





Abstract
As a derivative of adipose tissues, stromal vascular fraction gel has been widely utilized in facial soft tissue filling, but it still does not achieve the expected effect in forehead filling. The reason may be related to the corrugator muscles movements.
The authors aimed to evaluate the effect of botulinum toxin-A (BTX-A) on the retention rate of stromal vascular fraction gel by limiting the corrugator muscles movements and to provide a theoretical basis that short-term inhibition of movement in the affected area could improve the effects of the fat graft.
From January 2019 to June 2021, patients with stromal vascular fraction gel facial filling (including frontal and temporal parts) were selected. According to whether or not BTX-A treatment was received, patients were divided into injected and the noninjected groups. A questionnaire and the Global Aesthetic Improvement Scale (GAIS) were administered to evaluate 2-dimensional photos. The retention rate and curvature were calculated with 3-dimensional images utilizing Artec Studio 13 Professional and MATLAB software.
The graft retention, forehead curvature, and GAIS scores were all higher in the injected group than the noninjected group (P < .01). On the questionnaire, the injected group also showed more satisfaction with the treatment effect and were more willing to recommend the treatment to their friends.
BTX-A injection can improve the retention rate of prefrontal stromal vascular fraction gel filling, with higher patient satisfaction and better postoperative effects.

Unlike Western aesthetics, a large and gently curved forehead is regarded as a symbol of beauty and flat foreheads symbolize masculinity and aging in Asian females.1 Facial contour plastic surgery, especially on the forehead, is becoming more popular among Asians.2–5
Autologous fat transplantation is widely utilized in facial rejuvenation.6–10 However, its unstable retention rate is unsatisfying for various reasons.11,12 Some studies have shown that stromal vascular fraction gel as a derivative of autologous fat is often employed to fill the facial soft tissues.13,14 Because it is prepared by a process of centrifugation and inter-syringe shifting, stromal vascular fraction gel has fewer destroyed adipocytes and a higher content of adipogenic stem cells, vascular endothelial cells, and native extracellular matrix, and the filling effect is satisfactory.15–18 However, there is concern about long-term retention of the graft when utilized in the frontal region, because it may be impacted by frequent movement of the muscles in the forehead, such as when lifting the eyebrows or burrowing the eyebrows while frowning. Frequent movement may lead to a quicker loss of the graft, and so a quicker return to the patient's baseline appearance. Therefore, it is reasonable to assume that the retention rate may be affected by weakening or inhibiting the movements of the corrugator muscles for a short time before filling.
This study aimed to evaluate the effect of botulinum toxin-A (BTX-A) on the retention rate of stromal vascular fraction gel by injection into the enthesis of the bilateral corrugator muscles to limit frowning and demonstrate whether or not short-term inhibition of movement in the affected area could improve the effects of the fat graft.
METHODS
Patient Enrollment
The study protocol was approved by the institutional review board of the First Affiliated Hospital of Harbin Medical University, and all patients provided written informed consent. From January 2019 to June 2021, patients treated with stromal vascular fraction gel filling to the forehead by the same plastic surgeon at our center were selected. Patients who had (1) a history of diabetes, hypertension, cardiovascular or infectious diseases; (2) a history of frontal BTX-A injection, frontal filling, or other surgeries in the 6 months before treatment and during follow-up; (3) a body mass index change that was greater than 1 within 6 months after treatment; or (4) incomplete data or insufficient follow-up (less than 6 months) were excluded. The enrolled patients were divided into injected and noninjected groups, according to whether they received preoperative BTX-A injection in the corrugator muscles or not.
BTX-A Injection
The movements of eyebrow lifting and frowning showed the specific location of the prefrontal muscles (Figure 1 A, B, C). In these areas, the injection group was administered BTX-A (Botox; Allergan, Irvine, CA) 3 to 7 days in advance. BTX-A, 50 U, was dissolved into 1.25 mL of normal saline; 4 U of BTX-A was injected into the belly of both corrugator muscles, 2 U into the superficial terminations of the corrugator muscles, and 4 U into the middle of the superciliary depressor muscle with a 30-gauge needle. The dose and injection sites were adjusted based on the characteristics of the corrugator muscles. The same surgeon performed all procedures.

Photographs of a normal 27-year-old female. (A) No expression; (B) frown movement; and (C) eyebrow lifting.
Stromal Vascular Fraction Gel Preparation and Filling
The frontotemporal area was divided into 5 regions (Figure 2): the temporal regions were the yellow zones (area I); the side forehead regions had 2 inner boundaries that clung to the prefrontal region, with lateral boundaries at the frontotemporal line (area II); and the prefrontal region, where the lateral boundary was at the midpoint between the inner and outer canthi on each side, the upper boundary was the hairline, and the lower boundary was at the upper intersection of both eyebrows (area III). The prefrontal region (area III) was the main object of this study.
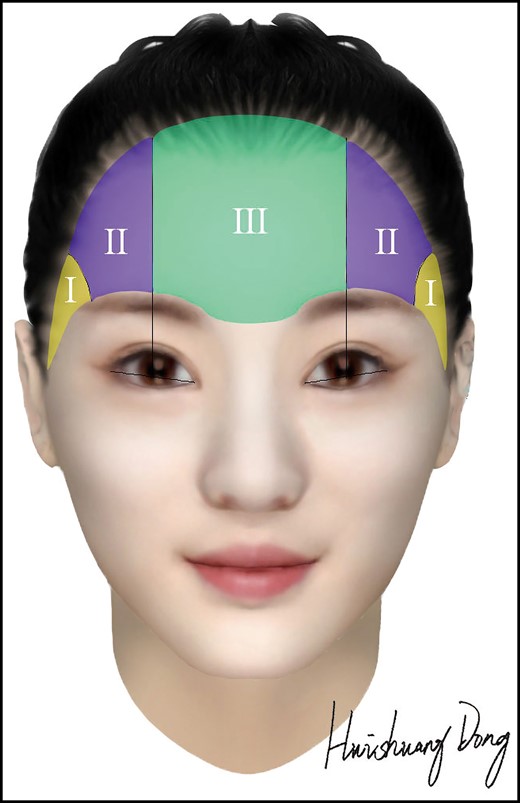
Partition map of frontal and temporal areas. Created by and reproduced with permission from the artist, Huishuang Dong.
Patients underwent fat suction under general anesthesia, and the fat was prepared into stromal vascular fraction gel according to the following process.14 The lipoaspirate was centrifuged at 1200×g for 3 minutes to obtain Coleman fat in the middle layer. Then, the Coleman fat was transferred to a piece of equipment that consisted of two 20-mL syringes connected by a luer-lock connector (internal diameter of 1.4 mm) and mechanically emulsified by shifting at a rate of 10 mL per second for 1 minute. The uniform emulsion was then centrifuged at 2000×g for 3 minutes, and the sticky substance under the oil layer was identified as stromal vascular fraction gel for further use.14
Filling with stromal vascular fraction gel for both injected and noninjected groups was first done in the temporal parts, then the side forehead and prefrontal parts. Patients were in a supine position and had local infiltration anesthesia of 0.75% lidocaine. The stromal vascular fraction gel was injected into the connective tissues below the deep temporal fascia and frontalis muscle with an 18-gauge cannula. The filling volume of each part was recorded separately.
Data Acquisition and Analysis
When this retrospective study began, all patients completed an anonymous questionnaire by phone or email, Patients could choose from 1 of the 4 options, stating that they disagreed, neither disagreed nor agreed, agreed, or strongly agreed with 3 statements: (1) The low and flat forehead has been significantly improved from the front view; (2) the curve of the forehead is more beautiful from the side view; and (3) I would recommend the same treatment to my friends.
Photographs and 3-dimensional (3D) images of all patients taken before and 6 months after treatment were collected for observation and data measurement. Photographs were taken with a digital camera (Nikon D90; Nikon, Minato, Tokyo, Japan). The photos were assessed by 3 professional plastic surgeons (who were not involved in the surgical procedure and blinded of the grouping) according to the Global Aesthetic Improvement Scale (GAIS) (Table 1).
Global Aesthetic Improvement Scale
| Score | Grade | Delineation |
|---|---|---|
| −1 | Worse | Appearance worse than original condition |
| 0 | No change | Appearance essentially the same as original condition |
| 1 | Improved | Obvious improvement but touch-up or retreatment indicated |
| 2 | Much improved | Marked improvement in condition, but not optimal for the patient; touch-up would slightly improve the result |
| 3 | Very much improved | Optimal cosmetic result for the patient |
| Score | Grade | Delineation |
|---|---|---|
| −1 | Worse | Appearance worse than original condition |
| 0 | No change | Appearance essentially the same as original condition |
| 1 | Improved | Obvious improvement but touch-up or retreatment indicated |
| 2 | Much improved | Marked improvement in condition, but not optimal for the patient; touch-up would slightly improve the result |
| 3 | Very much improved | Optimal cosmetic result for the patient |
Global Aesthetic Improvement Scale
| Score | Grade | Delineation |
|---|---|---|
| −1 | Worse | Appearance worse than original condition |
| 0 | No change | Appearance essentially the same as original condition |
| 1 | Improved | Obvious improvement but touch-up or retreatment indicated |
| 2 | Much improved | Marked improvement in condition, but not optimal for the patient; touch-up would slightly improve the result |
| 3 | Very much improved | Optimal cosmetic result for the patient |
| Score | Grade | Delineation |
|---|---|---|
| −1 | Worse | Appearance worse than original condition |
| 0 | No change | Appearance essentially the same as original condition |
| 1 | Improved | Obvious improvement but touch-up or retreatment indicated |
| 2 | Much improved | Marked improvement in condition, but not optimal for the patient; touch-up would slightly improve the result |
| 3 | Very much improved | Optimal cosmetic result for the patient |
Three-dimensional images of all patients were obtained with an Artec EVA 3D Scanner (Artec Europe Sàrl, Senningerberg, Luxembourg). The cloud point data were initially reconstructed to obtain a clear 3D facial image with the Artec Studio Professional software (Artec Europe Sàrl). Three points (α, β, γ) were established in accordance with the characteristics of the prefrontal region (area III). Points α and β were at the intersections of the 2 lateral boundaries with the lower boundary of area III, respectively, and point γ was the midpoint of the frontal hairline (Figure 3). A plane defined by the 3 points was adopted to cut the overlapping 3D image to produce an enclosed area. The software was utilized to measure the volume before and after treatment and calculate the difference. The retention rate of the fat graft was the ratio of the volume difference of the area to the forehead filling amounts cited in the treatment records.
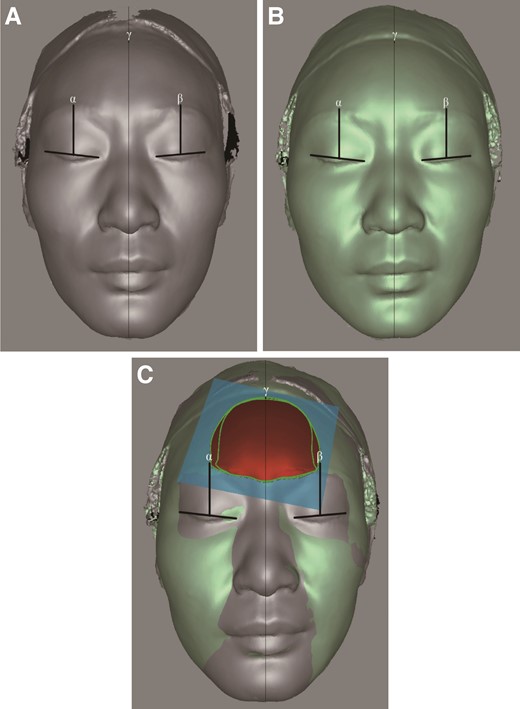
Schematic images of volumetric measurements obtained with Artec Studio 13 professional software (A) Before treatment; (B) 6 months after treatment; and (C) overlapping images of before and after treatment.
The 3D images before and after treatment were overlapped, and the software generated the fusion image as a colored height map. Red indicated that the height had increased, and blue indicated a decrease in height from the pretreatment height. The darker the color, the more pronounced the change in height.
Curvature is a metric of geometry; the higher the number, the larger the radian. According to 3D images obtained by scanning, the intersection of the anterior median and hairline was defined as point A, the intersection with brow level as point B, and the midpoint of the arc between points A and B was point C (Figure 4A). Due to the distribution characteristics of the corrugator muscles, arc BC was the focus for curve changes (Figure 4B). The contour drawing was copied with the profiles of the overlapped 3D images, and the maximum curvature was calculated by the MATLAB software (Natick, MA; Figure 4C).

Curvature measurements obtained with MATLAB software (A) Selection of measurement points; (B) side view of the curve; and (C) curvature circle.
SPSS 26.0 software (IBM, Armonk, NY) was utilized for statistical analysis, a rank-sum test for GAIS scores, Fisher's exact test for patient satisfaction, and independent sample t-tests for retention rate and curvature changes. A value of P < .05 was considered statistically significant.
RESULTS
From January 2019 to June 2021, 167 patients underwent treatment with stromal vascular fraction gel to the forehead by the same surgeon. Seventy-nine patients had complete follow-up data and met the enrollment criteria. There were 41 cases in the injected group and 38 cases in the noninjected group, according to whether or not they received a BTX-A injection in the corrugator muscles. All patients were females, with a mean age of 38.6 (range 24-53). The mean follow-up time was 9.8 months (range 6-11 months). There was no statistically significant difference in age between the 2 groups (P > .05).
Questionnaires were completed by all patients via telephone or email. For the first query (“The low and flat forehead has been significantly improved from the front view”), in the injected group 20 patients (48.78%) chose “strongly agree”; 17 (41.46%) chose “agree”; 4 (9.46%) chose “neither agree nor disagree”; and none chose “disagree.” In the noninjected group 7 patients (18.42%) chose “strongly agree”; 14 (36.84%) chose “agree”; 16 (42.11%) chose “neither agree nor disagree”; and 1 (2.63%) chose “disagree.” For the second (“The curve of the forehead is more beautiful from the side view”), in the injected group 2 patients (53.66%) chose “strongly agree”; 14 (34.15%) chose “agree”; 5 (12.20%) chose “neither agree nor disagree”; and none chose “disagree.” In the noninjected group, 6 patients (15.79%) chose “strongly agree”; 11 (28.95%) chose “agree”; 19 (50.00%) chose “neither agree nor disagree”; and 2 (5.26%) chose “disagree.” Regarding the third item (“I would recommend the same treatment to my friends”), in the injected group 17 patients (41.46%) chose “strongly agree”; 15 (36.59%) chose “agree”; 8 (19.51%) chose “neither agree nor disagree”; and 1 (2.44%) chose “disagree.” In the noninjected group, 6 patients (15.79%) chose “strongly agree”; 12 (31.58%) chose “agree”; 16 (42.11%) chose “neither agree nor disagree”; and 4 (10.53%) chose “disagree.” Generally, patients in the injected group mainly chose “strongly agree,” followed by “agree,” whereas patients in the noninjected group mostly chose “neither agree nor disagree,” followed by “agree” (Figure 5A).
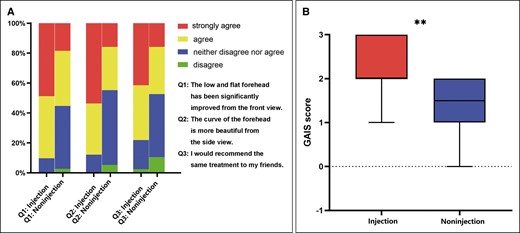
Patient self-evaluation (A) individual responses to each question for the 2 groups; and (B) median of Global Aesthetic Improvement Scale (GAIS) scores for the 2 groups. **P < .01.
Professional surgeons utilized the GAIS to objectively evaluate clinical outcomes. A comparison of the 2-dimensional pretreatment and posttreatment photographs showed that the median GAIS score was 2 for the injected group and 1.5 for the noninjected group. The results were statistically significant (P < .01) (Figure 5B).
Meanwhile, based on the 3D images, the retention rate of injected patients was 70.89% ± 4.18% (range 61.73%-78.72%) and that of noninjected patients was 56.74% ± 1.64% (range 53.86%-60.63%). The results were statistically significant (P < .001; Figure 6). The 3D fusion image also showed that the prefrontal height of the injected group significantly increased when compared with height before treatment (Figure 7A); there was no significant increase observed in the noninjected group (Figure 7B).
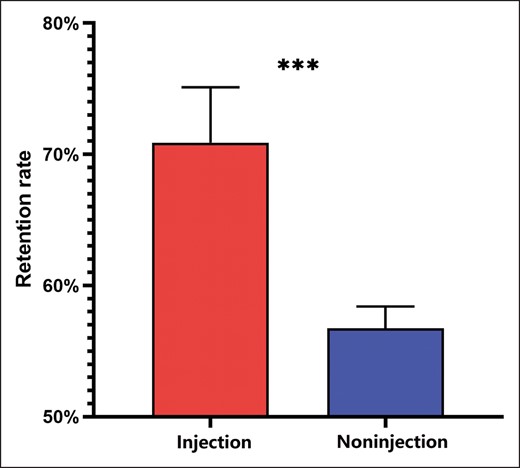
Mean value of retention rates ***P < .001.
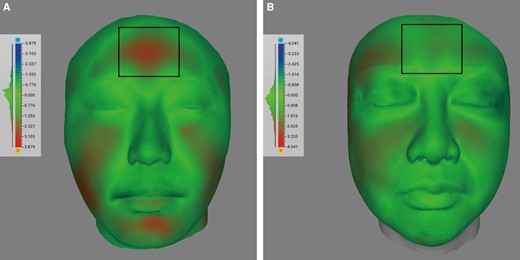
Schematic diagram of facial volume cloud images composited of 3-dimensional scans before and 6 months after treatment (A) Fusion image of patient with botulinum toxin-A (BTX-A) injected; and (B) fusion image of patient without BTX-A injected.
According to the curvature calculated by the software, the maximum curvature difference of the arc of the injection group was 0.2445 ± 0.0345 (range 0.1534-0.3220), and that of the noninjected group was 0.1294 ± 0.0319 (range 0.07016-0.1906). The results were statistically significant (P < .01) (Figure 8).
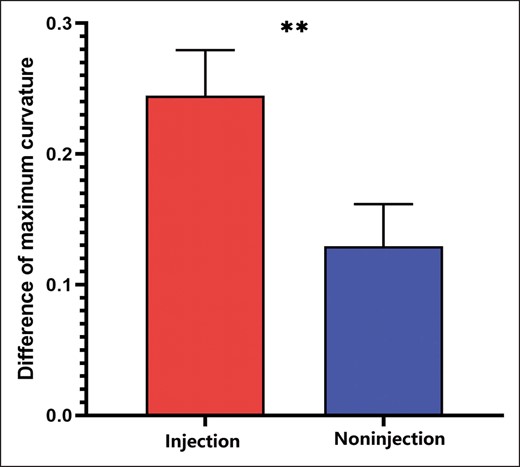
Difference of maximum curvature, **P < .01.
No patients had significant complications such as infection, hematoma, paresthesia, or fat embolism during the follow-up period. Only 2 patients experienced an induration or lump at more than 3 weeks after liposuction, but these were short lived.
Patients
A 34-year-old female with a flat forehead (Figure 9A, C) underwent the frontotemporal filling with BTX-A injection, and the frontal curve had a significant improvement at 6 months after treatment (Figure 9B, D). This patient strongly agreed with all the 3 items on the questionnaire.

Photographs of botulinum toxin-A injection results of a 34-year-old female with a flat forehead (A, C) who showed satisfying postoperative improvements (B, D) with botulinum toxin-A (BTX-A) injection.
A 39-year-old female with a flat forehead (Figure 10A, D) underwent the frontotemporal filling without BTX-A injection, and the frontal curve had a little improvement (Figure 10B, E). In the questionnaire, the patient neither agreed nor disagreed with the first and second queries, and said of the third that she would not recommend the treatment to friends. Fifteen months after the first filling, the patient underwent another frontotemporal filling with BTX-A injection, and significant improvement was observed at 6 months after treatment (Figure 10C, F). After this filling, the patient agreed with the first statement on the questionnaire, strongly agreed with the second, and agreed that she would recommend the treatment to her friends.

Photographs of botulinum toxin-A injection results of a 39-year-old female with a flat forehead (A, D) who showed unsatisfying postoperative improvements (B, E) without botulinum toxin-A (BTX-A) injection. After another frontotemporal filling with BTX-A injection (C, F), significant improvement was observed.
DISCUSSION
Autologous fat transplantation has been widely employed in frontal contour reconstruction for a fuller and smoother forehead due to its minimal invasion, availability, and natural plastic effect. However, its unpredictable retention rate limits its long-term effects. Several solutions have been proposed to solve this problem, such as the application of stromal vascular fraction gel with a higher retention rate in facial rejuvenation. But this is not ideal for forehead filling, where it is hypothesized that the retention difficulty is related to the movement of corrugator muscles.
Studies have reported that fat graft combined with BTX-A injection in mice could improve long-term retention rate, because the muscular movements are inhibited in the recipient area.19–21 BTX-A reduced muscle-derived dynamic or compressive mechanical forces and might promote adipogenesis in the graft. Previous studies have confirmed the validity of fat graft combined with BTX-A injection in mice, but it has not been established in humans. Therefore, this study aimed to investigate the effect of inhibiting the corrugator muscles with BTX-A on the retention rate of stromal vascular fraction gel in prefrontal filling.
The treating surgeon was asked whether or not the patient received BTX-A injection and what the reasons were for that; the physician summarized this information for us. In the injected group, patients accepted BTX-A injection because of the surgeon’s recommendation and previous positive experiences. In the noninjected group, patients refused BTX-A injection. The reasons included (1) uncertainty about the effect of BTX-A; (2) a history of intolerance or significant adverse effects with BTX-A; and (3) avoiding the additional expenses.
Four criteria, including patient satisfaction, GAIS score, retention rate, and curvature, were evaluated by taking measurements and analysis of photographs and 3D scans taken before and 6 months after treatment. According to the questionnaire, most patients in the injected group reported satisfaction with filling combined with BTX-A on the 3 questionnaire items, suggesting that administration of BTX-A improved the appearance of the forehead. Most patients in the noninjected group did not think that the frontal area had a significant improvement. One patient in the injected group said she would not recommend the same treatment to others due to its high expense. Four patients in the noninjected group declared that they would not recommend the treatment because they thought it was ineffective. During the follow-up period, most patients in the noninjected group believed that the filling effects in both temporal and lateral parts were very satisfactory, but that the prefrontal region effects were not remarkable. The center of the forehead was relatively flat, and its transition was not smooth. In analyzing the cause, these patients were asked if the flatness was associated with frequent frowning; they agreed that it was. Feedback in the injected group was different, because patients could not frown.
The stromal vascular fraction gel, which is routinely filled into the connective tissue under the frontalis muscle, is often squeezed by the corrugator muscles at the lower part of the forehead and between the eyebrows. The corrugator muscles include the corrugator supercilii, depressor supercilia, and procerus, and are located on the deep orbital surface of the frontal and orbicularis oculi muscles. The satisfaction questionnaire indicated that the movement of the corrugator muscles had a significant impact on the retention rate of stromal vascular fraction gel filling in the center of the forehead, and that when the muscles were paralyzed the filling effect improved significantly.
Professional plastic surgeons not involved in the process compared the pretreatment and posttreatment photographs and assigned GAIS scores. The median score of the injected group was 2 points, and that of the noninjected group was 1.5 points, indicating that the appearance of the injected group was significantly improved, whereas that of the noninjected group was improved but could achieve better results. This suggested that BTX-A injection was beneficial to the filling effect.
According to the 3D images, the average retention rate was 70.89% for the injected and 56.74% for the noninjected, indicating a significant increase in retention rate after the BTX-A injection. The results were consistent with our expectations and the results of animal experiments.19–21
The mean of the maximum curvature difference was 0.2445 and 0.1294 for the injected and noninjected groups, respectively, indicating that the protrusion degree of the lower part of the forehead in the injected group was more obvious, and the forehead was fuller and smoother. Traditionally, BTX-A makes the forehead look smoother by reducing frontal wrinkles, but in this study the mechanisms of BTX-A restricted muscle movement to increase the retention rate of the graft, resulting in a more rounded and smooth forehead.22 Wu and colleagues also suggested that graft volume with poor long-term retention due to the movements of the muscles inhibited the sprouting of new blood vessels, thereby limiting graft vascularization.23 Our study verified that the injection of BTX-A in the prefrontal corrugator muscles would improve the retention rate of stromal vascular fraction gel at this site and form a fuller frontal arc. Limiting muscle movement may well have reduced compression on the graft and allowed for improved growth of new blood vessels on the graft. This may have provided the graft with a more stable and adequate environment, increasing its retention and aesthetic effect.
However, there were some limitations to this study. First, only patients who underwent facial filling in our hospital in the past 2-1/2 years were included. The sample size of each group was relatively small. Further expansion of the sample size and geographical selection of the population should be considered for further studies. Second, of the 167 patients, only 79 had complete follow-up data and were successfully enrolled, which inevitably showed follow-up bias. However, the proportion of lost to follow-up patients in the 2 groups was similar, so there was no significant impact on the results of this study. Finally, this was only a retrospective analysis, conducted by classifying the existing data; the study failed to randomize the patients for prospective analysis. Nevertheless, the findings reflected that stromal vascular fraction gel transplantation supplemented by BTX-A injection improved the retention rate and cosmetic effect.
In recent years, BTX-A injection has become an important minimally invasive treatment of facial rejuvenation.24 This study focused on the combination of BTX-A with forehead filling, providing a minimally invasive combination therapy with better efficacy than simple forehead filling. In addition, a study has shown that the traditional brow-lifting technique combined with BTX-A injection skillfully reduced the effect of muscle traction, fundamentally treated the dynamic crow's feet on the external canthus caused by the contraction of the orbicularis oculi muscle, improved the postoperative effect, and resulted in high patient satisfaction.25 Another study involved performance of lower blepharoplasty combined with BTX-A. It was found that the therapeutic effect was better than simple lower blepharoplasty.26 In addition to periocular rejuvenation, BTX-A can also be utilized to improve bunny lines, vertical perioral rhytides, the melomental fold, and platysmal banding.27 In the future, we will continue to explore the improvement effect of combining BTX-A with more traditional procedures.
CONCLUSIONS
BTX-A injection limited the movement of the corrugator muscles. As a result, the retention rate of stromal vascular fraction gel was improved significantly, and the forehead was fuller and smoother. The study suggests that the combined application of stromal vascular fraction gel and BTX-A injection for frown inhibition leads to more effective frontal filling.
ACKNOWLEDGMENTS
Drs. Wang and Cheng contributed equally to this work as co-first authors.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
This study was supported by the National Natural Science Foundation of China (No. 82102356), the Outstanding Young Medical Talents Training Funding Project of The First Affiliated Hospital of Harbin Medical University (No. 2021J05), the Applied Technology Research and Development Project of Heilongjiang Province (No. GA20C019), and the Postgraduate Research and Practice Innovation Program of Harbin Medical University (YJSCX202088HYD).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}