





Case description
A 67-year-old male has been repeatedly hospitalized multiple times, with a history of recurrent chest tightness and generalized oedema accompanied by gastrointestinal bleeding for 8 years. Prominent jugular vein distension was noted. The patient had old pulmonary tuberculosis. Chest X-rays in both posteroanterior and left lateral views showed an oval-shaped calcification along the atrioventricular groove, pleural effusion, and pulmonary oedema (Figure 1A and B). Transthoracic echocardiography demonstrated thickened and hyperechoic pericardium along the atrioventricular groove with localized angulation, the interventricular septal bounce associated with respiration, thin ventricular wall without granular echoes, preserved ventricular wall motion, mitral inflow respiratory variation <25%, dilated inferior vena cava with inspiratory collapse <50%, and moderate biatrial enlargement. Tissue Doppler imaging showed that mitral annular early diastolic peak velocity (e′) is 14.2 cm/s. CT of the chest revealed an oval-shaped and localized eggshell-like calcification along the atrioventricular groove (Figure 1C), dilated inferior vena cava and portal vein, with multiple tortuous and engorged vessels in the hepatogastric space and gastric fundus. Pericardiectomy was performed. Biopsy of the pericardium showed: after decalcification, the hardened tissue of the specimen exhibited dense fibrous tissue with partial adipose tissue under microscopy, along with areas of collagenization with extensive calcification. Post-operatively, the symptoms of heart failure including chest tightness and generalized oedema resolved, and no further gastrointestinal bleeding occurred.
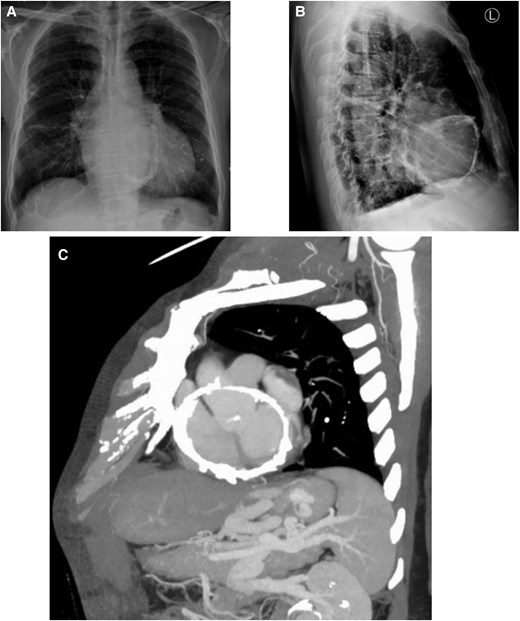
(A, B) Posteroanterior and lateral chest radiographs demonstrate an oval-shaped annular calcification adjacent to the atrioventricular groove, accompanied by pleural effusion and pulmonary oedema. (C) Contrast-enhanced chest CT reveals an oval-shaped calcification along the atrioventricular groove with localized eggshell-like hyperdensity. Note the dilated inferior vena cava and portal vein, along with multiple tortuous and engorged collateral vessels in the hepatogastric space and gastric fundus.
Constrictive pericarditis is a rare cause of gastric variceal bleeding.1,2 In this case, the chronic restriction of cardiac diastolic function led to persistently elevated venous pressure. The long-standing inferior vena cava hypertension ultimately resulted in portal hypertension, causing gastrointestinal bleeding. The patient had previously undergone esophagogastroduodenoscopy with gastric fundal variceal ligation. Investigations revealed that the constrictive pericarditis was caused by tuberculosis. However, tuberculous constrictive pericarditis with an oval-shaped annular calcification along the atrioventricular groove is exceptionally rare, and indicates the high risk of late-stage complications and mortality.
Consent: Consent for publication was obtained in line with the COPE best practice guidelines.
Funding: None declared.
Data availability
The data from the cases in this study can be obtained from the corresponding author upon reasonable request.
References
Author notes
Conflict of interest. None declared.

{kind=link}
Comments