





Abstract
The present article summarizes three cases of retrieving entrapped guidewire using rotablation technique.
All three cases pertained to guidewire being fractured and entrapped during percutaneous coronary interventions (PCIs) for right coronary artery (RCA) chronic total occlusion in a local hospital. In Case 1, two fractured filaments connecting to the entrapped guidewire could be clearly seen. One filament was in the right brachial artery and the other one was in the ascending aorta. In Case 2, the operator applied buddy wire technique during PCI but forgot to withdraw the second wire before stenting. As a result, the second SION wire was entrapped by the stent and was untangled and fractured when being retrieved. In Case 3, a SION guidewire was entrapped during PCI for RCA. The initial attempt to retrieve the guidewire ended in failure. Although the entrapped guidewire was still intact, it was difficult to advance the floppy rotawire into the RCA as it was still totally occluded. In those scenarios, complete retrieval of the entrapped guidewire using catheter-based technique was hardly possible. Rotablation was used to cut the entrapped guidewire, retrieve the broken end, and leave the remnants in coronary artery jailed by the stent. Clinical and angiographic follow-up observation demonstrated that the patients were free of target vessel failure.
Entrapment of guidewire is a rare complication of PCI. The management of entrapped guidewire is usually challenging. Rotablation technique is a useful and efficient strategy when conventional methods failed to retrieve the entrapped guidewire.
Conventional catheter-based techniques to retrieve broken coronary guidewire can be unsuccessful as the wire tip is usually tightly entrapped.
Rotablation technique can be considered for retrieval of entrapped untangled guidewires after failure of conventional catheter-based methods.
Introduction
Entrapment of guidewire is a rare complication of percutaneous coronary interventions (PCI). The reported incidence is ∼0.1–0.2%, usually occurred during PCI of chronic total occlusion (CTO).1 The management of patients with entrapped wire is challenging. Catheter-based retrieval is generally preferred over surgical extraction. Conventional catheter-based methods include stent jailing, snare loop retrieval, wire tangling technique, microcatheter supporting, guiding catheter deep wedging, and balloon inflation.2,3 These techniques were generally time-consuming and had unpredictable success rates. Besides, prolonged manipulation of entrapped devices may increase the risk of thrombus, air embolization, coronary ostial injury, and stent deformation.1,4 Rotablation, a technique widely used to debulk heavily calcified plaque, was found useful for entrapped guidewire retrieval recently. Here, we report our experience of successful retrieval of entrapped guidewire using rotablation technique by presenting the following cases in accordance with the CARE reporting checklist.
Timeline
| Events | |
|---|---|
| Case 1 | |
| 20 April 2021 | Coronary angiography revealed that serious three-vessel coronary artery lesions and chronic total occlusion (CTO) in right coronary artery (RCA) |
| 22 April 2021 | Percutaneous coronary interventions (PCI) in left anterior descending (LAD) |
| 29 April 2021 | GAIA-2 guidewire was fractured during PCI for RCA CTO in a local hospital |
| Admission 1 30 April 2021 | Retrieving entrapped guidewire |
| 2 May 2021 | Discharged in stable condition |
| Admission 2 26 July 2021 | Follow-up coronary angiography showed the RCA stent was unobstructed |
| Outpatient 4 January 2022 | Stable (no coronary event) |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Case 2 | |
| 13 May 2021 | Coronary angiography revealed that three-vessel coronary artery disease and had PCI to LAD |
| 16 June 2021 | Elective PCI and buddy wire technique was applied for RCA CTO, the second Sion wire was entrapped by the stent and the proximal stent in RCA was deformed |
| Admission 18 June 2021 | The deformed stent was dilated and another stent was implanted, the blood flowed in RCA was restored; retrieving untangled entrapped wire |
| 20 June 2021 | Discharged in stable condition |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Case 3 | |
| 16 August 2019 | Diagnosed coronary artery disease in local hospital and had PCI to LAD |
| 19 September 2019 | A SION guidewire was entrapped during elective PCI for RCA |
| Admission 19 September 2019 | Cutting and retrieving the entrapped guidewire using rotablation technique |
| 22 September 2019 | Discharged in stable condition |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Events | |
|---|---|
| Case 1 | |
| 20 April 2021 | Coronary angiography revealed that serious three-vessel coronary artery lesions and chronic total occlusion (CTO) in right coronary artery (RCA) |
| 22 April 2021 | Percutaneous coronary interventions (PCI) in left anterior descending (LAD) |
| 29 April 2021 | GAIA-2 guidewire was fractured during PCI for RCA CTO in a local hospital |
| Admission 1 30 April 2021 | Retrieving entrapped guidewire |
| 2 May 2021 | Discharged in stable condition |
| Admission 2 26 July 2021 | Follow-up coronary angiography showed the RCA stent was unobstructed |
| Outpatient 4 January 2022 | Stable (no coronary event) |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Case 2 | |
| 13 May 2021 | Coronary angiography revealed that three-vessel coronary artery disease and had PCI to LAD |
| 16 June 2021 | Elective PCI and buddy wire technique was applied for RCA CTO, the second Sion wire was entrapped by the stent and the proximal stent in RCA was deformed |
| Admission 18 June 2021 | The deformed stent was dilated and another stent was implanted, the blood flowed in RCA was restored; retrieving untangled entrapped wire |
| 20 June 2021 | Discharged in stable condition |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Case 3 | |
| 16 August 2019 | Diagnosed coronary artery disease in local hospital and had PCI to LAD |
| 19 September 2019 | A SION guidewire was entrapped during elective PCI for RCA |
| Admission 19 September 2019 | Cutting and retrieving the entrapped guidewire using rotablation technique |
| 22 September 2019 | Discharged in stable condition |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Events | |
|---|---|
| Case 1 | |
| 20 April 2021 | Coronary angiography revealed that serious three-vessel coronary artery lesions and chronic total occlusion (CTO) in right coronary artery (RCA) |
| 22 April 2021 | Percutaneous coronary interventions (PCI) in left anterior descending (LAD) |
| 29 April 2021 | GAIA-2 guidewire was fractured during PCI for RCA CTO in a local hospital |
| Admission 1 30 April 2021 | Retrieving entrapped guidewire |
| 2 May 2021 | Discharged in stable condition |
| Admission 2 26 July 2021 | Follow-up coronary angiography showed the RCA stent was unobstructed |
| Outpatient 4 January 2022 | Stable (no coronary event) |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Case 2 | |
| 13 May 2021 | Coronary angiography revealed that three-vessel coronary artery disease and had PCI to LAD |
| 16 June 2021 | Elective PCI and buddy wire technique was applied for RCA CTO, the second Sion wire was entrapped by the stent and the proximal stent in RCA was deformed |
| Admission 18 June 2021 | The deformed stent was dilated and another stent was implanted, the blood flowed in RCA was restored; retrieving untangled entrapped wire |
| 20 June 2021 | Discharged in stable condition |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Case 3 | |
| 16 August 2019 | Diagnosed coronary artery disease in local hospital and had PCI to LAD |
| 19 September 2019 | A SION guidewire was entrapped during elective PCI for RCA |
| Admission 19 September 2019 | Cutting and retrieving the entrapped guidewire using rotablation technique |
| 22 September 2019 | Discharged in stable condition |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Events | |
|---|---|
| Case 1 | |
| 20 April 2021 | Coronary angiography revealed that serious three-vessel coronary artery lesions and chronic total occlusion (CTO) in right coronary artery (RCA) |
| 22 April 2021 | Percutaneous coronary interventions (PCI) in left anterior descending (LAD) |
| 29 April 2021 | GAIA-2 guidewire was fractured during PCI for RCA CTO in a local hospital |
| Admission 1 30 April 2021 | Retrieving entrapped guidewire |
| 2 May 2021 | Discharged in stable condition |
| Admission 2 26 July 2021 | Follow-up coronary angiography showed the RCA stent was unobstructed |
| Outpatient 4 January 2022 | Stable (no coronary event) |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Case 2 | |
| 13 May 2021 | Coronary angiography revealed that three-vessel coronary artery disease and had PCI to LAD |
| 16 June 2021 | Elective PCI and buddy wire technique was applied for RCA CTO, the second Sion wire was entrapped by the stent and the proximal stent in RCA was deformed |
| Admission 18 June 2021 | The deformed stent was dilated and another stent was implanted, the blood flowed in RCA was restored; retrieving untangled entrapped wire |
| 20 June 2021 | Discharged in stable condition |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
| Case 3 | |
| 16 August 2019 | Diagnosed coronary artery disease in local hospital and had PCI to LAD |
| 19 September 2019 | A SION guidewire was entrapped during elective PCI for RCA |
| Admission 19 September 2019 | Cutting and retrieving the entrapped guidewire using rotablation technique |
| 22 September 2019 | Discharged in stable condition |
| Follow-up via telephone 14 February 2022 | Stable (no coronary event) |
Case presentation
Case 1
A 51-year-old Han man, with no past medical history, was referred to our hospital because a GAIA-2 guidewire (Asahi Intecc, Nagoya, Japan) was fractured during PCI for right coronary artery (RCA) CTO in a local hospital. No remarkable abnormalities in the physical examinations were found. The high-sensitivity cardiac troponin T was slightly elevated (83 ng/L, reference value <14 ng/L). Emergency coronary angiography (∼24 h after the guidewire fractured) demonstrated that the entrapped guidewire was untangled. Two fractured filaments connecting to the entrapped guidewire could be clearly seen (Figure 1A,B). One filament was in the right brachial artery and the other one in the ascending aorta, with a loop formed by the filament (Figure 1C,D). At that time, complete retrieval of the entrapped guidewire using catheter-based technique was hardly possible. We decided to cut and retrieve the untangled filaments using rotablation and left the remnants in the coronary artery, jailed by stent. The retrieval of the fractured guidewire was performed in the following steps: (i) Use a snare to catch the untangled guidewire through the right radial artery (Figure 2A). Use another snare to catch the untangled guidewire loop in the ascending aorta through the left radial approach (Figure 2B). (ii) Set up the rotablation system (Rotablator Rotational Atherectomy System, Boston Scientific Corporation) through femoral approach. Cut off the untangled guidewire at the ostium of RCA using rotablation (Figure 2C,D). Then retrieve the fractured guidewire filaments, which were held by the snares. (iii) Post-dilation to achieve ideal stent expansion and to make sure that the entrapped guidewire remnants were firmly jailed under the stent (Figure 2E). The untangled wire and the retrieving action were more vivid in Supplementary material online, Videos S1 to S6. The patient was discharged in stable condition with dual antiplatelet therapy including aspirin and clopidogrel. Three months after the procedure, a follow-up coronary angiography showed that the RCA stent was unobstructed.
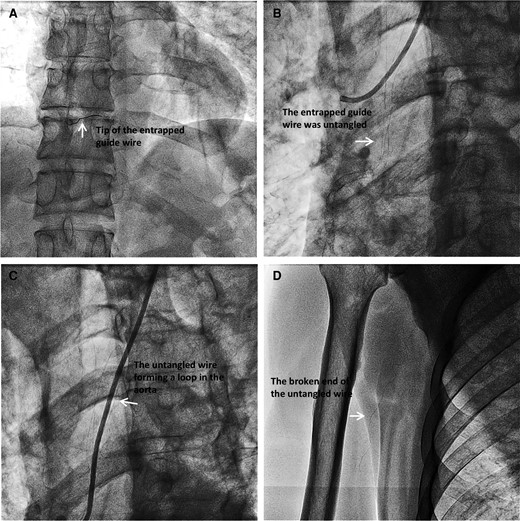
Entrapped guidewire. (A). Guidewire entrapped in RCA; (B). The entrapped guidewire was broken and untangled; (C). The untangled wire was forming a loop in ascending aorta; (D). The broken end of the untangled wire in the right brachial artery.
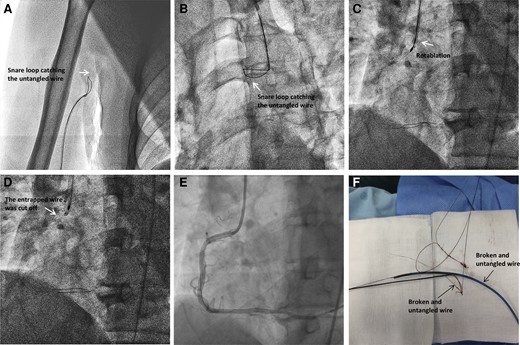
Retrieval of the fractured guidewire. (A). Snare loop catching the untangled guidewire in the right radial artery; (B). Another snare catching the untangled guidewire in the ascending aorta through the left radial approach; (C). Rotablation to cut the guidewire at the ostium of RCA; (D). The entrapped wire was cut off. (E). The entrapped guidewire remnants were jailed under the stent; (F). The retrieved broken guidewire.
Case 2
A 75-year-old Han man, with a history of hypertension and prior ischaemic stroke, had received PCI for an RCA CTO in a local hospital before being referred to our hospital. During the RCA PCI, buddy wire technique was applied. But the operator forgot to withdraw the second wire before stenting. As a result, the second SION wire was entrapped by the stent. The entrapped wire untangled and fractured when being retrieved. Nevertheless, the proximal stent was deformed. After being transferred to our hospital, no remarkable abnormalities in the physical examinations were found except for muscle strength weakness (Grade II) of left limb. The high-sensitivity cardiac troponin T was slightly elevated (152 ng/L, reference value < 14 ng/L). Emergency coronary angiography (∼57 h after the guidewire fractured) revealed that the proximal right coronary stent was longitudinally compressed and had visible thrombosis (Figure 3A,B, see Supplementary material online, Videos S7 and S8). We carefully advanced a guidewire through the deformed stent. The deformed stent was dilated, and another stent was implanted to make sure that the lesion in proximal RCA was fully covered. After the blood flow in RCA was restored, we tried to retrieve the fractured guidewire. The broken end of untangled guidewire was in the right carotid artery (Figure 3C, see Supplementary material online, Video S9). The initial attempts to catch the broken end through right radial approach ended in failure (Figure 3D, see Supplementary material online, Video S10). With the help of MP A1(I) catheter (Figure 3E, a type of single bend catheter with a length of 125 cm, Cordis Corporation), the broken end was caught by a snare through femoral approach. Then, the rotablation system (Rotablator Rotational Atherectomy System, Boston Scientific Corporation) was set up. The untangled guidewire was cut off at the ostium of RCA using rotablation and retrieved (Figure 3F and Figure 4A, see Supplementary material online, Videos S11 and S12). The patient was discharged in stable condition with dual antiplatelet therapy including aspirin and ticagrelor. During a 7-month follow-up, the patient remained stable without coronary event.
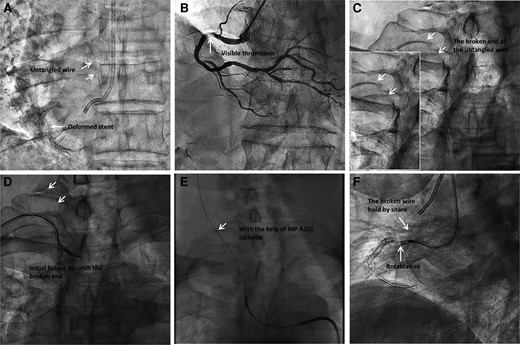
The entrapped guidewire. (A–B). The proximal right coronary stent was longitudinally compressed and had visible thrombosis. (C). The broken end of untangled guide wire in the right carotid artery. (D). The initial attempts to catch the broken end through right radial approach ended in failure. (E). With the help of MP A1(I) catheter, the broken end was caught by a snare through femoral approach. (F). The untangled guidewire was cut off at the ostium of RCA using rotablation.
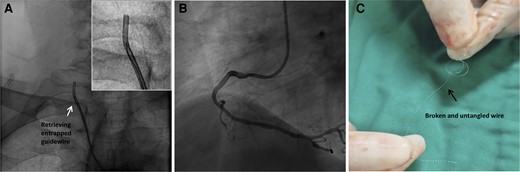
Retrieval of the fractured guidewire. (A). The entrapped guidewire was retrieved. (B). The blood flow in RCA was restored. (C). Retrieved broken guidewire.
Case 3
A 52-year-old Han man, with history of hypertension and diabetes mellitus, was referred to our hospital because a SION guidewire was entrapped during PCI for RCA in a local hospital. No remarkable abnormalities in the physical examinations were found. The high-sensitivity cardiac troponin T was slightly elevated (40 ng/L, reference value < 14 ng/L). The initial attempts to retrieve the guidewire with support of microcatheters and balloons ended in failure. But the entrapped guidewire was still intact. At that time, we decided to cut and retrieve the entrapped guidewire using rotablation technique. But in this case, the RCA was still totally occluded. It was difficult to advance the floppy rotawire into the RCA. As a result, we chose a novel retrograde rotablation approach by using Rotablator Rotational Atherectomy System (Boston Scientific Corporation). The procedure was performed as follows: (i) Use a second guiding catheter to approach the initial guiding catheter. (ii) Advance the floppy rotawire into the initial guiding catheter. 3. Initiate rotablation at the tip of the initial guiding catheter to cut the entrapped guidewire and retrieve the fractured wire. The detailed information of the case was published last year (doi: 10.5603/CJ.2020.0158.).5 The patient was discharged in stable condition with dual antiplatelet therapy including aspirin and clopidogrel. During a 2-year follow-up, the patient remained stable but refused any further attempts to revascularize the RCA.
Discussion
The management of entrapped guide wire usually includes catheter-based retrieval, surgical removal, or conservative management. Abdulrahman M et al.1 summarized the pros and cons of these three strategies in 2013. The catheter-based approach is generally preferred over surgical intervention unless grafting of the affected coronary artery is necessary.6,7 A variety of catheter-based techniques including double or triple wire technique, deep-guide catheter wedge, balloon inflation technique, and snare loop catching have been used for guidewire retrieval. The more recent case reports of managing entrapped guidewire are summarized in Supplementary material online, Table S1. Some novel techniques, such as laser atherectomy, rotational atherectomy, have been applied in entrapped guidewire retrieval.
If the wire is still intact, usually the first choice should be wholly pulling out the entrapped wire. Usually, guide catheter deep wedging and microcatheter supporting are needed to increase support and avoid cutting effect of the entrapped wire.8,9 However, in some cases, the entrapped guidewire may be fractured. There is very limited data regarding clinical outcomes of retained guidewire fragments. The adverse sequelae usually includes accelerated restenosis, thrombosis, and perforation.10 Retrieval of the remnants is extremely difficult. The first challenge is to tightly hold the broken end. If the broken end is still in the guide catheter, usually balloon jailing in the guide catheter is the simplest method. If the broken end is out of the guide catheter, wire tangling or snare loop catching should be considered. But even if these efforts of holding the broken end succeed, the retrieval of the broken fragment is still very difficult. The fact that the guidewire is broken usually indicates the tip is very tightly entrapped. The conventional wire-catching techniques usually do not have enough strength to retrieve it. If the retained fragment is entirely inside the vessel, stenting and jailing the fragment might be an option. In that scenario, case reports demonstrated that the remnants were generally benign and conservative strategy involving intensive antithrombotic treatment was a reasonable option.11–13
Considering the relative benign outcome of jailing guidewire fragment in the vessel, deliberate wire-cutting with a rotational atherectomy device is considered a reasonable last resort option for retrieving the entrapped guidewire. Dr. Jae Young Cho and Soon Jun Hong14 reported the first case of successful retrieval of entrapped guidewire by deliberately cutting the guidewire using a rotational atherectomy device. In Dr. Jae Young Cho’s case, the guidewire tip was strongly entrapped in a severely calcified plaque. All conventional catheter-based attempts failed to retrieve the entrapped wire. The operator chose to initiate rotablation in coronary artery, and the entrapped wire was successfully cut off and partially retrieved. The fragments left in coronary artery were jailed by stent.
If the entrapped guidewire is already broken and the broken end is outside the coronary artery, the conventional strategy is to catch the broken end using wire tangling, snare loop or other techniques. But as discussed before, these techniques usually do not have enough strength to retrieve the entrapped wire. In our cases, we used rotablation to cut the entrapped guide wire, retrieve the broken end and left the remnants in coronary artery jailed by stent.
Usually, the rotablation is performed in the coronary artery. In case three, the guidewire was entrapped in a still occluded artery. In that case, to advance a floppy rotawire into the occluded coronary artery was very difficult. As a result, we used a novel retrograde rotablation technique. The rotablation was performed in the guiding catheter rather than coronary artery. The retrograde rotablation technique was highly efficient and did not have complications related to conventional rotablation.
The antithrombotic regimen for PCI patients with retained fractured guidewire fragments is particularly challenging due to a lack of enough data regarding its clinical outcomes. Up to date, there are no guidelines in regard to the optimal management or choice of antiplatelet/anticoagulation regimen of patients with PCI and retained fractured guidewire fragments. In our experience, the prolonged dual antiplatelet strategy (usually aspirin plus ticagrelor) seems safe and effective for these patients.
In view of the difficulty of broken fragment retrieval, the operators should be aware of this complication and be familiar with the measures to avoid it in clinical practice. Bifurcation lesions, tortuous, and calcified lesions, and use of firm-tipped guidewires are important risk factors for guidewire entrapments and fractures. There are some tips to prevent guidewire entrapment: (i) Try to avoid advancing the wire too far in small branches; (ii) When the buddy wire technique is used to enforce support, remove the second guidewire before the stent is inflated; (iii) Remember to rewire the side branch protecting wire before high pressure post-dilation; (iv) Avoid continuous rotating the guidewire in the same direction if the guidewire is entrapped in severely calcified lesions; (v) Operator should be more careful when treating complex calcified lesions with hydrophilic-coated guidewires.
Conclusion
Deliberate wire-cutting with a rotational atherectomy device may be considered as a reasonable last resort option for retrieving the entrapped guidewire after the failure of conventional catheter-based attempts. More long-term observations are needed to illustrate the safety and efficiency of rotablation technique in the retrieval of entrapped guidewire.
Lead author biography
 Mian Wang is an associate professor of Department of Cardiology, West China Hospital of Sichuan University. She is engaged in clinical work in the Department of Cardiology for 20 years and has extensive clinical experience; she is good at diagnosis and treatment of various difficult and severe cardiovascular diseases and interventional treatment of complicated coronary artery disease. She is proficient in CTO intervention, rotational atherectomy for calcification lesions, intravascular ultrasound, and other interventional techniques.
Mian Wang is an associate professor of Department of Cardiology, West China Hospital of Sichuan University. She is engaged in clinical work in the Department of Cardiology for 20 years and has extensive clinical experience; she is good at diagnosis and treatment of various difficult and severe cardiovascular diseases and interventional treatment of complicated coronary artery disease. She is proficient in CTO intervention, rotational atherectomy for calcification lesions, intravascular ultrasound, and other interventional techniques.
Supplementary material
Supplementary material is available at European Heart Journal – Case Reports online.
Acknowledgements
The authors appreciate Wenyi Zhang for her editing advice.
Slide sets: A fully edited slide set detailing this case and suitable for local presentation is available online as Supplementary data.
Consent: The authors confirm that written consent for submission and publication of this case report including images and associated text has been obtained from the patient in line with COPE guidance.
Conflict of interest: None declared. Written informed consents were obtained from the patients for publication of these case reports and any accompanying images.
Funding: This study was funded by grant from National Natural Science Foundation of China (grant number 82100282). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments