





Abstract
The Leiden Convention coronary coding system structures the large variety of coronary anatomical patterns; isolated and in congenital heart disease. It is widely used by surgeons but not by cardiologists as the system uses a surgeons’ cranial view. Since thoracic surgeons and cardiologists work closely together, a coronary coding system practical for both disciplines is mandatory. To this purpose, the ‘surgical’ coronary coding system was adapted to an ‘imaging’ system, extending its applicability to different cardiac imaging techniques.
The physician takes place in the non-facing sinus of the aortic valve, oriented with the back towards the pulmonary valve, looking outward from the sinus. From this position, the right-hand sinus is sinus 1, and the left-hand sinus is sinus 2. Next, a clockwise rotation is adopted starting at sinus 1 and the encountered coronary branches described. Annotation of the normal anatomical pattern is 1R-2LCx, corresponding to the ‘surgical’ coding system. The ‘imaging’ coding system was made applicable for Computed Tomography (CT), Magnetic Resonance Imaging (MRI), echocardiography, and coronary angiography, thus facilitating interdisciplinary use. To assess applicability in daily clinical practice, images from different imaging modalities were annotated by cardiologists and cardiology residents and results scored. The average score upon evaluation was 87.5%, with the highest scores for CT and MRI images (average 90%).
The imaging Leiden Convention is a coronary coding system that unifies the annotation of coronary anatomy for thoracic surgeons, cardiologists, and radiologists. Validation of the coding system shows it can be easily and reliably applied in clinical practice.

Introduction
The coronary circulation can have an array of patterns. Where in most cases two orifices give rise to three main coronary arterial branches, more complex patterns, including single sinus coronary arteries, are also encountered. Especially when the great arteries are abnormally aligned, as is the case in different forms of congenital heart disease, e.g. transposition of the great arteries (TGA) and tetralogy of Fallot, it may be challenging to systematically describe the coronary anatomy. Over the past years, several classification systems have been developed to describe the origin and patterning of the coronary arteries.1–4 Unfortunately, these methodologies are not applicable irrespective of the position of the great arteries. In 1983, a coding system (dubbed ‘the Leiden Convention’) was designed which is independent of the position of the great arteries, thus rendering it also applicable to hearts with a different relationship of the great arteries relative to each other, such as TGA.5,6 In 2018, Gittenberger-de Groot et al.7 proposed the ‘modified Leiden Convention’, which also includes the course of the coronary branches around the great arteries. This coding system is applicable to (anomalous) coronary arteries and bicuspid aortic valves (BAV) irrespective of the position of the great arteries. In this way, the coronary anatomy can be uniformly described in all cases, independently of the cardiac anatomy.7
Over the past decades, the Leiden Convention has been widely used among surgeons.3,8–10 The coding system considers the coronary anatomy from a cranial view, as encountered during cardiac surgery (Figure 1). This is, however, not the view derived from imaging techniques in use by (paediatric) cardiologists. In both computed tomography (CT) angiography and transthoracic echocardiography (TTE), the preferred tools for delineation of the coronary artery anatomy in (paediatric) cardiology, the physician’s view is from caudal to cranial, and the coronary anatomy is viewed from the base of the aorta upward (Figure 1). Using the modified Leiden Convention (i.e. from a surgical point of view, Figure 2, left panels) for CT or TTE may result in inadequate anatomical descriptions.10,11

The surgeon’s view vs. the cardiologist’s view. A, anterior; Ao, aorta; L, left; LAD, left anterior descending artery; LCA, left coronary artery; LCx, circumflex artery; NF, non-facing sinus; P, posterior; Pu, pulmonary artery; R, right; RCA, right coronary artery.
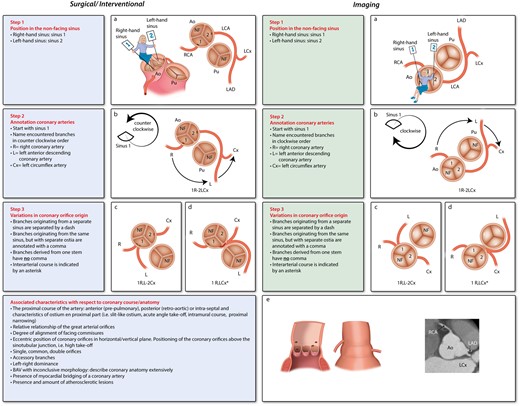
The surgical and interventional Leiden Convention (left) and the imaging Leiden Convention (right). Ao, aorta; LAD, left anterior descending artery; LCA, left coronary artery; LCx, circumflex artery; NF, non-facing sinus; Pu, pulmonary artery; RCA, right coronary artery. Figure derived and modified with permission from Gittenberger-de Groot et al.7
Correct diagnosis of the coronary anatomy is especially important prior to surgery in patients with congenital heart disease to facilitate the identification of patients at high-risk for surgery. In adults, a CT scan is preferred to magnetic resonance imaging (MRI) or TTE because of better spatial resolution.12–14 Another advantage of CT is that the results are operator-independent.11 In paediatric cardiology, TTE (using the parasternal short axis) is more often used to visualize the coronary anatomy. Children often have better echocardiographic windows than adults and TTE has the additional advantage of no radiation exposure, in contrast to CT scanning.14 Coronary artery anomalies after arterial switch operation are encountered frequently after surgery15 justifying repeated imaging with CT-angiography and TTE for follow-up by (paediatric) cardiologists after surgery.16,17
Since cardiac surgeons and cardiologists work closely together, it is important that they can use the same coding system when describing coronary anatomy. The feasibility for clinical use of a coronary coding system is largely determined by whether or not the coronary anatomy can be uniformly noted and easily preted. Here, we present the ‘imaging Leiden Convention’ (Figure 2, right panels), a coding system designed for uniform use in CT scans, MRI scans, and the TTE parasternal short axis. The hallmark feature is that the description of coronary anatomy is the same for all imaging techniques used and conform the description used for the surgical view (the ‘classical’ Leiden Convention that will further be referred to as ‘surgical Leiden Convention’). To provide a truly interdisciplinary coding system, methods for coronary angiography (CAG), which adhere to the surgical Leiden Convention, are also provided.
Methods and results
Principles of the surgical Leiden Convention
An important aspect of the surgical Leiden Convention is the terminology of the aortic sinuses. Rather than indicated as left coronary sinus, right coronary sinus, and non-coronary sinus according to the coronary artery originating from it, an unambiguous classification was made.7 In this way, the ambiguity that arises in case of malposition of the great arteries is avoided. In all hearts, as a general rule, two of the aortic sinuses face the pulmonary valve and one does not. The sinus that does not face the pulmonary valve is accordingly named ‘non-facing sinus’. The annotation of the coronary arteries is carried out in three simple steps (Figure 2, left panels). In Step 1, the physician takes place in the non-facing sinus, looking towards the pulmonary valve. In that position, the sinus on the right hand is called ‘sinus 1’ and the sinus on the left hand ‘sinus 2’. This can be applied independently of how the great arteries are aligned relative to each other or of the position of the aortic valve in the body. In Step 2, starting in sinus 1, the encountered coronary branches are named (‘L’ for left anterior descending (LAD), ‘Cx’ for left circumflex artery (LCx), and ‘R’ for right coronary artery (RCA)) in a counter-clockwise order. In Step 3, variations of the coronary orifices are annotated. Coronary arteries originating from different sinuses are separated by a dash, branches from the same sinus but with separate orifices are separated by a comma. Because of its clinical importance with an increased risk of sudden cardiac death,12–14,18 an interarterial proximal course of a coronary artery is clearly marked using an asterisk in this step. Finally, associated characteristics with respect to coronary course and anatomy are described.
Translation to the imaging Leiden Convention
When applied in the different imaging modalities, the concept of nomenclature of the sinuses is the same. However, adjustments are made to translate the coding system to the views obtained with different imaging modalities.
The imaging Leiden Convention for CT, MRI, and TTE
When changing the perspective from the surgical point of view to the point of view of CT, MRI, or TTE parasternal short axis images, the view on the aorta is changed from a cranial view to a view upward from the left ventricle (Figure 1). In order to maintain the same annotation as the surgical Leiden Convention, again three steps are followed, but with a slight modification (Figure 2, right panels). As a first step, the physician takes place again in the non-facing sinus, but will sit with the back towards the pulmonary valve, looking outwards from the sinus. In this way, the right-hand sinus is still ‘sinus 1’ and the left-hand sinus is ‘sinus 2’. In Step 2, as in the surgical Leiden Convention, the description starts with sinus 1. However, instead of a counter-clockwise fashion, now a ‘clockwise rotation’ is adopted to name the coronary branches. In Step 3, variations in coronary orifice origin are again described, using the same principles as in the surgical Leiden Convention and annotated specifically so that the user will recognize clearly from which sinus the coronary artery originates. Also described in this step is the interarterial course with an asterisk. Other proximal courses and associated characteristics are described separately, similar to the surgical coding system. All CT, echocardiography, and angiography images used for the figures below were obtained in the setting of standard clinical care.
Application of the coronary coding system
In the most common anatomical pattern, the RCA (annotated as ‘R’ in the Leiden Convention) arises from sinus 1, and the left coronary artery (LCA), branching into the LAD (annotated as ‘L’), and LCx (annotated as ‘Cx’), arises from sinus 2. Following the steps of the imaging Leiden Convention, this leads to the description: 1R-2LCx (Figure 2, right panel B), the same as the annotation in the surgical Leiden Convention (Figure 2, left panel B).
Figure 3 shows the results of applying the imaging Leiden Convention to TTE and CT images.
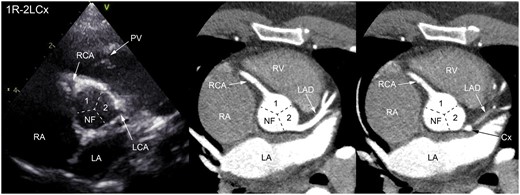
Normal coronary anatomy (1R-2LCx) on echocardiogram and computed tomography scan. The coronary anatomy is seen on two different trans-axial levels in one patient. Cx, circumflex artery; LA, left atrium; LAD, left anterior descending artery; LCA, left coronary artery; NF, non-facing sinus; PV, pulmonary valve; RA, right atrium; RCA, right coronary artery; RV, right ventricle.
In Figure 4, examples of application of the imaging Leiden Convention are shown for anomalous coronary arteries and TGA on TTE and CT.
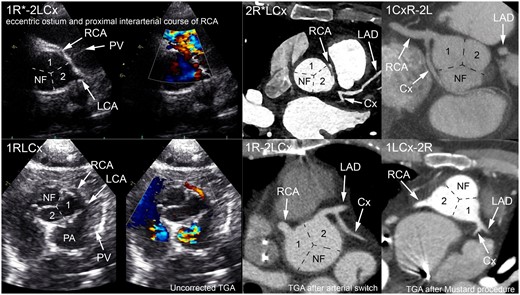
Examples of the application of the imaging Leiden Convention for anomalous coronary arteries and transposition of the great arteries on echocardiogram (with and without colour Doppler) and computed tomography scan. Cx, circumflex artery; LAD, left anterior descending artery; LCA, left coronary artery; NF, non-facing sinus; PA, pulmonary artery; PV, pulmonary valve; RCA, right coronary artery; TGA, transposition of the great arteries.
The surgical Leiden Convention for CAG
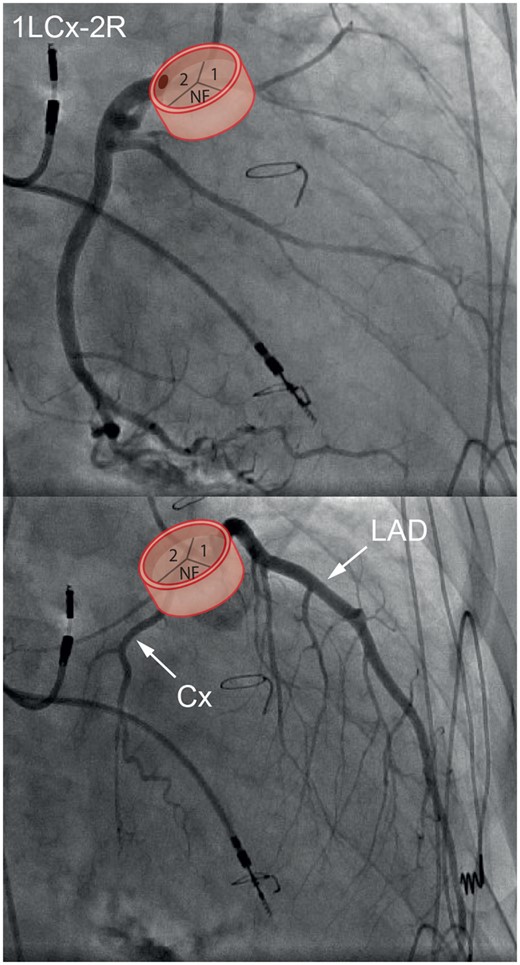
CAG is also an often used tool in cardiology, so it is important that the Leiden Convention is also applicable to this modality (Figure 5). Of interest, for CAG images the surgical Leiden Convention is the appropriate method to describe the coronary anatomy. As a general rule, the ‘non-angulated right anterior oblique (RAO) 30° projection’ must be used. This view is best suitable for detection of anomalous coronary arteries.18 In this projection, the most common variations of origin and proximal course can be distinguished in both normally related great arteries and TGA. Step 1 starts again with defining the location of the non-facing sinus and the annotation of sinus 1 and 2. This differs between patients with a normal relationship of the great arteries and patients with uncorrected TGA or after Mustard or Senning procedure. For normally related great arteries, in the RAO 30° view the non-facing sinus is posteriorly located in the aortic root (Figure 5). For patients with TGA, the non-facing sinus is anteriorly located in the aortic root on CAG images (Figure 6). Sinus 1 is on the right-hand side and sinus 2 is on the left-hand side when taking position in the non-facing sinus as described for the surgical Leiden Convention (Figures 2 and 5). In Step 2, the annotation of the coronary arteries is done using a ‘counter-clockwise rotation’ starting from sinus 1. Variations in coronary orifice origin and an eventual interarterial course are described in Step 3. After Step 3, additional characteristics are described.
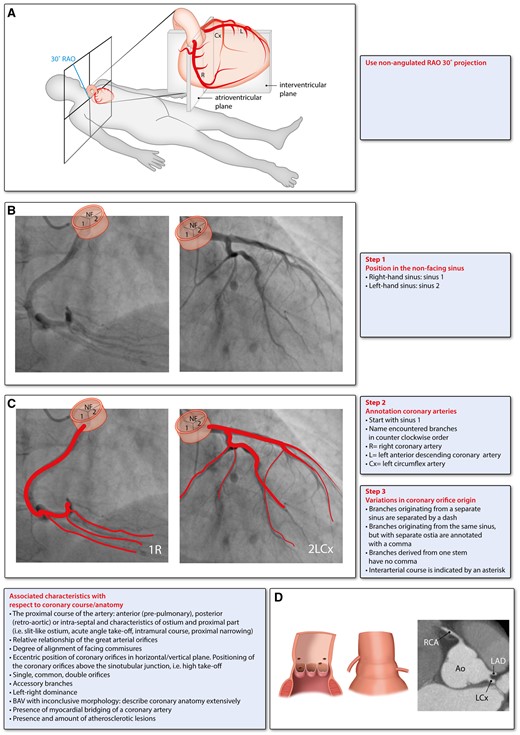
The surgical Leiden Convention for coronary angiography. Ao, aorta; BAV, bicuspid aortic valve; LAD, left anterior descending artery; LCx, circumflex artery; RAO, right anterior oblique; RCA, right coronary artery; NF, non-facing sinus. The bottom panels are derived and modified with permission from Gittenberger-de Groot et al.7
Non-angulated right anterior oblique 30° view of patient with transposition of the great arteries after Mustard procedure. Cx, circumflex artery; LAD, left anterior descending artery; NF, non-facing sinus.
To correctly describe an interarterial, pre-pulmonary, retro-aortic, or intra-septal course in Step 3 or as additional characteristic, the ‘dot and eye method’ from Serota et al.19 can be used. Examples of coronary anomalies are shown for normally related great arteries in Figure 7. A vessel seen ‘on end’ during CAG will appear as a ‘dot’. This is the case in the non-angulated RAO 30° view of an interarterial RCA (Figure 7A) and a retro-aortic or interarterial LCA (Figure 7B). An ‘eye’ can be seen in non-angulated 30° RAO when the LCA or LAD and LCx project above and below one another, forming an ellipse (Figure 7C). Depending on which arteries form the upper and the lower parts, the coronary artery course can be determined. For example, when the LCA forms the inferior part and the LCx the superior part, the left main stem originating from sinus 1 courses intra-septal (Figure 7C).
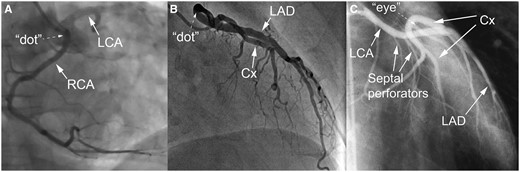
(A) RCA from sinus 2 with interarterial course. Note more intense contrast proximally, because vessel is seen on end (‘dot’). (B) LCA from sinus 1 with interarterial course (RCA not visualized). Note more intense contrast proximally, because vessel is seen on end (‘dot’). (C) LCA from sinus 1 with septal course (RCA not visualized). Cx, circumflex artery; LAD, left anterior descending artery; LCA, left coronary artery; RCA, right coronary artery. Images derived and modified with permission from Vliegen et al.18
Table 1 provides assistance for translating the CAG-images to a description according to the Leiden Convention.
| Anomalous coronary artery | Course | Appearance |
|---|---|---|
| RCA from sinus 2 | ||
Anterior 2R(,)LCx | Anterior to pulmonary artery | Coursing slightly forward, then turning backwards to atrioventricular groove |
| Posterior 2LCX(,)R | Posterior to aorta | ‘Dot’, turning around the aorta in the direction of the spine Very uncommon variation |
Interarterial 2R*(,)LCx | Between aorta and pulmonary artery At, below or above level of pulmonary valve | ‘Dot’, seen in proximal course of RCA (Figure 7A) |
| LCA/LAD from sinus 1 | ||
Anterior 1R(,)LCx 1R(,)L-2Cx | Anterior to pulmonary artery | ‘Eye’ configuration with LCx in atrioventricular groove |
Posterior 1LCx(,)R | Posterior to aorta | ‘Dot’, originating close to RCA and turning posterior to aorta |
Interarterial 1R(,)LCx* 1R(,)L*-2Cx | Between aorta and pulmonary artery At, below or above level of pulmonary valve | ‘Dot’, seen in proximal course of LCA (Figure 7B) |
Intra-septal 1R(,)LCx 1R(,)L-2Cx | Through inter-ventricular septum | ‘Hammock’ appearance of left main stem, ‘eye’ formed by LCx and left main stem, 1st septal branch arises from proximal left main stem (Figure 7C) |
| LCx from sinus 1 | ||
Posterior 1Cx(,)R-2L | Posterior to aorta | Posterior course with ‘dot’ |
| Anomalous coronary artery | Course | Appearance |
|---|---|---|
| RCA from sinus 2 | ||
Anterior 2R(,)LCx | Anterior to pulmonary artery | Coursing slightly forward, then turning backwards to atrioventricular groove |
| Posterior 2LCX(,)R | Posterior to aorta | ‘Dot’, turning around the aorta in the direction of the spine Very uncommon variation |
Interarterial 2R*(,)LCx | Between aorta and pulmonary artery At, below or above level of pulmonary valve | ‘Dot’, seen in proximal course of RCA (Figure 7A) |
| LCA/LAD from sinus 1 | ||
Anterior 1R(,)LCx 1R(,)L-2Cx | Anterior to pulmonary artery | ‘Eye’ configuration with LCx in atrioventricular groove |
Posterior 1LCx(,)R | Posterior to aorta | ‘Dot’, originating close to RCA and turning posterior to aorta |
Interarterial 1R(,)LCx* 1R(,)L*-2Cx | Between aorta and pulmonary artery At, below or above level of pulmonary valve | ‘Dot’, seen in proximal course of LCA (Figure 7B) |
Intra-septal 1R(,)LCx 1R(,)L-2Cx | Through inter-ventricular septum | ‘Hammock’ appearance of left main stem, ‘eye’ formed by LCx and left main stem, 1st septal branch arises from proximal left main stem (Figure 7C) |
| LCx from sinus 1 | ||
Posterior 1Cx(,)R-2L | Posterior to aorta | Posterior course with ‘dot’ |
LAD, left anterior descending artery; LCA, left coronary artery; LCx, circumflex artery; RCA, right coronary artery.
| Anomalous coronary artery | Course | Appearance |
|---|---|---|
| RCA from sinus 2 | ||
Anterior 2R(,)LCx | Anterior to pulmonary artery | Coursing slightly forward, then turning backwards to atrioventricular groove |
| Posterior 2LCX(,)R | Posterior to aorta | ‘Dot’, turning around the aorta in the direction of the spine Very uncommon variation |
Interarterial 2R*(,)LCx | Between aorta and pulmonary artery At, below or above level of pulmonary valve | ‘Dot’, seen in proximal course of RCA (Figure 7A) |
| LCA/LAD from sinus 1 | ||
Anterior 1R(,)LCx 1R(,)L-2Cx | Anterior to pulmonary artery | ‘Eye’ configuration with LCx in atrioventricular groove |
Posterior 1LCx(,)R | Posterior to aorta | ‘Dot’, originating close to RCA and turning posterior to aorta |
Interarterial 1R(,)LCx* 1R(,)L*-2Cx | Between aorta and pulmonary artery At, below or above level of pulmonary valve | ‘Dot’, seen in proximal course of LCA (Figure 7B) |
Intra-septal 1R(,)LCx 1R(,)L-2Cx | Through inter-ventricular septum | ‘Hammock’ appearance of left main stem, ‘eye’ formed by LCx and left main stem, 1st septal branch arises from proximal left main stem (Figure 7C) |
| LCx from sinus 1 | ||
Posterior 1Cx(,)R-2L | Posterior to aorta | Posterior course with ‘dot’ |
| Anomalous coronary artery | Course | Appearance |
|---|---|---|
| RCA from sinus 2 | ||
Anterior 2R(,)LCx | Anterior to pulmonary artery | Coursing slightly forward, then turning backwards to atrioventricular groove |
| Posterior 2LCX(,)R | Posterior to aorta | ‘Dot’, turning around the aorta in the direction of the spine Very uncommon variation |
Interarterial 2R*(,)LCx | Between aorta and pulmonary artery At, below or above level of pulmonary valve | ‘Dot’, seen in proximal course of RCA (Figure 7A) |
| LCA/LAD from sinus 1 | ||
Anterior 1R(,)LCx 1R(,)L-2Cx | Anterior to pulmonary artery | ‘Eye’ configuration with LCx in atrioventricular groove |
Posterior 1LCx(,)R | Posterior to aorta | ‘Dot’, originating close to RCA and turning posterior to aorta |
Interarterial 1R(,)LCx* 1R(,)L*-2Cx | Between aorta and pulmonary artery At, below or above level of pulmonary valve | ‘Dot’, seen in proximal course of LCA (Figure 7B) |
Intra-septal 1R(,)LCx 1R(,)L-2Cx | Through inter-ventricular septum | ‘Hammock’ appearance of left main stem, ‘eye’ formed by LCx and left main stem, 1st septal branch arises from proximal left main stem (Figure 7C) |
| LCx from sinus 1 | ||
Posterior 1Cx(,)R-2L | Posterior to aorta | Posterior course with ‘dot’ |
LAD, left anterior descending artery; LCA, left coronary artery; LCx, circumflex artery; RCA, right coronary artery.
Description of associated characteristics with respect to coronary course and anatomy
In some cases, the annotation does not provide all anatomical characteristics that can be of importance when planning a catheter intervention or surgical procedure, e.g. in case of an intramural course or myocardial bridging of a vessel. In these cases, additional information should be noted separately (Figures 2 and 5, bottom panels). This additional information includes the following:
The proximal course of the artery: anterior (pre-pulmonary), posterior (retro-aortic), or intra-septal. An interarterial course is already specified in Step 3 by an asterisk. In case of an interarterial course also note in this step whether the interarterial part courses at, below or above the level of the pulmonary valve.
Additional information on the proximal course of the coronary artery, i.e. shape of the coronary orifice, acute angle take-off, intramural course, and proximal narrowing. This information is especially important for arteries that follow an interarterial course, as this has implications for the risk of sudden cardiac death.12–14 Definitions for the shape of the coronary orifice are provided by the Texas Children’s Hospital: round (anterior–posterior diameter is the same as the transverse diameter), oval (transverse diameter is 50–90% of anterior–posterior diameter), and slit-like (transverse diameter is <50% of anterior–posterior diameter).20
Eccentric position of coronary orifices within the sinus and positioning of the coronary orifices relative to the sinotubular junction, i.e. high take-off. For a more detailed description of these characteristics, the topography map from the Texas Children’s Hospital can be used.21
Presence of single, common, or double orifices (this can also be derived from the annotation, from the presence, or absence of the comma).
Presence of accessory branches originating from the coronary sinuses, this includes the sinoatrial node branch and a potential conus artery.
Coronary artery system dominance: right, left, or co-dominant system.
Presence of myocardial bridging of a coronary artery.
Presence and degree of atherosclerotic lesions.
The position of the great arteries relative to each other and the alignment of the facing commissures. This is important in an arterial switch procedure to determine the site of relocation of the buttons of the new coronary orifices.
Coronary coding in BAV
Separate attention needs to be paid to BAV (Figure 8). Three main morphological BAV types can be distinguished based on which leaflets are conjoined: (i) Type 1 in which the leaflets of sinus 1 and 2 are conjoined; (ii) Type 2 in which the leaflets of sinus 1 and the non-facing sinus are conjoined; and (iii) Type 3 in which the leaflets of sinus 2 and the non-facing sinus are conjoined. The types can be further subdivided in types with and without a raphe (the latter referred to as ‘strictly bicuspid’).
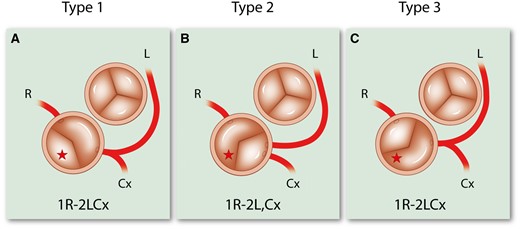
The Leiden Convention applied to bicuspid aortic valves. The star marks the non-facing sinus. Cx, circumflex artery; L, left anterior descending artery; R, right coronary artery.
For BAV, the Leiden Convention can be used, because in 99% of cases the coronary arteries connect to sinus 1 and 2 and as the non-facing sinus are non-coronary, the sinus annotation can thus be deduced.7 For strictly bicuspid valves (no raphe), this can be difficult. As described before by Gittenberger-de Groot et al.,7 the reasoning can be reversed in these cases. Using the Leiden Convention, it can be deduced which valve leaflets are fused, and where the non-facing sinus is. Once this is determined, the Leiden Convention can be applied.
In case the type of BAV cannot be determined, a descriptive approach is advised.
Applicability and feasibility
To assess practical applicability and feasibility in clinical practice of the imaging Leiden Convention, the coding system was tested using images of the various imaging modalities. Two congenital cardiologists and four cardiology residents assessed CT and MRI images. Two paediatric cardiologists and two cardiology residents assessed TTE images, and one interventional cardiologists and two cardiology residents assessed CAG images in RAO 30° view. All physicians received a brief explanation of the coronary coding system, followed by one exercise case, after which the physicians were asked to score 5 or 6 images according to the Leiden Convention coding system. Figures 2 and 5 and Table 1 were provided as instruction manuals for assessing the images.
A total score of 3 points could be obtained per case. The scores were appointed per correctly followed step. Points per step were rewarded as follows:
Step 1: correct sinus annotation: 1 point, if incorrect: 0 points.
Step 2: per correctly identified coronary artery, in the right order and from the correct sinus: 1/3 point (total of 1 point).
Step 3: 1 point if correct, −1/2 point if mistake is made in comma, asterisk, or dash annotation. Two mistakes are thus 0 points.
Test results
The average score on all three modalities was 87,5%. For CT and MRI, average score was 90%. On TTE participants scored an average percentage of 83%, and for CAG 88%. The scores on all imaging modalities were consistently high (Figure 9). Figure 9 also shows the average score per rater per modality and the mean scores per case per modality. Most mistakes were made in Step 3 (67% of all mistakes). Usually, this was the incorrect placement of the comma or forgetting to use the asterisk.
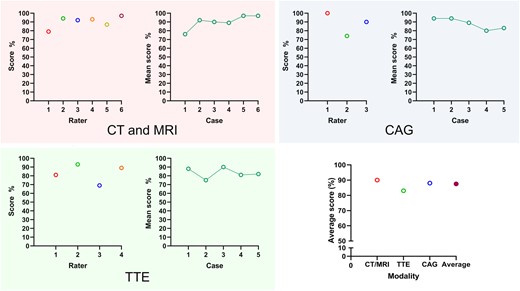
Result of the applicability and feasibility test among physicians: average score per rater, average score per case, and overall average of scores per imaging modality. Results show that the methods can be easily mastered and that applicability and feasibility for use in daily practice are high. CAG, coronary angiography; CT, computed tomography; MRI, magnetic resonance imaging; TTE, transthoracic echocardiogram.
Discussion of applicability and limitations
In this study, we introduce an extrapolation of the Leiden Convention coronary coding system. This system is already widely implemented in surgical practice and has now been modified for use in cardiac imaging techniques. Assessment of the applicability and feasibility of the imaging Leiden Convention shows that it can easily be implemented by colleagues of various experience after uniform short introduction and the results are likely to further improve with an increasing learning curve.
Applicability for CT and MRI
For CT and MRI, the imaging Leiden Convention is practically applicable. There was a clear learning curve: after the first few cases, the results during the test improved with each case, as shown in Figure 9.
Applicability for TTE
For TTE still frames were used. However, all participating cardiologists and residents are used to looking at moving images on TTE and the possibility of searching for the best view. Also, colour Doppler is often used to improve coronary artery visibility which was not available on all images presented. We therefore expect the application of the coding system to be even more feasible in daily practice than it already proved to be in the test. It is advised to use colour Doppler with a low Nyquist limit (e.g. 0.14) to optimize coronary artery visibility. Finding the coronary arteries using echocardiography can be challenging, especially in adults. However, if the coronary arteries are adequately visualized, such as in children, application of the imaging Leiden Convention proved well feasible.
Applicability for CAG
The applicability for CAG was tested on one interventional cardiologist and two cardiology residents. The interventional cardiologist could describe the coronary anatomy based on the RAO 30° view. Due to his experience, he used a ‘reversed method’ to describe the anatomy according to the Leiden Convention. He recognized the anatomy and anomalies, and then wrote down the correct annotation, scoring a maximum of 100%. In clinical practice, this is how most experienced cardiologists will use the coding system. For the cardiology residents with different amounts of experience with CAG, assessment based on the still frame images alone, proved difficult because of their inexperience with TGA (Cases 4 and 5) and coronary anomalies on CAG. With the assistance of Table 1, description of the coronary anatomy annotation was feasible. It was commented by the participants that moving CAG images and the possibility of looking from different angles would make using the Leiden Convention easier for CAG, but that in principle the method can be adequately applied. In clinical practice, clinicians will have the availability of moving images to interpret the anatomy, likely rendering its applicability more feasible than during the test cases.
Overall, it can be concluded that the applicability and feasibility of the Leiden Convention in daily practice are high and the methods can be easily mastered.
Limitations
The great advantage of the Leiden Convention coronary coding system lies in the applicability in different forms of congenital heart disease, as it can be applied irrespective of the position of the great arteries. However, there are a few limitations to the system. The Leiden Convention is not applicable in the absence of a pulmonary artery (i.e. in pulmonary atresia), in truncus arteriosus communis, quadricuspid aortic valves, and in cases where the aortic valve morphology cannot be adequately distinguished. In these anomalies, a descriptive approach is recommended. If a coronary artery arises from the pulmonary artery, the Leiden Convention can be applied to the normally arising artery and description of the coronary artery from the pulmonary artery should be done as an associated characteristic.
Of note, the Leiden Convention coronary coding system is not meant to replace direct contact and discussion between cardiologists and cardiac surgeons. Rather, it is a tool to render communications unambiguous for written reports and to support the discussion whilst reviewing images of patients.
Conclusions
The imaging Leiden Convention is a simple coronary coding system that unifies the annotation of the coronary anatomy for cardiac surgeons, cardiologists, and radiologists. Reviewing the applicability and feasibility of the coding system shows that it is can be easily and reliably applied and mastered in clinical practice. It is applicable to CT, MRI, and TTE. For CAG, the surgical Leiden Convention can be applied and also proved to be reliably applicable. Reviewing dynamic images is recommended to facilitate the use of the coding system. The Leiden Convention has the potential to improve the communication between cardiac surgeons and (paediatric) cardiologists by providing in a systematic interdisciplinary coronary artery coding system.
Acknowledgements
We greatly acknowledge Mr. Slagter for drawing the graphical abstract and Figures1, 2, 5, 6, and 8.
In respectful memory of Adriana C. Gittenberger-de Groot, without whom the Leiden Convention coronary coding system would not have existed.
Data availability
The data underlying this article will be shared on reasonable request to the corresponding author.
Conflict of interest: none declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}