





Abstract
Diagnostic dilemmas in an unwell neonate can require the use of enhanced imaging modalities, especially in post-operative cardiac disease.
A neonate presented a diagnostic challenge following the repair of complex transposition of the great arteries, when an echogenic mass was noted in the region of the left atrial appendage on two-dimensional echocardiography, in the context of a monitoring line (left atrial line) inserted directly through this area. Although the pressure monitoring on this line suggested elevated left atrial pressure, the neonate was clinically and haemodynamically stable. Contrast echocardiography was used to investigate this further and found the mass to be extracardiac.
Contrast echocardiography is a simple and readily available tool for further echocardiographic delineation of structures, although needs to be performed carefully and the results interpreted logically.
Contrast echocardiography can assist with outlining thrombus and may assist in differentiating between intracardiac and extracardiac thrombus.
Contrast echocardiography is a useful tool to delineate flow between intravascular lines, vessels and cardiac chambers and can thus contribute to confirming the location of an access line.
Introduction
Contrast echocardiogram is an easily accessible, safe, and cost-effective imaging modality, which can assist with some diagnostic dilemmas. This report illustrates the use of contrast echocardiography for confirmation of monitoring line position and differentiating between intracardiac and extracardiac thrombus.
Timeline

Case presentation
A 1-week old infant with transposition of the great arteries, ventricular septal defect, and hypoplastic aortic arch underwent a full correction with arterial switch operation. Due to the complexity of the operation, the chest was electively left open for the first post-operative night. A monitoring line was implanted directly via the left atrial appendage for monitoring of the left atrial pressure. Post-operatively, these pressure readings had been elevated to 30 mmHg, although there were concerns this may have been spurious. Other parameters were reassuring, with normal lactate levels and no evidence of ischaemic changes on electrocardiogram. Echocardiogram was performed for further assessment.
Transthoracic echocardiogram demonstrated normal atrioventricular and neo-aortic and pulmonary valve function, with mild impairment of the systolic ventricular function in keeping with the post-operative period. A heterogeneous, echogenic mass was noted in the region of the left atrial appendage, although localization of the mass as clearly intracardiac or extracardiac was difficult. At least one left-sided pulmonary vein could be identified draining in superiorly to the mass with laminar flow. Further delineation of location of this mass and the site of the monitoring line was sought, given this line as a potential nidus of thrombus formation in the left atrium.
After confirming free aspiration of the monitoring line, gentle contrast echocardiography was performed utilizing agitated albumin to delineate the location of the left atrial line in relation to the identified mass. This demonstrated contrast entering the left atrium superior to the echogenic mass and further delineated the smooth outline of this before draining to the left ventricle (Figure 1 and Video 1). No changes in the appearance of the mass were noted during the injection. This imaging provided information regarding both the left atrial line location in the atrium as intended and suggested the mass was likely to be extra-atrial.
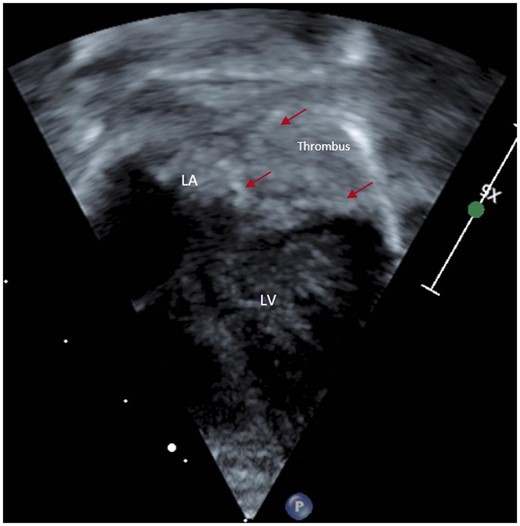
Contrast entering left atrium superior to echogenic mass, smooth lined left atrial wall delineated (red arrows) before it drains to left ventricle. LA, left atrium; LV, left ventricle.
Agitated albumin contrast injection via the left atrial line.
The infant returned to the operating theatres for open chest exploration. The thrombus was confirmed to be extracardiac, adjacent to the left atrial appendage and was removed. Subsequently, the child had an uneventful recovery and was later discharged.
Discussion
Agitated contrast injection can be a useful mechanism to define the location of vascular and cardiac lines, with contrast appearing in the vessel/chamber with which the line communicates. In addition, this contrast can be used to outline cardiac structures, which may help with delineation and location of masses in or adjacent to these structures.1 Care must be taken with these injections, with an assessment of the risk/benefit ratio of undertaking such an investigation, particularly when considering the systemic circulation. In this instance a very gentle injection was performed, which we felt would not alter flow in the atrial chamber significantly more than the pulmonary venous flow, whilst providing potentially valuable information. We would advise caution in the context of a left atrial line such as this not aspirating freely, as the possibility of embolizing thrombus may be higher.
The reported incidence of thrombosis post cardiac surgery in children is about 11%.2 Undergoing cardiac surgery puts children at high risk of developing thrombus in comparison to the other hospitalized children.2 These children are at increased risk of life-threatening complications including embolic arterial stroke, sinovenous stroke, pulmonary embolism, superior vena cava syndrome, and cardiopulmonary arrest or death.2 Early detection and management is the key to prevent its long-term consequences. Transthoracic echocardiogram has a good sensitivity (93%) to identify cardiac masses.1 Generally, thrombus has a smooth profile and moves in synchrony with the adjacent heart wall during cardiac cycle.1 It may be difficult to comment on thrombus extent and location, especially in relation to an intracardiac line. In such cases, use of contrast echocardiography improves the discrimination between blood and intracavitary masses and provides real-time assessment of the cardiac blood flow.3 The provision of accurate information to the surgical team allows optimal operative planning, with sensible back-up plans in place should the findings vary at the time of surgery. This report emphasizes the role of contrast echocardiogram in yielding valuable information in paediatric post-operative care settings.
Conclusion
Contrast echocardiography is a simple and readily available tool for further echocardiographic delineation of intravascular line position and cardiac structures, although needs to be performed carefully and the results interpreted logically. This report emphasizes the role of contrast echocardiogram in yielding valuable information in paediatric post-operative care settings.
Lead author biography

Bharti Sharma is a Paediatric Cardiologist from India. She completed her Paediatrics training in 2013 from Mumbai, post which she did a 2 year Fellowship in Paediatric Cardiology in Hyderabad, India. Recently, she worked as a fellow in Pediatric Cardiology at the Queensland Childrens Hospital, Brisbane, Australia for 1 year. Her interests predominantly lie in clinical cardiology, imaging, and haemodynamics.
Supplementary material
Supplementary material is available at European Heart Journal - Case Reports online.
Acknowledgements
Special thanks to Dr Prem Venugopal for the expert advice on the manuscript. Special mention of Sinh Le (our radiographer) for technical assistance.
Slide sets: A fully edited slide set detailing this case and suitable for local presentation is available online as Supplementary data.
Consent: The authors confirm that written consent for submission and publication of this case report, including images and associated text, has been obtained in line with COPE guidance.
Conflict of interest: None declared.
Funding: None declared.

{kind=link}
{kind=link}
{kind=link}
Comments