





Abstract
Primary hyperparathyroidism is a generalized disorder of bone and mineral metabolism caused by autonomous secretion of parathyroid hormone. It is primarily seen in adults with typical age of presentation between third and fifth decades of life. Juvenile hyperparathyroidism is a rare disorder. The common presentations in order of incidence are fatigue and lethargy, headache, nephrolithiasis, nausea, abdominal pain, vomiting and polydipsia. Though skeletal symptoms include bone pains and fractures, but the presence of limb deformity is atypical. We report a case of young girl who presented with isolated progressive genu valgum of both lower limbs and pigeon-shaped chest deformity. She was found to have hypercalcemia and hypophosphatemia with raised parathyroid hormone levels. The neck imaging showed a single adenoma in the left inferior parathyroid gland. The surgical removal of parathyroid adenoma was performed.
INTRODUCTION
Primary hyperparathyroidism (HPT) is a generalized disorder of bone and mineral metabolism caused by autonomous secretion of parathyroid hormone. The most common cause is parathyroid adenoma followed by parathyroid hyperplasia and rarely carcinoma. It is typically seen in adults between third and fifth decades of life. Juvenile hyperparathyroidism is rare with an incidence rate of ∼2–5 cases per 1 million [1]. The common presentations of juvenile hyperparathyroidism in order of incidence are fatigue and lethargy, headache, nephrolithiasis, nausea, abdominal pain, vomiting and polydipsia. Skeletal manifestations include bone pains and fractures. The presence of limb deformity is atypical and very few cases of genu valgus deformity associated with HPT have been described in the literature. We report a case of 15-year-old girl with HPT whose only presentation was progressive genu valgum of both lower limbs and pigeon-shaped chest deformity.
CASE REPORT
A 15-year-old girl presented with progressive deformity of both lower limbs (bow legs deformity) for 4 years. She also developed proximal muscle weakness in lower limbs and chest deformity (pigeon chest deformity) for 2 years. There was no history of recurrent fractures, polyuria, abdominal pains, recurrent vomiting or constipation. There was no past history of the use of anti-tubercular or anti-epileptic drugs, jaundice or renal problems. There was no family history of frequent fractures, renal calculi, hypertension or multiple endocrine neoplasia (MEN)-related disorders. She had good dietary habit along with adequate milk and sunlight exposure. Physical examination showed bilateral genu valgum deformity (Fig. 1a and b), pectus carinatum and exaggerated lumbar lordosis. No other bony deformities were present. Dentition was normal. Muscle power was medical research council (MRC) grade 4/5 in proximal muscles of lower limbs. The remaining examinations were unremarkable.

Image shows bilateral genu valgum deformity of patient (a) and X-ray lower limbs (b).
Laboratory evaluation showed that a serum level of corrected calcium (normal: 8.8–10.4 mg/dl), phosphate (normal: 3.4–5.8 mg/dl) and alkaline phosphatase (normal: 50–136 IU/l) were 13.2 mg/dl, 2.64 mg/dl and 10 280 IU/l, respectively. Hemogram, liver and renal function tests were normal. Twenty-four-hour urinary calcium was 300 mg/day (normal: 88–300 mg/day). Parathyroid hormone (PTH) and 25-hydroxy vitamin D tests were >2500 (normal: 10–68 pg/ml) and 18 (normal: 15–52 ng/ml), respectively. X-ray of the hand showed subperiosteal resorption of terminal phalanges, multiple bone cysts and generalized osteopenia suggestive of HPT (Fig. 2a and b). The ultrasonography of the neck and (99m) Tc-sestamibi (MIBI) scan showed the presence of a left inferior parathyroid adenoma. Genetic testing to rule MEN syndromes could not be done due to non-availability at our institute. The bilateral neck exploration was done by an experienced surgeon and perioperatively finding correlated with preoperative imaging. The left inferior parathyroid adenoma was resected and biopsy was sent which was consistent with parathyroid adenoma. The intraoperative PTH levels could not be assessed. Her immediate postoperative serum calcium was 9.5 mg/dl and intact parathyroid hormone was 24 pg/ml. The serum calcium fell down to 8 mg/dl in next 2 days following surgery due to transient hypoparathyroidism which was managed accordingly with oral calcium and calcitriol. Her proximal muscle weakness improved and she is in regular follow-up for 3 years.
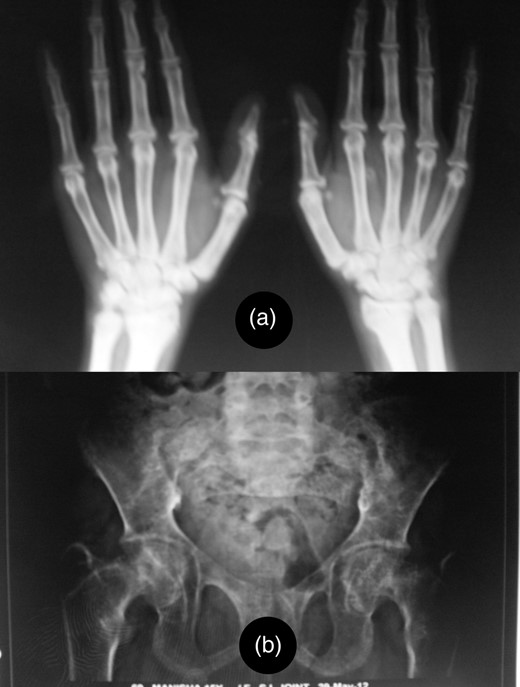
Image shows terminal osteolysis (a) and diffuse osteopenia with multiple bone cysts (b) in X-ray of the hand and pelvis.
DISCUSSION
HPT usually occurs in elderly patients, especially in postmenopausal women. Juvenile HPT is rare. Mostly, it is sporadic and related to isolated single parathyroid adenoma. Familial primary HPT accounts for 5–15% of all cases [2]. In contrast to asymptomatic HPT in adult, children are usually symptomatic with greater morbidity. The presentation can be nonspecific with vague signs and symptoms such as fatigue, anorexia, nausea, vomiting, constipation, irritability or with renal and skeletal manifestation and rarely pancreatitis and peptic ulcer [3]. Osteopenia is an important feature of HPT. Skeletal symptoms include bone pains and fractures. In a case series of 18 patients of juvenile hyperparathyroidism from India, the mean age of presentation was 17 years with female preponderance [4]. The clinical features included bone pain (86.67%), proximal myopathy (46.67%), bony deformities (53.33%), fractures (60%), palpable osteitis fibrosa cystica (33.3%), renal calculi (40%), palpable neck swelling (13.3%) and acute pancreatitis (6.67%). Bilateral genu valgum was seen in five patients. None had a positive family history or features suggestive of MEN. The isolated genu valgus deformity and proximal muscle weakness due to juvenile HPT are rare presentations and very few cases have been described in the literature so far, though genu valgum has been described as one of the skeletal manifestations of HPT in adolescents in multiple case series [5, 6]. The exact mechanism is still not understood. Although our case was found to be vitamin D deficiency, but she did not have other features of rickets. Vitamin D deficiency alone was insufficient to explain the isolated occurrence of genu valgum in hyperparathyroidism in our case, though it can be hypothesized that elevated parathyroid hormone levels may have a direct effect on the growth plates and bone remodeling during pubertal growth spurt resulting in genu valgum [7, 8].
To conclude, juvenile HPT is a rare disorder and raises diagnostic and prognostic problems. In contrast to adult HPT, juvenile HPT are mostly symptomatic and have greater morbidity. Apart from the classical presentation, rare presentation of isolated genu valgus deformity and proximal muscle weakness may occur and such patient should be thoroughly evaluated.
AUTHORS' CONTRIBUTIONS
All the authors contributed to prepare this study.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
No funding support was received for this article.
ETHICAL STANDARD
We have followed the ethical norms and have taken proper informed consent from the patient and relatives. Our patient participated voluntarily and did not suffer any harm. We confirm that all the research meets the ethical guidelines, including adherence to the legal requirements of the study country.
CONSENT
We have obtained written, informed patient consent for publication of the report and any accompanying images.
GUARANTOR
S.K. is a guarantor of this study.

{kind=link}
{kind=link}