






Abstract
A wealth of evidence suggests that adolescent psychotic experiences (PEs), and especially auditory hallucinations (AHs), are associated with an increased risk for self-injurious behavior (SIB). However, the directionality and specificity of this association are not well understood, and there are no published studies investigating within-person effects over time. The present study aimed to test whether AHs and SIB prospectively increase reciprocal risk at the individual level during early-to-middle adolescence.
Three waves (12y, 14y, and 16y) of self-reported AHs and SIB data from a large Tokyo-based adolescent birth cohort (N = 2825) were used. Random Intercept Cross-Lagged Panel Model (RI-CLPM) analysis was conducted to test the within-person prospective associations between AHs and SIB.
At the within-person level, AHs were associated with subsequent SIB over the observation period (12y–14y: β = .118, P < .001; 14–16y: β = .086, P = .012). The reverse SIB->AHs relationship was non-significant at 12–14y (β = .047, P = .112) but emerged from 14y to 16y as the primary direction of influence (β = .243, P < .001). Incorporating depression as a time-varying covariate did not meaningfully alter model estimates.
A complex bi-directional pattern of relationships was observed between AHs and SIB over the measurement period, and these relationships were independent of depressive symptoms. Adolescent AHs may be both a predictor of later SIB and also a manifestation of SIB-induced psychological distress.
Introduction
Adolescent psychotic experiences (PEs) are widely reported and associated with a broad range of poor mental health outcomes.1–5 PEs have been associated with self-injurious behavior (SIB) with and without suicidal intent in many large adolescents population-based studies6–8; one recent meta-analysis found that PEs confer 3.2× increased odds of any SIB9 with another finding that PEs confer 2× increased odds of suicidal ideation and 3× odds of suicide attempt specifically.10 PEs occurring at older ages in adolescence, as well as PEs that are persistent over time, tend to be less prevalent but more clinically relevant as indicators of concurrent distress and subsequent psychological ill-health.11,12 Within the psychotic experience spectrum, auditory hallucinations (AHs) are an especially potent risk factor for SIB and suicidality13,14; these associations have been identified even where other PE subtypes demonstrated no such association.15 Moreover, AH items have been shown to demonstrate the greatest validity among adolescent PE screeners.16,17
It is unknown to what degree the PEs–SIB relationship is causal. Two recent systematic reviews have found PEs–SIB associations to be frequently robust to the inclusion of confounders such as comorbid mental illness, environmental stressors, substance use, and early-life traumatic experiences9,13; similar observations were made in a meta-analysis of PEs and suicidal outcomes.10 Even where adjustment is found to lead to non-significance (eg, psychological distress,7,15 and cumulative psychosocial risk17), it is often unclear whether this represents confounding, or clinically relevant mediation effects facilitating the causal pathway between PEs and SIB.13 Furthermore, the direction of the longitudinal relationship between PEs and SIB has received comparatively little attention. The literature has almost exclusively focused on the degree to which PEs increase the risk for subsequent SIB (ie, PEs cause SIB, but not vice-versa) or to which both are consequences of shared risk factors (ie, PEs do not cause SIB, and SIB does not cause PEs; “third variables” are responsible for the association).9,13
In a recent study using cross-lagged panel modeling (CLPM), Murphy and colleagues found preliminary evidence that the relationship between PEs and SIB was bi-directional (ie, PEs cause SIB and SIB causes PEs) for both any PE and AHs alone at 12y and 18y in a birth cohort of general population adolescents (n = 2232), even after extensive controlling for known shared risk factors.18 Dubbed the “suicidal drive hypothesis”, Murphy and colleagues propose that some subtypes of PEs are manifestations of (and therefore caused by) the psychologically intolerable self-directed threat posed by self-harm episodes.19 However, one major limitation of CLPM is the limited ability to test such within-person causal inferences, as CLPM conflates between-person and within-person variance.20–23 Using the example of psychosis and cannabis use, van Os and colleagues suggest this may be a significant and widespread limitation across psychosis research; within-person causal inferences are frequently made about psychotic phenomena without using analyses that are able to sufficiently control for the full range of between-person confounders, leading to potentially spurious causal assessments.24 The PE–SH relationship is a prime example, as it is within-person relationships that are the main object of interest—i.e. how experiencing PEs influences the prospective likelihood of that same individual self-harming, and vice-versa—yet there are no studies to date which have conducted within-person analyses between these variables.
With a large, representative birth cohort sample (Tokyo Teen Cohort; TTC) and three waves of data available at 12y, 14y, and 16y, we sought to use Random Intercept Cross-Lagged Panel Model (RI-CLPM) analysis to investigate the direction and strength of longitudinal associations between AHs and SIB in adolescence at the within-person level. The RI-CLPM extends the standard CLPM via the addition of stable “random intercepts” for each measured variable, thus partialing out between-person variance so that the cross-lagged associations represent only within-person change over time.20 Our hypotheses were (a) that AHs would be prospectively associated with increased SIB risk at the within-person level, based on numerous prior studies13; and (b) that SIB would exhibit prospective associations with AHs at the within-person level, as suggested by Murphy & colleagues’ previous CLPM analyses.17
Methods
Study Design and Participants
Data was used from the Tokyo Teen Cohort (TTC) study (http://ttcp.umin.jp/). TTC is an ongoing population-based birth cohort study assessing health and development in a representative sample of adolescents in Tokyo. Baseline recruitment was carried out via random sampling of households with a child born between September 2002 and August 2004 using the resident registers of three Tokyo municipalities (Setagaya-ku, Mitaka-shi, and Chofu-shi) with oversampling of low-income households used to compensate for predicted low response rate. With data collection commencing in 2012, a trained interviewer visited participant homes to administer self-report questionnaires when the child was 10 (T1), 12 (T2), 14 (T3), and 16 (T4) years of age. Measures pertaining to sensitive items were administered in the presence of the interviewer to ensure confidentiality from caregivers. A total of 3171 child–parent pairs were recruited to the T1 cohort; of these, 3007 participated at T2 (follow-up rate: 94.8%), 2667 at T3 (follow-up rate: 84.1%), and 2616 at T4 (follow-up rate: 82.5%). The full protocol for TTC has been published previously.25 As SIB data was not collected at T1, data from T2 to T4 was used for the main RI-CLPM analysis. T1 data was used only to check for attrition biases.
Written informed consent was obtained from primary caregivers prior to participation in each wave of data collection. Written informed assent was obtained from adolescent participants at T2 (12y) and T3 (14y); written informed consent was obtained at T4 (16y). The TTC study protocol was approved by the Ethics Committees of the Tokyo Metropolitan Institute of Medical Science (approval number: 12-35), the University of Tokyo (10057), and SOKENDAI (the Graduate University for Advanced Studies; 2012002).
Measures
Auditory Hallucinations.
A single self-report item measuring auditory hallucinations taken from the Diagnostic Interval Schedule for Children (DISC-C) was used.26 Respondents were asked “Have you ever heard a voice that other people couldn’t hear?” and answered with “yes, definitely”, “maybe”, or “no, never”. Adolescents who answered “yes, definitely” were treated as having auditory hallucinations; “no, never” and “maybe” responses were treated as indicating the absence of hallucinations. Prior research has indicated that this item has excellent predictive power for adolescents experiencing auditory hallucinations (positive predictive value: 71.4%; negative predictive value: 90.4%) and identifying those experiencing any psychotic symptom (PPV: 100%; NPV: 88.4%), validated against interviewer-ratings16; it may also be less susceptible to social desirability biases than other PE items.17 As such, items assessing auditory hallucinations are often used as a general indicator of adolescent PEs.11,17,27,28 The Japanese versions of these measures have been used in a number of previous studies.6,29–32
Self-Injurious Behavior.
A 12m prevalence of self-injurious behavior was captured via a single self-report item: “Within the past year, have you ever hurt yourself on purpose?”. Possible responses were “no” and “yes” at T2 (12y). However, at T3 (14y) and T4 (16y), possible responses were “never”, “only once”, “2–5 times”, “6–10 times” and “More than 10 times”; for comparability with T2 data, these responses were recoded as a binary variable (never=“no”; once or more=“yes”). This metric is similar to those used in previous studies of adolescent self-harm.33–35
Confounding Variables.
The within-unit analysis in a RI-CLPM model is controlled for time-stable confounders, such as sociodemographic factors, environmental influences, and early-life experiences. As such, only time-varying confounders were considered for inclusion as control variables. Depression has been found to mediate the prospective association of PEs with later SIB in two prior meta-analyses.9,13 The present study used the Short Mood and Feelings Questionnaire (SMFQ); a unidimensional 13-item measure capturing depressive symptoms in children and adolescents aged 8–18 years.36 A dichotomous variable derived from a cut-off of ≥8 was used to indicate a high risk of depression, as this cut-off has demonstrated good internal consistency (α = 0.85) and predictive validity against diagnosis (60% sensitivity and 85% specificity).36 The Japanese version of the SMFQ has been used in multiple prior studies of adolescents in Japan.37–39
Since the statistical treatment of variables of interest and time-varying confounders is identical in RI-CLPM, adding multiple confounders can quickly make the models extremely large, and so difficult to interpret. As such, we opted to include depression as the sole time-varying confounder, and present both bivariate (unadjusted) and trivariate (adjusted) models in the results.
Analysis
Random Intercept Cross-Lagged Panel Modeling (RI-CLPM)20 was conducted to test the within-person associations between AHs and SIB at 12y, 14y, and 16y. The fully specified RI-CLPM path diagram is shown in figure 1. For each construct of interest, the observed variables at 12y, 14y, and 16y were regressed (with regression weights constrained to be equal) on (a) a single time-invariant latent factor representing stable influences on the construct over the observation period (the “random intercept”) and (b) a separate latent factor for each time point, representing time-specific deviations in an individual’s construct level at the time of measurement. Cross-lagged and auto-regressive parameters were then specified and freely estimated between these time-varying latent factors, with the coefficients of these parameters interpreted as associations between within-person change in AHs/SIB over that time interval. These within-person associations were used to test our hypotheses that AHs and SIB would be prospectively associated over time. The correlations of the random intercepts were interpreted as capturing the time-invariant effects of unmeasured between-person sources of variance (eg, gender, childhood adversity, and stable environmental factors) on the overall relationships between constructs. We conducted a bivariate analysis with AHs and SIB only (figure 2) and an additional trivariate model adjusting for depression as a time-varying confounder (figure 3).
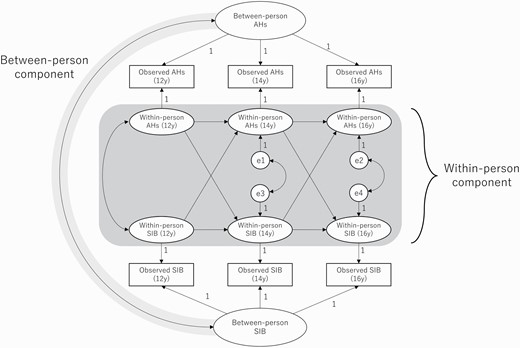
Full specification of bivariate RI-CLPM analyzing reciprocal effects of auditory hallucinations (AHs) and self-injurious behavior (SIB) at 12y, 14y, and 16y.
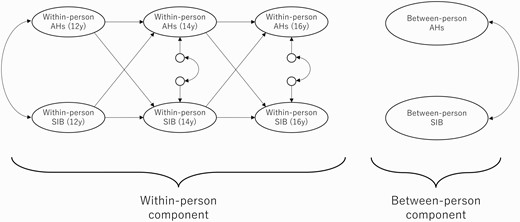
Simplified representation of bivariate RI-CLPM analyzing reciprocal effects of auditory hallucinations (AHs) and self-injurious behavior (SIB) at 12y, 14y, and 16y.
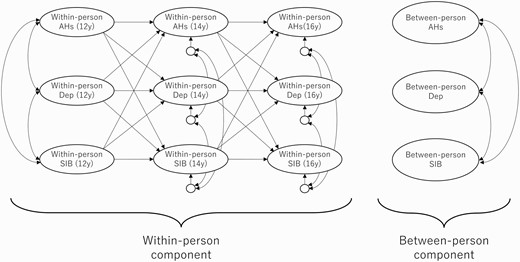
Simplified representation of trivariate RI-CLPM analyzing reciprocal effects of auditory hallucinations (AHs) and self-injurious behavior (SIB) at 12y, 14y, and 16y with the inclusion of depression (Dep) as a time-varying covariate.
Standardized estimates were reported and compared for all analyses. Significance thresholds were set to .05. We adopted a full information maximum likelihood (FIML) estimation procedure to handle missing data under the assumption of missing at random (MAR). RI-CLPM analyses were performed using IBM SPSS Statistics v.28.0 (IBM Corp., Armonk, NY, USA), and IBM SPSS Amos v.28.0 (IBM Corp.); Amos files containing path diagrams and syntax can be found as a supplementary material to this paper. Additional sensitivity analyses were conducted using Mplus v.8.7 (bootstrap) and R v.4.1.3 (multiple imputations) using the “mice”, “lavaan”, and “semTools” packages.
Results
Participant responses for this sample are detailed in Table 1. From the full (N = 3171) cohort, cases with completely missing data for all relevant variables were removed, resulting in a sample of N = 2825. Chi-square tests yielded no significant differences in gender, age in months (higher/lower than the median), or low-income status (annual household income <\4 900 000) resulting from the removal of these 346 cases. Further chi-square tests revealed no significant differences in gender or age between participants retained vs. lost to attrition at any subsequent wave. However, there was evidence that low-income participants were more likely to drop out over time (T2 low SES on T3 non-response: χ² = 3.774, P = .052; T3 low SES on T4 non-response: χ² = 5.736, P = .017).
Sample Characteristics
| N = 2825 (girls: N = 1327, 47.0%) | Age 12 | Age 14 | Age 16 |
|---|---|---|---|
| Mean age, months1 (SD) | 146 (3.6) | 172 (3.4) | 198 (4.5) |
| Low household income2 (<\490 000), n (%) | 285 (16.5) | 192 (12.8) | 192 (13.6) |
| Auditory hallucinations,3n (%) | 223 (8.9) | 121 (5.9) | 59 (3.0) |
| Self-injurious behaviour,4n (%) | 278 (11.2) | 119 (5.8) | 110 (5.7) |
| Depressive symptoms,5n (%) | 444 (17.9) | 279 (13.5) | 351 (17.4) |
| N = 2825 (girls: N = 1327, 47.0%) | Age 12 | Age 14 | Age 16 |
|---|---|---|---|
| Mean age, months1 (SD) | 146 (3.6) | 172 (3.4) | 198 (4.5) |
| Low household income2 (<\490 000), n (%) | 285 (16.5) | 192 (12.8) | 192 (13.6) |
| Auditory hallucinations,3n (%) | 223 (8.9) | 121 (5.9) | 59 (3.0) |
| Self-injurious behaviour,4n (%) | 278 (11.2) | 119 (5.8) | 110 (5.7) |
| Depressive symptoms,5n (%) | 444 (17.9) | 279 (13.5) | 351 (17.4) |
Note:1Valid N = 2774 at 12y; 2478 at 14y; 2387 at 16y.
2Assessed byparent-report. Valid N = 1730 at 12y; 1498 at 14y; 1407 at 16y.
3Assessed by self-report item from the Diagnostic Interview Schedule for Children (DISC-C), counting “definite” responses only. Valid N = 2503 at 12y; 2056 at 14y; 1938 at 16y.
4Assessed by self-report item pertaining to the past year. Valid N = 2480 at 12y; 2048 at 14y; 1939 at 16y.
5Assessed by SMFQ, using ≥8 as cut-off indicating high risk of depression. Valid N = 2479 at 12y; 2070 at 14y; 2017 at 16y.
Sample Characteristics
| N = 2825 (girls: N = 1327, 47.0%) | Age 12 | Age 14 | Age 16 |
|---|---|---|---|
| Mean age, months1 (SD) | 146 (3.6) | 172 (3.4) | 198 (4.5) |
| Low household income2 (<\490 000), n (%) | 285 (16.5) | 192 (12.8) | 192 (13.6) |
| Auditory hallucinations,3n (%) | 223 (8.9) | 121 (5.9) | 59 (3.0) |
| Self-injurious behaviour,4n (%) | 278 (11.2) | 119 (5.8) | 110 (5.7) |
| Depressive symptoms,5n (%) | 444 (17.9) | 279 (13.5) | 351 (17.4) |
| N = 2825 (girls: N = 1327, 47.0%) | Age 12 | Age 14 | Age 16 |
|---|---|---|---|
| Mean age, months1 (SD) | 146 (3.6) | 172 (3.4) | 198 (4.5) |
| Low household income2 (<\490 000), n (%) | 285 (16.5) | 192 (12.8) | 192 (13.6) |
| Auditory hallucinations,3n (%) | 223 (8.9) | 121 (5.9) | 59 (3.0) |
| Self-injurious behaviour,4n (%) | 278 (11.2) | 119 (5.8) | 110 (5.7) |
| Depressive symptoms,5n (%) | 444 (17.9) | 279 (13.5) | 351 (17.4) |
Note:1Valid N = 2774 at 12y; 2478 at 14y; 2387 at 16y.
2Assessed byparent-report. Valid N = 1730 at 12y; 1498 at 14y; 1407 at 16y.
3Assessed by self-report item from the Diagnostic Interview Schedule for Children (DISC-C), counting “definite” responses only. Valid N = 2503 at 12y; 2056 at 14y; 1938 at 16y.
4Assessed by self-report item pertaining to the past year. Valid N = 2480 at 12y; 2048 at 14y; 1939 at 16y.
5Assessed by SMFQ, using ≥8 as cut-off indicating high risk of depression. Valid N = 2479 at 12y; 2070 at 14y; 2017 at 16y.
The prevalence of rates of AHs across the three-time points was within the range of results reported by other general population adolescent cohort studies in Japan32 and internationally,40,41 and similarly declined with age12,32,40; SIB rates were also comparable to global estimates.33 Systematic missingness of AH data at each wave was investigated by chi-square tests comparing to the presence/absence of AHs at 10y; results were non-significant for all waves. Similar tests could not be conducted for SIB (as not collected at 10y), though comparison to T1 SMFQ gave no evidence that SIB missingness at any wave was related to 10y depression status.
Bivariate and trivariate RI-CLPM analyses were conducted to test cross-lagged associations at the within-person level between AHs and SIB at all three-time points. Parameter estimates are reported for both, though as estimates were similar between models, only the bivariate model diagram is presented below (figure 4); the trivariate model (supplementary figure 5) can be found in the supplementary material. At the within-person level, individuals who experienced AHs at 12y exhibited increased likelihood of reporting SIB at 14y (bivariate model, β = .118, P < .001; trivariate model, β = .124, P < .001) while SIB at 12y did not demonstrate any significant within-person prospective associations with AHs at 14y (bivariate model, β = .047, P = .112; trivariate model, β = .038, P = .203). However, individuals reporting SIB at 14y did exhibit increased likelihood of reporting AHs at 16y (bivariate model, β = .243, P < .001; trivariate model, β = .241, P < .001), while the effect of AHs on SIB likelihood at 14–16y (bivariate model, β = .086, P = .012; trivariate model, β = .079, P = .021) was reduced compared to the effect between 12y and 14y. As sensitivity analyses, trivariate model analyses were re-run using continuous SMFQ scores; cross-lagged effects between SIB and AHs did not differ from reported estimates using cut-off (dichotomous) scoring. In addition, we carried out re-estimation via bootstrap analysis (10 000 repetitions) and using multiple imputations (100 datasets) on our bivariate model. The overall pattern of results was consistent with the RI-CLPM presented here, with the exception that the association between AHs at 14y and SIB at 16y was reduced to trend level (bootstrap analysis: P = .076; multiple imputations: P = .084).
![Bivariate RI-CLPM analyzing relationships between auditory hallucinations (AHs) and self-injurious behavior (SIB) at 12y, 14y, and 16y, separated into within-person and between-person components. Solid black arrows represent significant regression weights (single-headed) or correlations (double-headed); significant cross-lagged effects are highlighted in bold. Standardized estimates are reported. Dashed/gray arrows denote non-significant parameters (P > .05). Model χ²/df(1): 1.264 (P = 0.261), CFI: 1.000, RMSEA: 0.009 [90% CI: 0.000–0.049]. *P < .05 ***P < .001.](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/schizophreniabulletin/49/2/10.1093_schbul_sbac155/1/m_sbac155f0004.jpeg?Expires=1749224599&Signature=VEX4gjHvzeXaRdlCpnhEQ2FosAmtDO3AFNyUErDvytfRDL50hV-dZsm0vF0dTrQJR-GI~2~~SfZSNNV93VG49-NbWqYsgypxT69dzZeYX3TNvsYHb-4f9WQjA74QKDkEwEP8Y1rDDbjwy6yTXZIXmMji21aDoOzOpVHKuhqITxna3e176Fc0xHiKc8gB0qnp~fA28DSXcu2XYPhwURCvkkr29Q86yztzByKYW9WQMBa5wkr8VtWJud2bAJlBhag5PxT91Ii3qzyFWtotokTbna3nRzz7xVpT-VHWrPGAEcVo2Uc-ECjT6-8iKLjbZ2--FQEM5CD7K3tgGu84APDxAw__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Bivariate RI-CLPM analyzing relationships between auditory hallucinations (AHs) and self-injurious behavior (SIB) at 12y, 14y, and 16y, separated into within-person and between-person components. Solid black arrows represent significant regression weights (single-headed) or correlations (double-headed); significant cross-lagged effects are highlighted in bold. Standardized estimates are reported. Dashed/gray arrows denote non-significant parameters (P > .05). Model χ²/df(1): 1.264 (P = 0.261), CFI: 1.000, RMSEA: 0.009 [90% CI: 0.000–0.049]. *P < .05 ***P < .001.
Auto-regressive effects for AHs were significant at both 12y–14y (bivariate model, β = .212, P < .001; trivariate model, β = .209, P < .001) and 14–16y (bivariate model, β = .220, P < .001; trivariate model, β = .219, P < .001), meaning AHs were prospectively associated with themselves at all time points. In contrast, SIB at 12y was not associated with SIB at 14y (bivariate model, β = −.017, P = .674; trivariate model, β = −.004, P = .922), though SIB at 14y did predict SIB at 16y (bivariate model, β = .221, P < .001; trivariate model, β = .215, P < .001). At the between-person level, the random intercepts of AHs and SIB were not significantly correlated in either model (bivariate model, r = .111, P = .675; trivariate model, r = .088, P = .748).
Model fit indices were as follows: bivariate = model χ²/df(1) = 1.264 (P = 0.261), CFI: 1.000, RMSEA: 0.009 [90% CI: 0.000–0.049]; trivariate = model χ²/df(3) = 1.926 (P = 0.123), CFI: 0.998, RMSEA: 0.017 [90% CI: 0.000–0.038], suggesting excellent fit for both models compared to conventional thresholds of model χ²/df < 2, CFI > 0.95 and RMSEA < 0.08.42,43 While we include the RMSEA here, it should be noted that this may be an overly strict estimate of model fit where models have low degrees of freedom.44 As both our models had low df (bivariate model df = 1, trivariate model df = 3), model χ²/df and CFI were used as primary indicators for assessing model fit.
Discussion
Overall, our within-person analyses were supportive of a bi-directional relationship between AHs and SH in adolescence, though the pattern of these relationships changed over time. Our models suggested that experiencing AHs increased the risk of that same individual later experiencing SIB at both 12–14y and 14–16y, though this effect was attenuated at the later interval. Meanwhile, SIB demonstrated no significant effect on an individual’s risk of AHs from 12y to 14y but did increase risk for later AHs from 14y to 16y. As a result, the primary direction of influence was from AHs->SIB at 12y–14y but reversed between 14y and 16y, where SIB->AHs emerged as the stronger effect. Regression weights varied only trivially after model adjustment suggesting these relationships were largely independent of depressive symptoms, which prior research has suggested mediates the relationship between psychotic experiences and SIB.13 The use of RI-CLPM models also allows us to exclude “third variable” explanations based on known between-subjects confounders (eg, sociodemographic13 and environmental influences,45 early-life trauma46).
This pattern of results may relate to the changing nature of psychotic experiences across adolescent development. Previous longitudinal studies have noted that the prevalence of AHs and other psychotic experiences tends to decline from childhood through adolescence, as likewise found in these data, while the clinical and functional severity of these symptoms simultaneously increases.11,40,47 The smaller effect sizes of the AHs->SIB relationships may suggest that AH is not driving subsequent SIB through any direct mechanism but, instead, serves as an early marker of psychological difficulty that precedes the typical age of onset of SIB. AHs may signify loneliness48,49 and/or social isolation,50 helplessness51 and emotional regulation difficulties,15,27 which are instrumental factors in the Interpersonal52,53 and the Integrated Motivational-Volitional54,55 theories of suicide as well as the Cognitive-Emotional model of NSSI.56 In contrast, the larger effect size of the SIB->AHs relationship observed from age 14 to 16 may indicate a more direct and/or specific relationship, where the emotional distress associated with self-harm, as well as the stigma and social isolation that may accompany these behaviors, can contribute to substantial psychological distress that manifests as AHs in vulnerable individuals. Under this framework, acts of SIB at age 14 may act as a source of stress or trauma that can contribute to psychosis onset or persistence, consistent with diathesis-stress,57,58 social defeat,59,60 and other models of psychosis etiology emphasizing prolonged exposure to adversity.45,61
Our results are consistent with Murphy and colleagues’ recent analyses, which observed a bi-directional relationship between any PE and SIB at 12y and 18y.18 In addition, that our results showed shifting relative strength of the SIB->AHs relationship compared to AHs->SIB from 12y to 14y and 14y to 16y may (partially) explain why neither AHs nor SIB was the dominant predictor of the other over their six-year measurement interval. One notable difference is that we found the SIB->AHs relationship to be significant from 14y to 16y only, while Murphy and colleagues’ analysis found that SH at 12y conferred 2.5× increased odds of hallucinations (including both auditory and verbal) at 18y. Prior evidence has not been conclusively supportive of a SIB->PEs longitudinal relationship in adolescence; one recent cohort study by Hielscher and colleagues with Australian adolescents aged 12–17 found any PE was prospectively associated with non-suicidal self-injury (NSSI), but not the reverse, at 1 and 2-year follow-ups.12 The results for AHs alone were mixed, with NSSI conferring significantly increased odds (OR=4.75) of AHs at 1-year follow-up, but not at 2-year. There is therefore accumulating evidence for self-injurious behavior prospectively increasing risk for AHs in adolescence, though this may not apply to other PE subtypes and age may be a more significant factor than for the reverse direction.
Our study has numerous strengths. We believe the present analysis to be the first application of RI-CLPM to model the longitudinal relationship between adolescent psychotic experiences and SIB, and thus the first to analyze specifically within-person effects in this area. This represents a substantial contribution to the literature, where the debate about time-invariant confounders—eg, genetic factors, adverse childhood experiences—has previously cast doubt on whether previously observed PEs-SIB correlations are explainable by unmeasured (or unmeasurable) third factors24 Although not yet widespread in use, it has been argued elsewhere that RI-CLPM (and other within-person analysis techniques) may address critical methodological shortcomings in psychiatric epidemiology more broadly, particularly around issues of causal inference20–24 (though see Lüdtke and Robitzsch62 for a critical review). An additional strength is the use of Tokyo Teen Cohort study data. TTC is a large, population-based prospective adolescent birth cohort drawn from three wards of the Tokyo metropolitan area, with oversampling of lower SES households.25 As TTC is a birth cohort with data collection every 2 years, we were able to model relationships at specific ages in early- and mid-adolescence. An additional unique strength of TTC is that self-reported drug use was n = 0 at 14y and n < 5 at 16y (not collected at 10y and 12y), suggesting this is highly unlikely to be confounding any observed associations.
There are limitations to the present study. First, although our study controlled for depression, other time-variant factors (such as psychological distress) were not controlled for. Moreover, while we assumed that the between-person variance component controlled for exposures before measurements such as childhood adversity and environmental risk, it is theoretically possible that these confer time-varying effects (ie, do not confer increased risk until mid- or late-adolescence, or confer mediation/moderation effects between AHs and SIB following initial onset) that would not have been controlled for by this component of our model. These limitations preclude us from claiming that AHs and SIB are directly causing each other—though this does not reduce the importance of the more clinically relevant observation that SIB and AHs increase the risk for each other at the individual level in mid-adolescence, rather than being explainable by between-person confounding. Second, our analyses only allowed observation of the relationship between AHs and SIB in early- and mid-adolescence, from 12y to 16y. Future studies analyzing datasets from later adolescence, including forthcoming waves of the TTC data, would be valuable for investigating whether this bi-directionality is consistent in the transition to adulthood. Finally, our measures of AHs and SIB were self-report, single-item metrics. While our prevalence estimates for AHs and SIB were consistent with previous studies,32,33,40,41 incorporating triangulated data from multiple sources—eg, researcher or clinician-conducted interviews—may result in more comprehensive measurement.1,63 Using single-item metrics meant we were unable to analyze the potential differential effects of severity, persistence, or subjective content of these experiences. AHs may have varying clinical implications depending on the verbal content (eg, name-calling, praise, criticism, and commands), the hearer’s beliefs about the source (eg, spiritual, malevolent, real, or illusory), the degree to which the voices can be controlled, and whether or not the experiences are distressing.64–68 In addition, meta-analytic findings suggest methods, motivation, and frequency of SIB mediate the risk of subsequent outcomes such as the transition to the suicide attempt.35 Nonetheless, as brevity is often a vital factor for inclusion in clinical contexts, it is a notable practical implication of the present study that later individual-level risk can be predicted from single-item screeners.
Overall, our study has demonstrated evidence of a bi-directional relationship between AHs and SIB at the within-person level in a general population cohort of adolescents. Further, we have demonstrated that the relative strengths of these relationships may not be consistent over adolescence, with AHs predicting SIB over the full observation period but attenuating from 14y to 16y, and SIB overtaking AHs as the dominant predictor from 14y onwards. Future studies investigating AHs and SIB (and subtypes thereof) from early through to late adolescence and early adulthood would represent valuable next steps in understanding these complex relationships.
Funding
This work was supported by JSPS KAKENHI (grant numbers JP19K17055, JP20H01777, JP20H03951, JP20H03596, JP21H05171, JP21H05173, JP21H05174); JST-Mirai Program (grant number JPMJMI21J3), Japan; and the International Research Center for Neurointelligence (WPI-IRCN) at The University of Tokyo Institutes for Advanced Study (UTIAS).
Acknowledgments
We sincerely thank all of the adolescents and their primary caregivers who participated in TTC. We acknowledge the work of all interviewers who conducted the data collection. The authors have declared that there are no conflicts of interest in relation to the subject of this study.
Data Availability
Data can be made available from the Tokyo Teen Cohort Data Operating Committee for all interested researchers upon requests sent to the committee. The initial contact for the request should be addressed to Dr. Atsushi Nishida [[email protected]].

{kind=link}
{kind=link}
{kind=link}
{kind=link}