






Abstract
Carbapenemase-producing (CP-) carbapenem-resistant Enterobacteriaceae (CRE) have been almost exclusively linked to extensive healthcare exposure and are of significant concern due to limited treatment options and potential for plasmid-mediated spread of resistance. We report on CP-CRE in community-dwelling individuals.
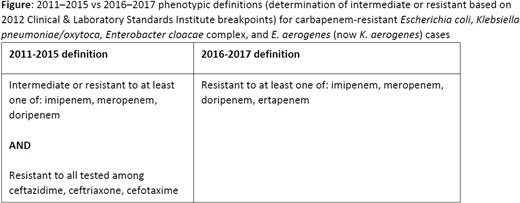
We used 2012–2017 active, laboratory and population-based surveillance data for CRE from CDC’s Emerging Infections Program sites (9 sites by 2017). Cases were the first isolation of Escherichia coli, Klebsiella spp., or Enterobacter spp. from a normally sterile body specimen or urine in a surveillance site resident meeting a CRE phenotype (figure) in a 30 day period. Epidemiologic data were obtained from chart review. Cases were community-associated (CA) if not isolated after the first three days of a hospital stay; without inpatient healthcare, dialysis, or surgery in the year prior; and without indwelling medical devices within two days prior to culture. A convenience sample of isolates was tested at CDC by real-time PCR to detect blaKPC, blaNDM, blaOXA-48-like, blaVIM, or blaIMP.
Of 4023 CRE cases, 699 (17%) were CA, from which 297 isolates were tested; 20 (7%) were CP-CRE, from 18 patients (2 had repeat isolation of the same gene/species). The median age was 68 years (range: 33–91), and 14 (78%) were female. Patients were from 7 sites (range: 1–4/site). Their CP-CRE (10 blaKPC, 6 blaNDM, and 2 blaOXA-48-like) were from three species (10 K. pneumoniae, 6 E. coli, 2 E. cloacae) and isolated from urine (n = 16) and blood (n = 2). Among those with CP-CRE from urine, 12 (75%) had clinical diagnoses of urinary tract infections and the rest had no infection documented. Overall, 7 (39%) were admitted to a hospital within 30 days of culture; none died during hospitalization. Most (n = 13; 72%) had underlying medical comorbidities, most commonly urinary tract abnormalities (n = 5; 28%) and diabetes mellitus (n = 5; 28%). Three (17%) had international travel within two months prior to culture.
CA CP-CRE were found in most surveillance sites but are rare, occurring primarily in older patients with underlying medical conditions. Patient interviews are planned to determine whether CA CP-CRE may be associated with distant or undocumented healthcare exposures.
All authors: No reported disclosures.
Session: 54. HAI: MDRO – GNR Epidemiology, CRE
Thursday, October 3, 2019: 12:15 PM


Comments