






Abstract
Clinical outcomes in patients with severe viral LRTD diagnosed with a bacterial or fungal coinfection
We included adults with a first hospitalization for viral LRTD (2015–2023) based on ICD codes using Optum’s de-identified Clinformatics® Data Mart Database. From this cohort, we identified patients with a bacterial or fungal coinfection using ICD codes. We descriptively analysed patient characteristics in the 12 months pre-hospitalization and clinical outcomes for the first 30 days from hospital admission.
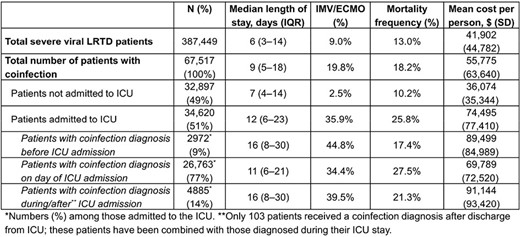
We identified 387,449 patients with severe viral LRTD (75% with coronavirus etiology), of which 67,517 (17%) also had a bacterial/fungal coinfection diagnosis. Mean (SD) age was 73 (14) years in these patients and 54% were women (similar to the overall viral LRTD cohort). Mean (SD) Charlson Comorbidity Index (CCI) was 4 (3), which was slightly higher than in the overall cohort (mean CCI [SD]: 3 [3]). Just over half (51%) had an intensive care unit (ICU) admission (overall cohort: 39%), and among these patients 91% received their coinfection diagnosis while in the ICU (Table). Outcomes including invasive mechanical ventilation (IMV)/extracorporeal membrane oxygenation (ECMO) and death were more frequent in patients with coinfections versus the overall cohort. Among patients receiving IMV/ECMO, 73% received their coinfection diagnosis on the day of the procedure (12% were diagnosed before; 15% were diagnosed after receiving IMV/ECMO). Length of stay was shorter among those diagnosed with a coinfection at ICU admission (vs those diagnosed before ICU admission or during/after an ICU stay). IMV/ECMO frequency was highest in those who were diagnosed with coinfection before their ICU admission; mortality was higher among those diagnosed during their ICU stay.
Patients with viral LRTD and bacterial/fungal coinfection had a higher frequency of severe clinical outcomes compared with the overall viral LRTD cohort, that could not be fully explained by a high ICU admission in this cohort. Coinfection may be an important consideration for high-risk patients even prior to ICU admission.
Susan J. Johnson, PhD, AstraZeneca: Employee|AstraZeneca: Stocks/Bonds (Public Company) Ekaterina Maslova, ScD, AstraZeneca: Employee of AstraZeneca|AstraZeneca: Stocks/Bonds (Private Company) Malin Fageras, PhD, AstraZeneca: Full time employee|AstraZeneca: Stocks/Bonds (Private Company) Gopal Dalal, PhD, AstraZeneca: Advisor/Consultant|AstraZeneca: Employee of ZS Associates India Pvt. Ltd. and contracted to AstraZeneca at time of study Hashmath Ulla T. A. Syed, PhD, AstraZeneca: Advisor/Consultant|AstraZeneca: Employee of ZS Associates India Pvt. Ltd. and contracted to AstraZeneca at time of study Nadir Yehya, MD, AstraZeneca: Advisor/Consultant
Author notes
Study Group:
Session: 65. Respiratory Infections - Viral
Thursday, October 17, 2024: 12:15 PM


{kind=link}
Comments