in transgastric position in O and Q. IAS, interatrial septum; IVC, inferior vena cava; LA, left atrium; RA, right atrium; RV, right ventricle; SVC, superior vena cava.
Consent
Written informed consent has been obtained from the patient for the procedure.
Funding
This research received no external funding.
Data availability
No new data were generated or analysed in support of this research.
Lead author biography

Massimiliano Mariani serves as a cardiologist at Heart Hospital Fondazione G. Monasterio in Massa, Italy. His practice is focused on diagnosis and treatment of heart valve’s diseases as he started as echocardiographer, the transcatheter structural heart disease programme in his hospital. As a fellow of EACVI, he is committed in standardization of methods and education in transoesophageal and intracardiac echocardiography and their application to transcatheter procedures. His research activity is oriented to the development of imaging modalities in intraprocedural echocardiography.
References
Author notes
Massimiliano Mariani and Michela Bonanni contributed equally to this work.
Conflict of interest: None declared.

{kind=link}