





A 20-year-old girl had fever, cough with purulent expectoration and anorexia for the past 6 weeks. Chest auscultation revealed crepitations in both lung fields. There was no lymphadenopathy, and oxygen saturation on pulse oximeter was 98% on room air.
Blood investigations showed elevated erythrocyte sedimentation rate (95 mm in the first hour, normal < 20) and C-reactive protein (48 mg/l, normal < 10). Total leucocyte count, procalcitonin, liver and kidney function tests were normal. Inhomogeneous opacities were observed in both upper zones and left middle zone on chest radiograph. A computed tomogram of the chest showed scattered nodules in both lungs distributed in centrilobular pattern. Some areas showed clustering of nodules around prominent airways in branching pattern, which is called the ‘tree-in-bud’ appearance (Figure 1A, described further).1 Inflammation of the terminal airways or collection of secretions in their lumen leads to thickening of the bronchioles which appear on computed tomogram as linear branching structures. Involvement of the lung parenchyma around peripheral airways gives rise to centrilobular nodules. Combined appearance of centrilobular nodules along with thickened airways is likened to a tree with budding branches (Figure 1B). Necrotic mediastinal lymph nodes were also observed in the computed tomogram. Sputum examination of the patient showed bacilli which stained positively with acid-fast stain. A combination of rifampicin, isoniazid, ethambutol and pyrazinamide was initiated. Culture of the sputum showed growth of Mycobacterium tuberculosis, which was sensitive to all the first-line anti-tubercular drugs. Pyrazinamide was discontinued after 2 months; rifampicin, isoniazid and ethambutol were continued for the next 4 months. Six months later, there was disappearance of the symptoms, weight gain of 4 kg, and normalization of acute phase reactants was observed.
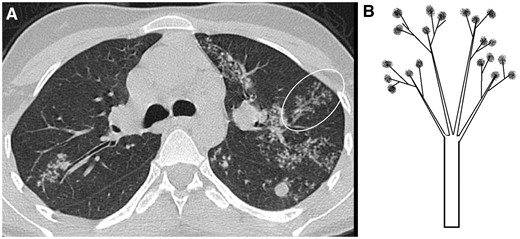
Computed tomogram of the chest showing thickened terminal airways in branching pattern along with centrilobular nodules (encircled area in A). It is called the ‘tree-in-bud’ appearance as it is likened to a tree with budding branches (B).
‘Tree-in-bud’ appearance is a relatively non-specific computed tomographic finding seen in a variety of conditions. However, pulmonary tuberculosis is the commonest cause in developing countries.2 It may also be seen in other bacterial (Staphylococcus aureus and Haemophilus influenzae), fungal (Aspergillus) and viral (cytomegalovirus and coronavirus disease 2019) infections.1 Less common causes include malignancy, pulmonary vasculitis, interstitial lung disease and inhalation of fumes. Other radiological and laboratory features help in making the correct diagnosis. Inflammation of the peripheral airways and surrounding lung parenchyma is the underlying pathogenesis.3
Our patient had classical clinical features of pulmonary tuberculosis. Radiological features (including ‘tree-in-bud’ appearance and necrotic mediastinal lymph nodes) strengthened the suspicion and microbiological results confirmed the diagnosis. Patient recovered completely after 6 months of anti-tubercular therapy.
Informed consent: Written informed consent was obtained from the patient described in the article.
Conflict of interest: None declared.
Author contributions
Ashish Sharma (Conceptualization-Lead, Data curation-[equal], Formal analysis-Lead, Resources-[equal], Software-[equal], Supervision-Lead, Validation-[equal], Visualization-[equal], Writing—original draft-Lead, Writing—review & editing-[equal]) and Ankita Sheoran (Conceptualization-Supporting, Data curation-[equal], Formal analysis-Supporting, Resources-[equal], Software-[equal], Supervision-Supporting, Validation-[equal], Visualization-[equal], Writing—original draft-Supporting, Writing—review & editing-[equal]).

{kind=link}