





A 70-year-old man presented to the emergency department with right periorbital region pain and swelling, which were noted after a fal 1 day prior to the presentation. Upon arrival, he had clear consciousness and stable vital signs. Physical examination showed ecchymosis and tenderness around his right periorbital region. The pupils were isocoric and reactive to light, eye movements were within the normal limits, and visual acuity was intact. A plain Water’s radiographic view was obtained (Figure 1A), showing no apparent fracture lines but with a crescent-shaped radiolucency in the right superior orbit, known as black eyebrow sign, leading to a suspicion of occult orbital wall fracture. Computed tomography confirms the diagnosis of nondisplaced fractures at the medial and inferior orbital wall and intra-orbital emphysema. The patient was treated conservatively and was followed up at the outpatient department.
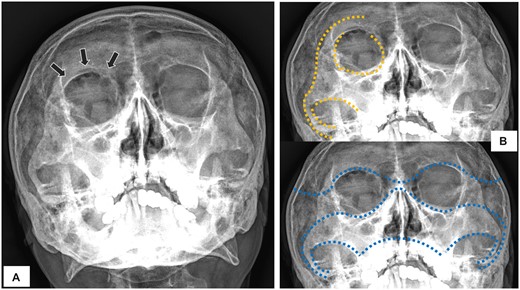
Plain radiography of Water’s view (A) showing black eyebrow sign (arrows); (B) depicting the elephantine lines of Dolan (upper panel) and McGrigor’s lines (lower panel).
Facial trauma is a common occurrence; however, the first-line imaging tool, plain radiographs, has a low sensitivity in detecting facial bone fracture, leading to frequent misdiagnosis.1 Utilizing the Dolan or McGrigor’s lines (Figure 1B) helps in identifying facial bone fracture.2 Additionally, the diagnosis should also be suspected when there are indirect signs, such as air-fluid level in the maxillary sinus, herniated intra-orbital fat (teardrop sign) and intra-orbital free air.3 The black eyebrow sign refers to pathological air that is collected in the superior aspect of the orbit, resulting in a curvilinear radiolucency that resembles an eyebrow on radiographs. This finding indicates inferior or medial orbital wall fracture, where air leaks from the adjacent sinus into the superior aspect of the orbit.
Authorship
B.-H.K. acquired the clinical data, drafted the manuscript and maintained contact and consent with the patient. J.-T.S., C.-M.F. and K.-C.T. served as scientific advisor and did revision of the manuscript. C.-J.C. was responsible for editing the article and gave final approval to the manuscript.
Conflict of interest
None declared.

{kind=link}