




Abstract
Sodium-glucose cotransporter 2 inhibitors (SGLT2-Is) improve heart failure (HF) outcomes but their effects on acute myocardial infarction (AMI) remains poorly characterized. This study aimed to evaluate the one-year cardiovascular outcomes of SGLT2-Is among patients with AMI.
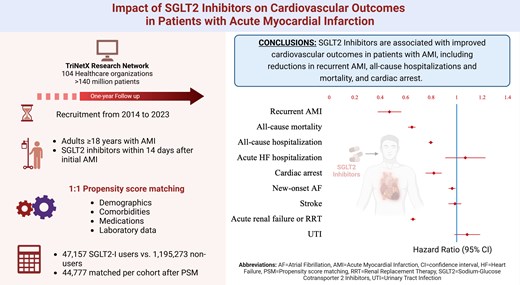
We conducted an observational, retrospective cohort study using TriNetX data, including patients aged ≥18 with AMI identified via ICD-10 codes regardless of left ventricular ejection fraction (LVEF), categorized by SGLT2-Is use. Propensity score matching (PSM) was performed to balance baseline demographics, comorbidities, and medication use. Adjusted odds ratios (aORs) were estimated for the primary outcome (recurrent AMI) and the secondary outcomes (acute HF hospitalizations, stroke, all-cause hospitalizations, all-cause mortality, new-onset atrial fibrillation, and cardiac arrest). After PSM, 89,554 patients were analyzed (44,777 SGLT2-Is users; 44,777 non-users). The mean age was approximately 68 years in both cohorts with a similarly high burden of cardiovascular comorbidities. Mean follow-up duration was 290.854 days for SGLT2-Is users and 284.465 days for non-users. SGLT2-Is use was linked to lower rates of recurrent AMI (aOR: 0.459; 95% CI: 0.367–0.551), all-cause hospitalizations (aOR: 0.782; 95% CI: 0.762–0.803), all-cause mortality (aOR: 0.640; 95% CI: 0.612-0.670), and cardiac arrest (aOR: 0.834; 95% CI: 0.773–0.900). No differences were observed in acute HF hospitalizations, new-onset atrial fibrillation, or stroke.
SGLT2-Is are associated with improved cardiovascular outcomes in patients with AMI, including reductions in recurrent AMI, all-cause hospitalizations and mortality, and cardiac arrest. These findings emphasize the need for prospective clinical trials involving patients with AMI and other cardiovascular comorbidities, regardless of left ventricular ejection fraction, to confirm these results.
 Accepted manuscripts
Accepted manuscripts
{kind=link}