





A previously well 27-year-old Bangladeshi man developed insidious left-hand weakness for 6 days. Physical examination showed marked wasting over the left forearm and hand muscles with sparing of the brachioradialis muscle. Atrophy of the hypothenar eminence was more prominent compared to thenar eminence, suggestive of reverse split hand syndrome (Figure 1A). Power testing revealed unilateral left C7-T1 segmental weakness and normal sensation. Nerve conduction study and electromyography corroborated these findings which were most marked in the ulnar innervated muscles. Magnetic resonance imaging (MRI) of the cervical spine revealed focal cervical cord atrophy with C5–7 intramedullary hyperintense signal in neutral position and anterior displacement of the posterior dura with prominent posterior epidural space and flow voids in flexion position (Figure 1B). He was diagnosed with Hirayama disease and advised to apply a hard cervical collar to prevent neck flexion injury.
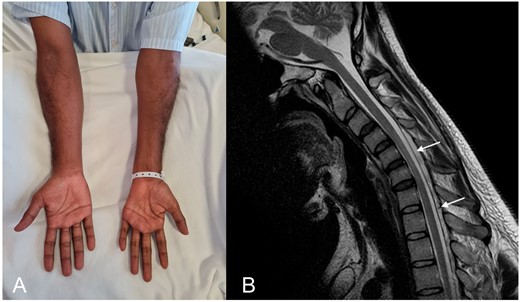
Reverse split hand syndrome and distinctive magnetic resonance imaging features in Hirayama disease. (A) The examination is notable for marked wasting over the left forearm and hand muscles with sparing of the brachioradialis. Reverse split hand syndrome due to dissociated atrophy of the abductor digiti minimi compared to the abductor policis brevis is seen. (B) T2-weighted sagittal MRI image in flexion shows anterior displacement of the posterior dura and prominent posterior epidural space with flow voids.
Hirayama disease is a rare, non-familiar monomelic amyotrophy classically described in young men of Asian descent.1 It is postulated to be due to chronic ischemia of the anterior horn cells typically at C7-T1, and predisposed by limited dural sac laxity.2 Patients often present with weakness and wasting in the hand and forearm, with sparing of the brachioradialis muscle, giving rise to oblique amyotrophy.1 This clinical sign, along with the reverse split hand syndrome due to dissociated atrophy of the abductor digiti minimi compared to the abductor policis brevis may be helpful bedside clues to differentiate Hirayama disease from untreatable conditions such as amyotrophic lateral sclerosis.3 Disease course is initially slowly progressive followed by spontaneous arrest within several years.1 The presence of muscle atrophy in the hand and forearm of our patient suggested that the onset likely preceded the duration reported, with the current presentation representing the initial progressive phase of the disease. Distinctive radiological features include forward displacement of the cervical dural sac and compressive flattening of the lower cervical cord during neck flexion.4,5 The diagnosis should be considered in young men who present with insidious onset, unilateral C7-T1 segmental weakness, oblique amyotrophy, reverse split hand syndrome and distinctive spine imaging features. The use of cervical collar and surgical intervention have been proposed as treatment options.1,6
Conflict of interest. None declared.

{kind=link}