





Abstract
A key lesson of the coronavirus pandemic was the importance for pro-social behaviour of popular trust in key information sources. Yet existing studies rarely consider the role of people’s trust in a range of different information sources, and the relationship between such trust and particular attitudes and behaviours among individuals. This study goes beyond the general mantra that ‘trust matters’ and explores more specific effects, relating to trust in particular actors and for particular outcomes. Based on a survey fielded on a representative sample of the British population conducted towards the end of the pandemic, we find evidence that people’s coronavirus attitudes and behaviours are particularly related to their trust in scientific experts and, in some cases, to their trust in local councils. However, trust in these actors is not uniformly associated with people’s coronavirus beliefs and actions. This suggests that the link between people’s trust and their pro-social attitudes and behaviours is often specific rather than general. The results hold important implications for the design of effective public communication strategies in the event of any future health emergency.
The coronavirus pandemic originating in late 2019 was, for the populations of most countries, one of the most disruptive and traumatic events ever experienced. The Millions of people died from COVID-19, healthcare systems were put under unprecedented strain and governments presided over some of the most far-reaching systems of social control introduced outside wartime. Many countries are now seeking to identify lessons from the episode, and to ready themselves for any future viral pandemic. In the UK, the independent COVID-19 inquiry, which started work in summer 2022, is tasked with assessing the national response to the pandemic and helping the country prepare for any future health emergencies.1 Among the central issues for any future planning is how citizens might be presented with health and risk-related guidance in ways that maximise their acceptance of scientifically valid information and their compliance with socially-beneficial rules and restrictions. At the outset of the coronavirus pandemic, it was widely accepted that these outcomes were likely to be strongly influenced by people’s dispositions towards relevant public actors and institutions. In particular, people’s trust in key information sources and rule-makers was seen as a central resource in ensuring appropriate and effective public responses to the challenges posed by the pandemic (e.g., Van Bavel et al. 2020). A range of studies conducted during the coronavirus pandemic provided support for this intuition, showing how individuals’ decisions over health choices and behaviours were conditioned by their feelings of trust in partisan, scientific and medical actors (for reviews, see Seyd and Bu 2022; Devine et al. 2024).
Yet there remains some debate over the role of trust in shaping people’s support for, and compliance with, health-related restrictions and norms. Alongside studies suggesting that feelings of trust were closely associated with individuals’ pro-social beliefs and actions, other analyses identified weaker associations with trust (for relevant reviews, see Kooistra and van Rooij 2020; Seyd and Bu 2022; Devine et al. 2024). One way of making sense of these competing findings is to focus more closely on the conditional effects of trust, namely by exploring how people’s trust in particular actors and agencies is associated with particular attitudes and behaviours among individuals. Our intuition here is that trust may well have specific, rather than general, associations with people’s beliefs and actions. That is, individual attitudes and behaviours may be more closely related to feelings of trust in some actors than to trust in others. Similarly, feelings of trust may be more closely associated with certain attitudes and behaviours among individuals than to others.
Existing studies hint at such particularities or conditionalities in the association between trust and coronavirus behaviours. Thus, analyses have shown that some actions, such as getting vaccinated against COVID-19 and complying with social hygiene measures, are more closely associated with people’s feelings of trust in health and scientific actors than with their trust in partisan actors (e.g., Dohle, Wingen and Schreiber 2020; Jennings et al. 2021). Other analyses have found that people’s trust in health agencies is more closely associated with their tendency to get a COVID-19 vaccination than with other behaviours, such as social distancing (e.g., Devine et al. 2024). There is thus some evidence that the associations between people’s trust in key social actors and agencies and their coronavirus attitudes and behaviours might be specific rather than general.
Yet there remains considerable scope for further parsing the associations between people’s feelings of trust and their health-related beliefs and actions. In particular, we might wish to explore the effects of people’s trust in a wider range of social actors than those explored in most previous studies. In contemporary societies, people access information from a wide range of sources, both mainstream or ‘official’ (notably the government, the regular media and scientific and medical experts) and non-mainstream or ‘unofficial’ (such as social media, community leaders and personal contacts) (Nielsen et al. 2020). Given the range of sources that individuals draw on for information, we need to understand more clearly how people’s trust in a variety of social actors might be associated with their attitudes and behaviours around the coronavirus. In particular, might people’s beliefs and actions be associated with their evaluations of some non-mainstream information sources? Might people’s trust in these sources thus ‘reach the parts’ that their trust in more mainstream sources does not?
Alongside attention to a wider set of information sources, we also need to explore how feelings of trust might be associated with a range of attitudes and behaviours among individuals. While, as just noted, existing studies have explored the association of trust with activities such as vaccination uptake, we have less evidence about the relationship between people’s trust and other important behaviours (such as working from home) and beliefs (such as support for social restrictions and lockdowns). This situation has not been helped by the tendency of many studies on the coronavirus pandemic to group together a range of individual actions into aggregate indices of ‘compliant behaviour’ (e.g., Seyd and Bu 2022). This approach hinders our understanding of whether people’s trust in key social actors might be related to some pandemic-related attitudes and behaviours but not to others.
If we are to adequately learn the lessons of the coronavirus pandemic, and to implement effective strategies to prepare for any future health emergencies or pandemics, we need a more detailed understanding of how citizens evaluate particular sources of information and of how these evaluations might be associated with particular beliefs they hold and behaviours they engage in. This way, we can move beyond potentially simplistic conclusions that ‘trust matters’, and pinpoint the potential effects of trust in specific objects and on specific outcomes. In turn, a more precise understanding of the role of trust could underpin a more tailored—and thereby more effective—approach to public information-provision and guidance in any future health emergency.
This study extends earlier national and cross-national analyses that explored how trust motivates important social behaviours by explicitly examining the effects of people’s trust in a range of different information sources, both ‘mainstream’ and ‘non-mainstream’. It further extends existing studies by exploring how trust across these different information sources is associated with a range of pro-social actions and beliefs, ranging from coronavirus-compliant behaviours to wider support for official restrictions and lockdown measures. The study analyses these issues using data drawn from a representative survey of British citizens. The survey was conducted in early 2022, towards the end of the coronavirus pandemic, when people had become accustomed to the public provision of health information and guidance, to the need for individual protective behaviour and to the reality and nature of social lockdowns. The survey was thus able to measure a relatively informed set of public responses on these issues, as well as having the space to probe people’s trust in a range of information sources and their behaviours and beliefs across a range of coronavirus measures.
1. Trust and health behaviours
Official information played a central role in the public management of the coronavirus pandemic by equipping citizens with the tools to make effective choices on issues around personal health and risk management. In turn, citizens faced with such information had to decide whether to accept it and to follow official guidance and rules. Studies have long stressed the importance in these decisions of feelings of trust (Hovland et al. 1953; Pornpitakpan 2004). Trust plays a significant role because people often lack the requisite knowledge to evaluate technical risk-related information, and instead fall back on cognitively simpler evaluations such as the perceived trustworthiness of the source (Renn and Levine 1991; Siegrist and Cvetkovich 2000). As a result, trust is widely seen to be a key element in shaping citizens’ receptiveness to, and compliance with, information around social risk. Studies conducted prior to, as well as during, the coronavirus pandemic show that higher levels of individual trust in agencies like national governments are associated with greater take-up of vaccination opportunities [Larson et al. 2018; de Figueiredo et al. 2020; see the reviews by Adhikari, Cheah, and von Seidlein (2022) and Sapienza and Falcone (2022)] and engagement in pro-social behaviours such as social distancing and mask-wearing (e.g., Brodeur et al. 2020; Seyd and Bu 2022; Devine et al. 2024).
Yet existing studies suggest that such health-related activities tend to be more strongly linked to individuals’ trust in certain bodies than to their trust in others. Thus, reported uptake of coronavirus vaccination opportunities has been found to be more closely associated with people’s trust in scientists, medical practitioners and healthcare organisations than with their trust in political actors such as national governments (Dohle, Wingen and Schreiber 2020; Jennings et al. 2021, 2023; Lindholt et al. 2021; Rosek et al. 2021; Han et al. 2022; Viskupič, Wiltse, and Meyer 2022; Barceló et al. 2023; Devine et al. 2024). Similarly, when it comes to observing coronavirus rules—by wearing a face-covering, for example—the associations with people’s expressed trust in scientists have generally been found to be stronger than the associations with their expressed trust in politicians (Dohle, Wingen, and Schreiber 2020; Algan et al. 2021; Bicchieri et al. 2021; Kazemian, Fuller, and Algara 2021; Pagliaro et al. 2021; Han et al. 2022). However, a recent meta-analysis found some health-compliant behaviours (such as social distancing and mask-wearing) to be more closely related to people’s trust in government than to their trust in public health authorities (Devine et al. 2024).
These findings suggest that the relationship between trust and health-related behaviours is conditional; it depends on which social actor or information source is being evaluated, and on what form of social behaviour is being undertaken. While empirical studies conducted during the coronavirus pandemic have thus helpfully begun to explore people’s evaluations of particular information sources and their association with particular health-related behaviours, most studies have focussed on a rather narrow set of information sources, notably national governments and scientific experts. This focus may reflect the principal mediums of information-provision adopted during the pandemic by many countries—including Britain—where televised press conferences and health broadcasts tended to be fronted by senior politicians and scientific advisers (Lavazza and Farina 2020). Yet while many citizens looked to these figures for information and guidance on the coronavirus, others also gleaned information from a variety of alternative sources, including social media (Nielsen et al. 2020), local tiers of government and community leaders. In today’s society, where it is easier for people to access information across a range of sources, it seems important to understand what associations their evaluations of different information outlets might have with key health-related behaviours and attitudes.
Moreover, while empirical studies have begun to explore the associations between trust and different forms of social behaviour, these variations have not been parsed as finely as they might. This has not been helped by analysts’ frequent tendency to aggregate different coronavirus behaviours among individuals into composite scales—in the form of a general ‘compliance index’—rather than retaining them as individual items. Granted, the rare studies that measure individual behaviour across a range of specific activities suggest largely consistent associations with trust in particular actors (Bicchieri et al. 2021; Han et al. 2022; Devine et al. 2024). For example, Han et al. (2022) cross-national analysis finds that different coronavirus behaviours are consistently associated with people’s trust in scientists, while also being fairly consistently not associated with people’s trust in government. However, the variety of coronavirus-related rules and restrictions introduced by national governments during the pandemic—and thus the variety of different practices citizens were asked to follow—makes it important that analysts explore the associations between trust and a range of individual behaviours and beliefs. Without such a broad focus, we risk failing to detect whether people’s trust in information sources might be more closely associated with certain social behaviours and attitudes than with others.
Based on these previous studies, we thus hypothesize that individuals’ coronavirus attitudes and behaviours will be associated with feelings of trust and that, in general, these associations will be stronger when it comes to people’s trust in scientific and medical experts than when it comes to their trust in politicians. We also hypothesize that people’s trust in particular information sources will be more strongly associated with certain behaviours and attitudes than will their trust in other sources. Specifically, we hypothesize that ‘personal’ coronavirus-protective behaviours (such as getting vaccinated and wearing a face-covering) will be particularly closely associated with people’s trust in scientific and medical experts, reflecting these actors’ roles in quantifying the costs and benefits of such individual actions.2 Yet when it comes to more social or ‘collective’ measures (such as compliance with the requirement to work from home and support for such measures as the mandatory closure of schools), we hypothesize closer associations with people’s trust in politicians, as governments are more clearly implicated in such decisions. The associations between people’s trust in other information sources—such as the media, local government and community actors—and their coronavirus behaviours and attitudes are less clearly identified in existing studies, and thus remain a more open question for analysis.
2. Data and methods
To explore levels of trust in different information sources and their association with individual beliefs and behaviours, we draw on data collected by a specially designed survey of the British population (n = 1,501), conducted by Ipsos-MORI in February 2022.3 The survey was conducted online and based on a sample of adults aged 18+ drawn from the company’s online panel. To ensure the sample was representative of the national population, quotas were set on age, gender, region and working status. In addition, the results were weighted to the known offline population proportions for age, working status, social grade within gender and region.
The survey included batteries of questions on trust in different sources of information about the coronavirus, on self-reported coronavirus behaviours including vaccination uptake, and on attitudes towards official coronavirus restrictions and rules. As far as possible, the measures fielded on the survey drew on indicators and scales whose validity had been demonstrated in previous studies. Full details of all the survey measures, along with response options and descriptive statistics, are provided in Appendix 1.
The survey measured people’s trust in nine different sources in relation to “providing information about COVID-19”: government ministers, the local council, scientific, and medical experts, local doctors, television news, newspapers, social media platforms, local faith leaders, and local ethnic group leaders. People’s trust in each of these sources was recorded on an 11-point (‘no trust’ to ‘full trust’) scale. The survey measured three sets of coronavirus-related behaviours and attitudes among individuals. First, it measured individuals’ own (self-reported) compliance with four different behaviours: wearing a face-mask, avoiding indoor gatherings, working from home and maintaining a distance from other people.4 Second, it measured personal vaccination behaviour and intentions, in particular respondents’ current COVID-19 vaccination status and reported likelihood of taking up any future COVID-19 vaccination. Third, the survey asked respondents whether they supported government health-related restrictions in four areas: a requirement that individuals present evidence of vaccination to access social venues (the so-called ‘vaccine passport’), the obligatory wearing of face-masks in public areas, enforced working from home and the mass closure of schools.
These three sets of health-related behaviours and attitudes form our outcomes to be explained, with trust in different social actors serving as the principal explanatory variable. In order to identify the relationships between people’s trust in particular sources and particular health-related behaviours and attitudes, we ran a number of discrete regression models, each measuring an individual behavioural or attitudinal outcome and trust in an individual information source. Each model also included indicators tapping factors that potentially covary with both trust and our outcome variables, and whose inclusion helped to ensure the accurate identification of any relationships. These factors were: (i) attitudes towards lockdown restrictions, captured through two survey items asking respondents to indicate on a scale their personal preference for reducing coronavirus infections against either protecting the economy or protecting people’s freedom5; (ii) fear of the coronavirus, both personally, and in relation to one’s locality and the country6; (iii) feelings of civic obligation, measured by responses to a statement on whether citizens have a “duty to follow the coronavirus rules”, and (iv) various political values and choices, notably conformity with authority (measured by a six-item libertarian-authoritarian scale; Evans, Heath, and Lalljee 1996), vote choice in the 2016 Brexit referendum, and vote choice at the previous national election in 2019. To control for the fact that individual behaviour might also reflect personal understanding of the coronavirus, our models included a coronavirus knowledge scale (comprising answers to a four-item quiz7). The models also included variables capturing individuals’ age, gender, ethnic group, education, and socio-economic status (proxied by reported household income).
In the models, continuous independent variables are normalised (taking values between 0 and 1) in order to maximise their comparability. ‘Don’t know’ responses are omitted from the analysis. The first set of models estimates individuals’ coronavirus behaviours, which are measured on six-point scales. The third set of models estimates individuals’ support for different coronavirus restrictions, which are measured on five-point scales. Both sets of models employ ordinary least-squares (OLS) regression.8 The second set of models estimates individuals’ current vaccination status, which is measured in binary form and modelled using binary logit. Future vaccination status is measured through a four-category response option (‘I would not get vaccinated’, which served as the base category, ‘I would only get vaccinated if required’, ‘I might get a future vaccination’, and ‘I would get a vaccination as soon as it became available’; see Appendix 1 for details), and is modelled using multinomial logit.
3. Results
We begin by examining how far British citizens trust different sources as providers of information about COVID-19. The results are shown in Fig. 1. Our results comport with previous studies, showing significantly lower levels of trust in government ministers than in local doctors and scientific experts. Two years into the pandemic, we find continued high levels of trust in scientific and medical experts, with mean trust at seven or more on a 0 (no trust at all) to 10 (full trust) scale. We find that people trust local government more than they do national government, and television news more than newspapers. Trust in local ethnic and faith leaders falls towards the lower end of the distribution, with social media platforms attracting very low ratings (mean trust score of 2.6 on a 0–10 scale).
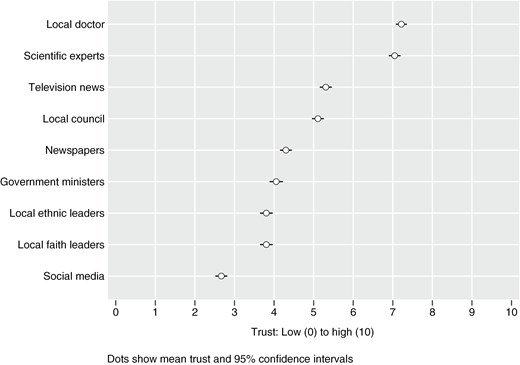
Trust in different information sources.
3.1 Coronavirus behaviours
How are these feelings of trust in different information sources associated with individuals’ personal reported coronavirus behaviours? The results of our models are presented in full in Appendix 2 and in summary graphical form in Fig. 2. The figure shows the coefficients for people’s trust in each information source where these have been entered separately into models predicting compliance with each of four coronavirus-suppressing actions: wearing a face-mask, avoiding other people, working at home, and keeping a distance from other people. The whiskers associated with each point estimate capture 95% confidence intervals; a statistically significant association is indicated by whiskers that do not overlap with zero (marked by the vertical line positioned at 0).9
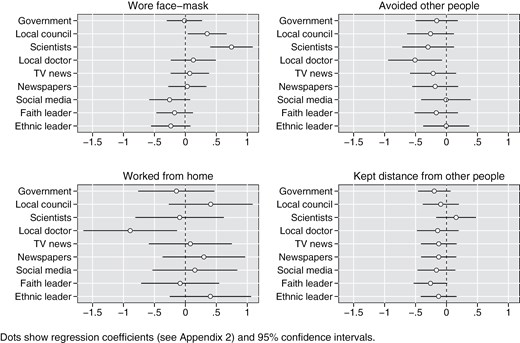
Trust in information sources and coronavirus behaviours.
The results in Fig. 2 suggest that people’s trust in different information sources is generally not closely associated with their coronavirus behaviour (since the confidence intervals associated with most of the coefficients on trust overlap with zero, indicating that we cannot reject the null hypothesis of no association between trust and behaviour). People’s trust in scientists is significantly associated with just one form of protective behaviour, namely wearing a face mask. Higher levels of trust in scientists among individuals are associated with higher reported rates of wearing a face-covering. This finding is in line with our hypothesis that people’s trust in scientists would be particularly closely associated with ‘personal’ forms of preventive behaviour. When it comes to the three other behaviours—avoiding other people, social distancing, and working from home—we find no significant association with people’s trust in scientists. In the case of people’s trust in central government, there is no significant association with any of the four behaviours, although when it comes to local government there is a significant positive association with wearing a face-mask. The results also suggest significant, but negative, associations between people’s trust in local doctors and avoiding other people and working from home. However, in tests that adjust for multiple comparisons, these coefficients fall short of statistical significance (P < .05).10
These results run counter to many previous studies and to our own hypothesis, which suggested a significant positive association between people’s feelings of trust and their engagement in pro-social behaviours. As observed above, however, it is important to note that some other studies, conducted in a variety of contexts, have identified weak and/or statistically insignificant associations between feelings of trust and coronavirus-related behaviours among individuals. In addition, studies have also shown that the relationship between trust and behaviour varies over time (Seyd and Bu 2022); it may be that, two years into the pandemic, people’s reported behaviours had become ingrained and largely independent of their trust in different information sources.11 We also observe that individuals’ precautionary behaviours are closely related to beliefs and feelings beyond trust, notably social duty and fear of the coronavirus (Appendix 2). These beliefs and feelings—rather than evaluations of trust—appear to be doing most of the ‘heavy lifting’ in encouraging pro-social behaviours.
Note, however, that some of these relationships are specific to particular behaviours. For example, we find that people’s personal fear of contracting COVID-19 is positively associated with them reporting avoiding other people, social distancing and working from home (Appendix 2, models b–d). Yet when it comes to mask-wearing, behaviour is instead more closely associated with individuals’ concern about coronavirus in the wider locality and country as a whole (Appendix 2, model a). These variations make intuitive sense; wearing a face-covering is a sociotropic measure designed to protect others, while avoiding other people, social distancing and home-working involve greater self-protection. Similarly, we find that feelings of social duty appear to motivate compliant behaviour when it comes to mask-wearing, avoiding other people and social distancing, but not when it comes to home-working. Again, there is a logic to this. The first three behaviours involve personal choices that are likely to be shaped by feelings of social duty. By contrast, working from home reflects a mandate issued by businesses and workplace organisations, and is thus less likely to be shaped by individual feelings of social duty. Finally, we find that people prioritising the protection of individual freedoms are significantly more likely to report not wearing a face-mask than those prioritising the reduction of coronavirus infections (Appendix 2, model a). However, in the case of social distancing, non-compliant behaviour is more closely associated with prioritising protection of the economy than prioritising individual freedoms (Appendix 2, model d). Thus, while the relationships between people’s coronavirus behaviours and their trust in different information sources are largely and consistently weak, the relationships between those behaviours and other beliefs and feelings are often stronger and also often specific to particular behaviours.
3.2 Vaccination status
We now turn to examining the relationship between people’s feelings of trust and their vaccination behaviour. The survey asked respondents separate questions about whether they had already received a COVID-19 vaccination and whether they would be likely to take up a COVID-19 vaccination in future. Among our sample, more than nine in ten said they had already had at least one dose of the COVID-19 vaccination, while more than six in ten indicated they would immediately take up any future COVID-19 vaccination opportunity (see Appendix 1). We model existing and future vaccination status in a similar way to the previous models of coronavirus behaviour, namely by identifying the associations with trust in the nine different information sources along with the same battery of control variables.
The results—which are presented in full in Appendix 3 and summarised in Fig. 3—show a very similar picture for people’s current vaccination status and their reported likelihood of immediately getting a vaccination in the future. For both, trust in a range of information sources is positively associated with vaccination. The only exceptions are social media and local faith and ethnic leaders, where trust has no significant association with vaccination behaviour.12
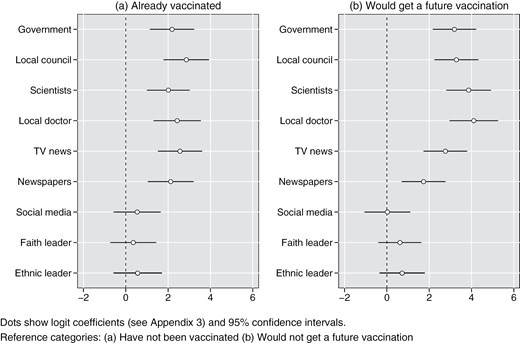
Trust in information sources and vaccination status.
These results do not mean that people’s trust in each institution is individually and independently associated with vaccination status. It is well known that people express similar trust judgements across different institutions (Seyd 2024: 28, 29). People’s trust therefore often generalises across social actors rather than being specific to particular actors.13 We can test whether people’s trust in different information sources is associated with their vaccination behaviour by simultaneously including in the models measures of trust in central and local government, scientists, local doctors and television news (see also footnote 13). In the case of existing vaccination status, this model (Appendix 5, model a) suggests that only people’s trust in local councils is independently associated with the outcome. We do not take this to imply that local councils are uniquely placed to encourage vaccination take-up. It may well be that people’s expressions of trust in local councils overlap particularly closely with more general feelings of trust in institutions (although the result might also suggest that local councils are well-positioned to encourage vaccination take-up across the population). In the case of future vaccination intentions, the model only identifies independent associations with people’s trust in scientists and local doctors (Appendix 5, model b). Again, this does not imply that people’s prospective vaccination behaviour depends only on their trust in scientific and medical experts; the role of people’s trust in these actors might overlap with the role of a wider—and latent—institutional trust. However, the results do provide at least some support for our hypothesis that ‘personal’ coronavirus-protective behaviours such as vaccination intentions will be more closely associated with people’s trust in scientific and medical experts than with their trust in politicians.
3.3 Support for coronavirus restrictions
Having examined the relationship between trust and people’s behaviour, we now turn to explore the relationship with their attitudes towards different coronavirus restrictions. Our survey asked respondents for their level of support for four such measures, namely vaccine passports, mandatory face-masks, enforced home working and school closures. On a five-point scale (where 1 = strongly oppose and 5 = strongly support), support was highest for mandatory face-masks (mean figure of 3.83), followed by requiring home working and vaccine passports, with compulsory school closures attracting the lowest level of support (mean figure of 2.64).
We ran the same set of models as those used to predict people’s compliance and vaccination behaviours. The results of these models are presented in full in Appendix 6 and in summary form in Fig. 4. They show that people’s trust in a variety of information sources is associated with support for some restrictions (notably vaccine passports, where support is significantly associated with people’s trust in government ministers, local councils, scientific experts, local doctors, television news and newspapers) but not for others (notably required working from home, where support is only significantly associated with trust in scientific experts and social media). As before, these results do not suggest that people’s trust in different information sources are each individually associated with their attitudes towards coronavirus restrictions. We can see this by entering into the same models predicting support for official restrictions measures of trust in central and local government, scientists, doctors and television news (see footnote 13). Where trust in multiple information sources is simultaneously entered, the model results (Appendix 7) suggest that only trust in scientists is an independent predictor of support for vaccination passports, compulsory mask-wearing and required working from home.14 In other words, there may be a generalised ‘trust in institutions’ associated with support for these coronavirus measures, yet if so this latent trust appears to be most closely tapped by people’s feelings towards scientists.
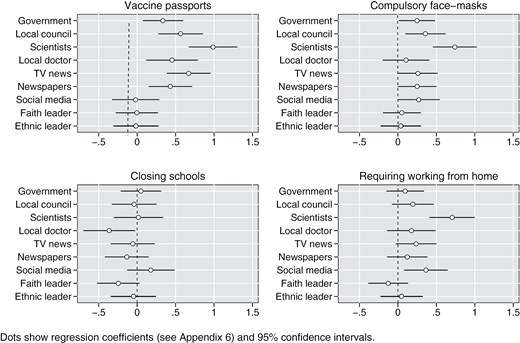
Trust in information sources and support for coronavirus restrictions.
Moreover, the association with trust in scientists is particularly noticeable when it comes to support for measures around ‘personal’ behaviour (such as requiring evidence of a coronavirus vaccination and wearing a face-mask); it disappears when it comes to support for non-personal or ‘collective’ measures such as closing schools. In the case of support for school closures, we anticipated a closer relationship with people’s trust in government, yet our results provide no evidence of such an association.
We also observe that these varied associations with trust are obscured if, instead of studying people’s support for individual coronavirus restrictions, we aggregate that support into a single, combined, measure. Creating a summed scale of support for the four coronavirus restrictions (α = 0.80) reveals a statistically significant and positive coefficient with people’s trust in scientists. This might be taken to imply that people’s trust in scientists is closely related to their support for both ‘personal’ and ‘collective’ forms of coronavirus restriction. In reality, as the results from our disaggregated models show, people’s trust in scientists is only related to their support for measures targeting personal behaviour, not to their support for more collective restrictions.
When it comes to other factors associated with people’s support for coronavirus measures, we find some consistency in identified relationships (Appendix 6). Thus, people’s beliefs about the appropriate balances to be struck between lockdowns and the protection either of personal freedoms or of the economy are—unsurprisingly—associated with their support for each of the four coronavirus restrictions. Yet when it comes to other attitudes and beliefs, we find less consistent relationships; there are associations with people’s support for some coronavirus restrictions but not with their support for others. Thus, people’s sense of social duty is strongly associated with their support for vaccine passports and mandatory face masks, yet only weakly associated with their support for working from home and not significantly associated with their support for mandatory school closures. Similarly, while people scoring high on authoritarian values are more likely than their libertarian counterparts to favour vaccine passports, they are no more likely to favour other coronavirus restrictions (our results here tally with those of Mellon, Bailey, and Prosser (2021)], who found libertarian-authoritarian attitudes to only weakly correlate with individual support for different coronavirus restrictions). People’s personal anxiety about the coronavirus and their anxiety about the coronavirus at the local and national levels are both positively associated with support for school closures. Yet support for compulsory mask-wearing is only associated with people’s social fears, not with their personal fears. By contrast, personal anxiety is more closely associated than is social anxiety with support for vaccine passports. Our results thus provide some evidence that people’s feelings of trust in different information sources and their wider attitudes and beliefs are associated in differing ways with their support for particular coronavirus restrictions.
4. Discussion
This study has sought to extend our understanding of how people’s trust in different sources of health-related information might be associated with important social behaviours and attitudes in the context of a viral pandemic. In particular, the study has sought to go beyond claims about the role of trust in a narrow set of social actors, and in relation to a generic set of ‘coronavirus compliance’ behaviours. Instead, it has tested the associations between people’s trust in numerous different information sources and a range of health-related behaviours and attitudes. We hypothesized that people’s behaviours and attitudes would be most closely-associated with their evaluations of (i.e., trust in) scientific experts, and that these associations would be particularly strong in the case of ‘personalised’ behaviours (such as wearing a face-mask and getting vaccinated), and weaker in the case of more ‘collective’ measures (such as support for closing schools).
Our results provide some support for these intuitions. When it comes to protective behaviours, we find people’s trust in scientists to be associated particularly with wearing a face-mask. Yet aside from this example, trust in different social actors is generally not significantly associated with people’s propensity to take preventive health actions. Trust in a range of information sources appears to be more important for individuals’ vaccination status. In modelling that tests trust in different sources simultaneously rather than individually, we identify a particular role of trust in local councils in the case of individuals’ existing vaccination status, and of trust in scientists in the case of their future vaccination behaviour. Individual decisions over vaccination are not, however, associated with trust in social media sources or with local ethnic and religious leaders. While sections of the population undoubtedly look to these sources for information and guidance, our results provide little evidence that individuals’ subsequent behaviours are linked to their feelings of trust in these actors. Finally, we find that people’s support for various coronavirus restrictions is particularly closely associated with their trust in scientists.
Overall, our results confirm the results of previous studies conducted in Britain and elsewhere which identify the role played by people’s trust in scientists in shaping people’s coronavirus-related behaviours and attitudes. Granted, this study finds that other beliefs—such as fear of the coronavirus—also play a significant role in shaping individual behaviours. Nonetheless, where we do find significant associations between people’s behaviours and beliefs and their feelings of trust, the role of trust in scientists emerges as particularly important. At the same time, people’s behaviours also seem to be associated with their trust in other bodies, such as local government, which we identified as particularly closely related to people’s reported vaccination status.
Our results also largely confirm that people’s trust in scientists is more closely associated with personalised forms of behaviour (such as vaccination intentions) and support for restrictions around personalised behaviours (such as vaccination passports and compulsory mask-wearing) than with support for more institutionally-oriented measures (such as the mandatory closure of schools). However, we also find associations with people’s trust in scientists for more collective measures such as enforced home-working, where we expected, but did not find, a closer association with people’s trust in government.
These results suggest that trust may often have specific, rather than general, effects. They show that trust might not necessarily matter for all individual behaviours and beliefs, and that it matters more when attached to certain social actors than to others. We therefore need to be cautious before concluding that trust provides a general stimulant for benign social behaviour and beliefs in the context of a health emergency. Instead, the factors shaping those behaviours and beliefs might be more varied and specific.
In identifying these results, we acknowledge the limitations attached to this study. For a start, our data were collected at a single point in time and, as we have been careful to note, our results therefore constitute associations between variables rather than demonstrable causal effects. In addition, our survey indicators capture self-reported actions and attitudes rather than measures of actual behaviour.15 Moreover, the data were collected at a particular point in the coronavirus pandemic’s cycle, and in a single country. As we noted above, empirical studies on the relationship between trust and individual health-related behaviours during the coronavirus pandemic have often produced rather divergent findings. These differences are highly likely to reflect variations in the context and timepoints at which data were gathered. Given this, we would be reluctant to generalise our results to countries outside Britain and to other timepoints. This must await replication studies conducted in other geographical contexts and periods.
5. Conclusion
A key lesson from the coronavirus pandemic that engulfed the world in early 2020 appears to be that, to be effective, agencies tasked with informing and counselling citizens need to command high levels of public trust. This lesson has been recognised by many politicians and officials. For example, in the British case, among the cache of sensitive WhatsApp messages written by former UK Health Secretary, Matt Hancock, and leaked to the British media in spring 2023, was a response from the senior official, Cabinet Secretary Simon Case, who noted the difficulty of encouraging people who had contracted COVID-19 to self-isolate: “We are losing this war because of behaviour—this is the thing we have to turn around (which also probably relies on people hearing about isolation from trusted local figures, not nationally distrusted figures like the PM [Prime Minister, Boris Johnson], sadly)” (The Telegraph 2023).
The results of our study bear out the Cabinet Secretary’s scepticism. People need to hear information and guidance from figures likely to encourage pro-social behaviours and beliefs. Scientific experts are particularly important—reinforcing the central public information role they played during the coronavirus pandemic in many countries, including Britain—although other actors—such as local government—also appear to play an important role. Yet while trust in these actors might help to stimulate popular uptake of vaccination programmes and popular support for some restrictive health measures, they might do less to motivate popular acceptance of other measures like the closure of schools and other public venues. Effective public communication that builds popular support for the kinds of social restrictions seen in Britain and elsewhere during the coronavirus pandemic might profitably include a role for other sources of information and guidance, such as respected educational figures.
In designing strategies that enable national populations to cope with any future health emergency, policy-makers should recognise that, while public trust is an important element in stimulating socially-optimal behaviours and attitudes, people’s evaluations of certain actors appear to be more important than their evaluations of others. Moreover, trust in those actors appears to stimulate some important actions and beliefs more than it does others. In learning the lessons of the coronavirus pandemic, and in planning for any future health emergencies, policy-makers need to move beyond any simplistic assumption that ‘trust matters’, and to understand important conditionalities in the association between people’s trust in different information sources and their behaviours and beliefs.
Supplementary data
Supplementary data is available at Parliamentary Affairs online.
Conflict of interest
The authors report no conflicts of interest.
Data availability
The data analysed in this article are publicly available at the Kent Data Repository (https://doi.org/10.22024/UniKent/01.01.536).
Acknowledgements
A previous version of this paper was presented at the annual conference of the Elections, Public Opinion and Parties (EPOP) group in September 2022. The authors would like to thank the conference participants for their feedback. We would also like to thank the journal reviewers for their helpful comments on an earlier draft of this paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: data collection for this project was funded by the British Academy (grant COVG7210043).
References
Footnotes
For the UK COVID-19 inquiry, see: https://covid19.public-inquiry.uk/.
We formulate this hypothesis notwithstanding the positive association between mask-wearing and trust in government identified by Devine et al. (2024).
The fieldwork period coincided with a downturn in the high-point of COVID-19 cases in Britain, which reached a peak of over 180,000 new daily cases in early January 2022. By the time of the fieldwork, the daily number of new COVID-19 cases had more than halved from this peak, while the daily number of deaths had dropped to under 200. At the same time, just over 70 per cent of the UK population had been fully vaccinated against the coronavirus (Mathieu et al. 2021).
The legal requirement in the UK for people to wear face-masks in shops and other public spaces, to have proof of vaccination to access restaurants and other venues, and to work from home, ended shortly before the start of the survey fieldwork. However, the government continued to urge cautionary behaviour, for example by recommending that individuals wear a face-mask in enclosed or crowded public spaces.
The two items asked respondents to indicate their own position on separate scales asking whether “coronavirus infections should be reduced even if this damages the economy … [or] … the economy should be protected even if this increases coronavirus infections” and “coronavirus infections should be reduced even if this restricts people’s freedoms … [or] … people’s freedoms should be protected even if this increases coronavirus infections”. The wording of these scales was drawn from the British Election Study internet panel (BESIP).
The relevant survey items asked respondents how worried they were “about you, yourself, catching, and becoming seriously ill from COVID-19” and “about the coronavirus situation in the locality where you live …” and, separately, “… in the country as a whole” (the two latter measures were combined into a single scale tapping ‘sociotropic’ fear; α = 0.89). The wording of the personal fear item was based on a question fielded on the BESIP survey.
Items were drawn from various sources, including a Reuters Institute for the Study of Journalism report, and online knowledge quizzes fielded by Johns Hopkins Medicine and The Guardian newspaper.
To check that our reported results are not shaped by this choice of estimation method, we replicated the models predicting people’s coronavirus behaviours and support for coronavirus restrictions using ordinal logit. The results (which are not reported here but are available on request from the first-named author) are substantively similar to those reported in Figs 2 and 4.
In the case of working from home, our sample is significantly smaller than for the other behaviours, since home working was not an option for many survey respondents. Hence, the models predicting home working return coefficients with significantly wider confidence intervals.
We employ Westfall-Young adjustments to the P-values.
In the case of people’s trust in scientists, the generally insignificant associations with individual behaviour are unlikely to reflect changes in the distribution of trust. Our own survey points to high levels of trust in scientists (Fig. 1), while according to Ipsos’ Veracity Index, Britons maintained a high level of trust in scientists over the first two years of the pandemic. In autumn 2019, just before the pandemic’s outbreak, 84% of the British public trusted scientists “to tell the truth”, with an almost identical figure (83%) recorded in autumn 2021, immediately prior to our survey.
Ideally, we would have tested the results for local faith and ethnic leaders specifically among individuals from ethnic minority groups. However, our sample comprised too few such individuals to enable such an analysis.
We can see such commonalities in people’s trust judgements by running a factor analysis of trust in the nine information sources. This exercise suggests a two-dimensional structure to people’s trust judgements (Appendix 4). Trust in central and local government, scientists, local doctors and television news loads onto one dimension (all factor loadings >0.55), while trust in social media and ethnic and faith leaders loads onto a second dimension (all factor loadings >0.83). Only trust in newspapers does not load cleanly onto one of these two dimensions.
When it comes to support for vaccine passports, there is a positive association with trust in television news while, when it comes to support for compulsory mask-wearing and school closures, there are negative associations with trust in local doctors. However, none of the relevant coefficients are that strong, while in tests that adjust for multiple comparisons, they also fall short of statistical significance (P < 0.05).
For example, while at the time of our fieldwork, 92% of our sample reported that they had received at least one COVID-19 vaccination, the actual vaccination rate for the UK population at that point was just over 70% (source: Mathieu et al., 2021).

{kind=link}
{kind=link}
{kind=link}
{kind=link}