





IgG4-related disease (IgG4RD) should be considered as a potential cause of pericarditis. Early diagnosis and treatment of IgG4-related pericarditis can prevent pericardial fibrosis and subsequent heart failure. A multidisciplinary team approach, including comprehensive imaging studies and histopathologic confirmation, is required for proper management of IgG4RD.
Introduction
IgG4-related disease (IgG4RD) is an uncommon systemic inflammatory disorder. Although cardiac involvement in IgG4RD is rare with an unknown prevalence, more cases are being reported with increasing awareness. We present a case of IgG4RD affecting solely the pericardium and manifesting as effusive constrictive pericarditis (ECP).
Case presentation
A 77-year-old man presented to the emergency department due to poor oral intake and fever of 3 months’ duration. He had a 20-year history of hypertension and dyslipidemia. His blood pressure was 132/82 mmHg, heart rate was 112 beats/min, respiratory rate was 20/min, and body temperature was 36.2°C. Physical examination showed weak, fast and regular heartbeats without murmur, and no palpable mass or enlarged lymph nodes. An electrocardiogram revealed sinus tachycardia at 112 bpm. A chest radiograph showed cardiomegaly with a cardiothoracic ratio of 0.59 and a blunted left costophrenic angle. Laboratory findings were unremarkable except for anemia with a hemoglobin of 9.3 g/dl, and elevated levels of high-sensitivity C-reactive protein of 33.91 mg/l and N-terminal pro-brain natriuretic peptide of 557.9 pg/ml. Computed tomography scans of the chest and abdomen revealed a pericardial effusion with pericardial thickening and both pleural effusions (Figure 1A). There was no evidence of lymphadenopathy or masses. Transthoracic echocardiography indicated a normal left ventricular ejection fraction of 58% and the findings of ECP with a moderate amount of pericardial effusion and fibrinous strands (Figure 1A).18F-fluorodeoxyglucose-positron emission tomography scan showed diffusely increased uptake in the pericardium (Figure 1B).
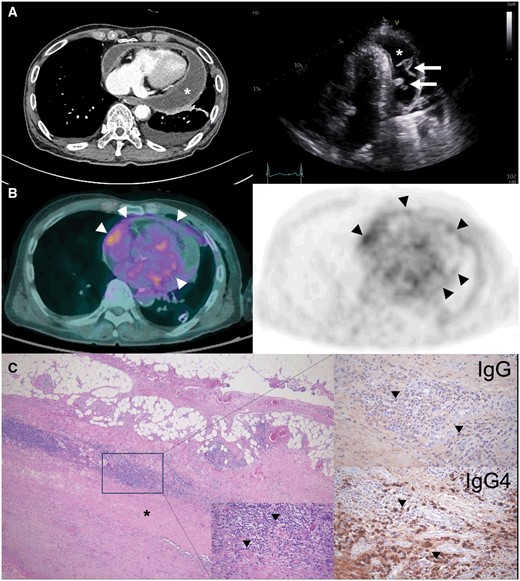
(A) Chest computed tomography and echocardiography showing a moderate amount of pericardial effusion (white asterisks) with pericardial thickening and fibrinous strands (arrows). (B) 18F-fluorodeoxyglucose-positron emission tomography scan showing diffusely increased uptake (arrowheads) in the pericardium. (C) The pericardial biopsy specimen demonstrating dense fibrosis of the pericardium (black asterisks) and infiltration of lymphoplasmacytic cells (arrowheads) (middle bottom, hematoxylin & eosin) stained brown by IgG and IgG4 with an IgG4/IgG cell ratio of ∼50%.
One hundred and sixty milliliters of sanguineous fluid were removed during pericardiocentesis. The fluid was found to be a lymphocyte-dominant exudate with a borderline increase in adenosine deaminase of 42.2 IU/l and chronic inflammatory cells. Thoracoscopic pericardial biopsy was performed, and a histopathologic study demonstrated lymphoplasmacytic infiltration with fibrosis and a high plasma cell ratio. IgG4-positive plasma cells were >50/HPF and the IgG4/IgG ratio was ∼50% (Figure 1C), indicating IgG4RD. Serum IgG4 levels were elevated to 2340.0 mg/l (normal range, <135). Infectious or other inflammatory diseases, malignancy, or IgG4RD involvement in other organs were all thoroughly excluded.
We consulted rheumatology, and the patient was diagnosed with IgG4RD involving the pericardium based on clinical, imaging, serologic and pathological results. He was started on glucocorticoid therapy and is being monitored clinically.
Discussion
IgG4RD is a recently recognized systemic fibroinflammatory disease that typically affects multi-organs, most notably the lymph nodes, salivary/lacrimal glands, retroperitoneum/mediastinum, pancreas/biliary tract/spleen and respiratory system, ultimately leading to fibrosclerotic changes.1,2 IgG4RD with cardiovascular involvement has also been reported, with the majority of cases limited to coronary arteritis and periaortitis,3 and only a small proportion of pericardial and valvular heart disease.2,4
Corticosteroid therapy is the first-line treatment for IgG4RD. Patients usually respond well to medium doses of glucocorticoids, and long-term maintenance is required to avoid relapse. Glucocorticoids, with or without surgical intervention, are used to treat IgG4RD involving the cardiovascular system.4 In patients with IgG4-related pericarditis, early diagnosis and corticosteroid therapy may prevent progression to constrictive pericarditis requiring pericardiectomy.
Idiopathic etiology is one of the most prevalent causes of ECP, and ECP is often deemed idiopathic after tuberculosis, neoplasm, uremia or postirradiation have been ruled out.5,6 We insist, however, that IgG4RD should be listed as one of the causes of pericarditis because it can be challenging to detect IgG4RD without suspicion, and corticosteroid therapy can improve the outcome of the IgG-related pericarditis.
Author contributions
Jihee Son (Data curation [lead], Investigation [equal], Resources [lead], Visualization [lead], Writing—original draft [equal]) and Sun Hwa Lee (Conceptualization [lead], Investigation [equal], Project administration [equal], Supervision [lead], Writing—original draft [supporting], Writing—review & editing [lead])
Consent
Patient consent was obtained before submitting this case report.
Conflict of interest
None declared.

{kind=link}