






Abstract
Increasingly, injection opioid use and opioid use disorder (OUD) are complicated by methamphetamine use, but the impact of stimulant use on the care of people who inject drugs (PWID) with serious injection-related infections (SIRIs) is unknown. The objective of this study was to explore hospital outcomes and postdischarge trends for a cohort of hospitalized PWID to identify opportunities for intervention.
We queried the electronic medical record for patients hospitalized at the University of Alabama at Birmingham with injection drug use–related infections between 1/11/2016 and 4/24/2021. Patients were categorized as having OUD only (OUD), OUD plus methamphetamine use (OUD/meth), or injection of other substance(s) (other). We utilized statistical analyses to assess group differences across hospital outcomes and postdischarge trends. We determined the OUD continuum of care for those with OUD, with and without methamphetamine use.
A total of 370 patients met inclusion criteria—many with readmissions (98%) and high mortality (8%). The majority were White, male, and uninsured, with a median age of 38. One in 4 resided outside of a metropolitan area. There were significant differences according to substance use in terms of sociodemographics and hospital outcomes: patients with OUD/meth were more likely to leave via patient-directed discharge, but those with OUD only had the greatest mortality. Comorbid methamphetamine use did not significantly impact the OUD care continuum.
The current drug crisis in AL will require targeted interventions to engage a young, uninsured population with SIRI in evidence-based addiction and infection services.
The drug epidemic is crippling the United States, with the prevalence of both opioid and stimulant substance use resulting in the highest rates of overdose death and often being associated with severe injection-related infections (SIRIs) [1, 2]. Inpatient care for SIRIs commonly requires an extended stay, and many patients express feeling “stuck” in the hospital, often leading to patient-directed discharge (PDD) before treatment completion [3, 4]. People who inject drugs (PWID) are at heightened risk of PDD from the hospital, which complicates as many as 30% of admissions and leads to higher rates of readmission and mortality postdischarge [5–7].
In our prior work, we found that 14% of PWID were readmitted within 30 days of discharge, and 11% were deceased within 3 years [5]. Other hospitalized cohorts of PWID had similar results, indicating a critical need for improvements in the quality and safety of care for PWID [8–10]. Linkage to medications for opioid use disorder (MOUD) in the hospital setting is feasible and has been shown to reduce readmissions and death, emphasizing the importance of diagnosing and linking patients to MOUD during their hospital stay [9, 11]. Furthermore, almost every step along the opioid use disorder (OUD) care continuum can be supported during hospitalization [11]. Providers and policies in acute care settings can leverage the hospital setting to ensure that patients get and stay in care [12, 13].
An emerging body of literature has identified hospital-based interventions that can improve patient-centered care and reduce PDD and readmission, such as MOUD becoming the standard of care for hospitalized patients with OUD [14, 15]. However, no such pharmacotherapy is approved for treating methamphetamine use disorder, which is increasingly driving overdoses and infections. Concurrent use of opioids and stimulants increases the risk of contracting HIV, hepatitis B, and hepatitis C (HCV) [16]. Methamphetamine use in conjunction with opioids complicates addiction treatment [17–21] and likely increases the complexity of care for patients with SIRI. Methamphetamine use in patients with OUD is associated with lower rates of MOUD treatment, MOUD retention, and opioid abstinence [22]. Yet, there is a dearth of research on hospital outcomes of methamphetamine use in the context of the contemporary drug crisis.
The objective of this study was to explore hospital outcomes and postdischarge trends for a contemporary cohort of hospitalized PWID, with an emphasis on opioids and methamphetamine use, and to determine the OUD Continuum of Care. We focused our analysis on patients who missed opportunities for linkage to evidence-based care with an emphasis on MOUD, but expanded the scope to include methamphetamine due to the high prevalence of polysubstance use with OUD in our contemporary cohort of PWID [23]. We hypothesize that the sociodemographic and clinical outcomes of PWID differ based on their underlying substance use, with methamphetamine use being more common in younger and more racial/ethnic minorities [24]. Further, we anticipate that the OUD continuum, including diagnosis, linkage, and retention in treatment, will vary for those with OUD relative to those with polysubstance use—elucidating opportunities for targeted interventions along the care continuum, based on work by Williams et al. [25].
METHODS
Study Design and Patient Population
This is a retrospective study of hospitalized PWID receiving care at a large academic medical center in the Southeastern United States for an SIRI.
Data Collection and Definition
Retrospective data were queried from the electronic medical record (EMR) for all eligible patients according to the following inclusion criteria: admitted to the University of Alabama at Birmingham (UAB) main hospital campus or UAB Highlands satellite hospital with injection drug use–related infections between 1/11/2016 and 4/24/2021 [11]. We included patients referred to our Intravenous Antibiotic and Addiction Team (IVAT) for an injection-related infection as defined by an electronic order for “IVAT team,” which we have previously described [11]. Injection-related infections were defined as skin and soft tissue infections, bloodstream infections, bone and joint infections, endocarditis, or brain abscesses. Patients were excluded if, upon chart review, there was no evidence of an injection-related bacterial infection.
Baseline demographic information obtained from the EMR included age at admission, race, type of insurance, and location of residence. Residence was categorized using US Department of Agriculture 2010 Rural-Urban Area (RUCA) Codes, categorized as either: Metropolitan (RUCA 1–3), Micropolitan (RUCA 4–6), Small Town (RUCA 7–9), or Rural (RUCA 10) [26]. Insurance type was categorized as “Uninsured,” “Public” (which included Medicaid and Medicare patients), or “Private” (which included commercially insured patients). Length of stay (LOS) was defined in days between date of admission and date of discharge. We also collected data on hospital service utilization (eg, pharmacotherapy, infectious diseases, addiction medicine consult service) and time to service delivery.
Due to the high prevalence of comorbid methamphetamine use disorder and OUD [11], we categorized patients into 1 of 3 groups: “OUD,” indicating that the patient met criteria for an opioid use disorder; “OUD/meth,” indicating that the patient met criteria for OUD and reported methamphetamine use; and “other,” indicating that the participant did not meet criteria for OUD (ie, stimulant only). In some cases, patients were categorized as “other” because they were being treated for an SIRI, with references to injection but no clear documentation of specific substances being injected. A physician reviewed all charts and extracted data on substance use disorder through a review of all primary and addiction medicine consultation notes. In cases of uncertainty, a second physician with expertise in addiction assisted with categorization of specific substance use disorders. The data abstraction focused on patients who met clinical criteria for OUD [27]. Although “OUD” was consistently and frequently documented, documentation on methamphetamine use was varied, with “use,” “disorder,” and “misuse” used interchangeably. Due to the limitations of chart review, we categorized patients with “methamphetamine use” rather than disorder. It is also possible that some groups of OUD or OUD/meth were miscategorized as “other” due to imperfect documentation by physicians and patients underreporting substance use due to stigma. Due to the large percentage of patients who left prematurely, in many instances, documentation was not comprehensive enough to determine specific substance use.
MOUD use was defined as receipt of a Food and Drug Administration (FDA)–approved treatment for OUD including methadone, buprenorphine, or extended-release naltrexone. Using retrospective chart review, we determined whether patients received a medication for OUD during admission and/or at discharge. We evaluated MOUD use for OUD (not pain control only) at any point during hospitalization. We conducted a manual review of each admission and discharge note and pharmacy orders to ensure that data on MOUD dispensing and prescribing were extracted correctly. Time to MOUD was defined in days as time from admission to time of MOUD initiation.
Emergency department (ED) visits and readmissions were defined as both a dichotomous yes/no variable and as frequency of occurrance within 12 months of discharge. Repeat admissions were only included as an outcome. In other words, each participant is only included once in the total sample size, and any duplicate observation (emergency room visit or admission) was included in the outcomes table. We quantified PDD discharge as any person leaving before completion of the discharge process based on absence of standardized discharge documentation completion and/or a discharge note indicating PDD. Outpatient visits were defined as any outpatient infectious disease or addiction clinic visit in the UAB Health system within 12 months of hospital discharge. Data on deaths within 12 months of discharge from any cause were obtained from the EMR and the case management database at the Jefferson County Coroner/Medical Examiner's Office (JCCMEO), the county in which most of the Birmingham metro area resides, from January 2016 to April 2021.
We defined MOUD during admission as patients who received an FDA-approved MOUD during their hospitalization. We defined the second stage of the continuum as having a prescription for MOUD at the time of discharge from the hospital. The final stage was defined as having a recorded outpatient ID or addiction medicine outpatient visit within the UAB health system within 12 months after discharge for SIRI. Care continuum outcomes were sequential, meaning patients would either advance to the next stage or drop off the continuum. For example, patients would not advance on our continuum if they had MOUD at the sentinel visit and an outpatient visit without first having MOUD at discharge.
Statistical Analysis
Preliminary analyses included summarizing the available data using measures of central tendency (sample medians), dispersion (interquartile range), and distribution (frequency, percentage). Missing data were considered missing at random (MAR) and, therefore, not included in descriptive measures or statistical tests. Hypothesis testing (Kruskal-Wallis, Pearson chi-square test; Mantel-Haenszel row mean scores test), evaluated at the .05 significance level, was applied when appropriate statistical assumptions and sample sizes were met. When appropriate, unadjusted post hoc comparisons between OUD alone and OUD/meth use were conducted. All analyses were conducted using SAS software, version 9.4.
RESULTS
A total of 370 PWID receiving hospital-based care for SIRI met inclusion criteria. Among this cohort of PWID, 192 (52%) presented with OUD only, 94 (25%) with OUD/meth, and 84 (23%) other (Table 1). The median age (interquartile range [IQR]) was 38 (31–46) years; most were male (n = 217, 59%), White (n = 326, 88%), seropositive for HCV (n = 98, 60%), and uninsured (n = 160, 44%). Of the 221 (60%) of patients tested for HIV, 5 (2%) were positive (Table 1). Notably, 25% (n = 90) did not reside in a metropolitan area, and 10% (n = 35) reported a rural residence. Further, 41% of patients noted RUCA codes within Jefferson County. Once hospitalized, the median length of stay (IQR) was 14 (7–32) days. During admission, almost all received an addiction medicine consult (n = 357, 97%), but less than half (n = 160, 43%) accessed outpatient services for addiction or infection within 12 months. Many experienced a subsequent ED visit (n = 128, 35%), almost all were readmitted (n = 360, 97%), and 8% (n = 29) died within 12 months (Table 2).
Demographics by OUD Status, Sentinel Admission
| Presentation at Sentinel Visit | |||||
|---|---|---|---|---|---|
| OUD Only (n = 192) | OUD & Meth Use (n = 94) | Other (n = 84) | Overall | OUD Only vs OUD & Meth Usea | |
| Age, y | 38.0 (31.0–46.0) | 36.0 (29.0–41.0) | 41.0 (33.0–51.0) | 0.0024b | 0.0473b |
| Gender, male | 102 (53.1) | 55 (58.5) | 60 (71.4) | 0.0177c | 0.3899c |
| Race | <0.0001c | 0.0371c | |||
| White | 175 (91.1) | 93 (98.9) | 58 (69.0) | ||
| Black or African American | 12 (6.3) | 1 (1.1) | 23 (27.4) | ||
| Other | 5 (2.6) | 0 (0.0) | 3 (3.6) | ||
| Insurance plan type | 0.0029c | 0.0129c | |||
| Uninsured | 79 (41.1) | 56 (59.6) | 25 (30.5) | ||
| Public | 72 (37.5) | 23 (24.5) | 36 (43.9) | ||
| Private | 41 (21.4) | 15 (16.0) | 21 (25.6) | ||
| Missing | 0 | 2 | 2 | ||
| Length of stay, d | 15.5 (7.0–33.5) | 16.5 (7.0–33.0) | 10.5 (6.5–20.5) | 0.1397b | – |
| Rural-Urban Continuum Category | 0.1195d | – | |||
| Metropolitan | 148 (77.5) | 70 (74.5) | 60 (72.3) | ||
| Micropolitan | 16 (8.4) | 11 (11.7) | 14 (16.9) | ||
| Small Town | 7 (3.7) | 2 (2.1) | 5 (6.0) | ||
| Rural | 20 (10.5) | 11 (11.7) | 4 (4.8) | ||
| Missing | 1 | 0 | 1 | ||
| Hepatitis C test result | 0.0631c | – | |||
| Positive | 60 (65.9) | 27 (58.7) | 11 (40.7) | ||
| Negative | 31 (34.1) | 19 (41.3) | 16 (59.3) | ||
| Not tested or NA result | 101 | 48 | 57 | ||
| Meth use indicated, yes | 0 (0.0) | 94 (100.0) | 46 (54.8) | – | – |
| Addiction medicine consultation, yes | 185 (96.4) | 92 (97.9) | 80 (95.2) | 0.6286c | – |
| Time to addiction medicine consultation | 3.0 (1.0–5.0) | 2.0 (1.0–5.0) | 4.0 (2.5–6.0) | 0.0003b | 0.4633b |
| Missing | 7 | 2 | 4 | ||
| Presentation at Sentinel Visit | |||||
|---|---|---|---|---|---|
| OUD Only (n = 192) | OUD & Meth Use (n = 94) | Other (n = 84) | Overall | OUD Only vs OUD & Meth Usea | |
| Age, y | 38.0 (31.0–46.0) | 36.0 (29.0–41.0) | 41.0 (33.0–51.0) | 0.0024b | 0.0473b |
| Gender, male | 102 (53.1) | 55 (58.5) | 60 (71.4) | 0.0177c | 0.3899c |
| Race | <0.0001c | 0.0371c | |||
| White | 175 (91.1) | 93 (98.9) | 58 (69.0) | ||
| Black or African American | 12 (6.3) | 1 (1.1) | 23 (27.4) | ||
| Other | 5 (2.6) | 0 (0.0) | 3 (3.6) | ||
| Insurance plan type | 0.0029c | 0.0129c | |||
| Uninsured | 79 (41.1) | 56 (59.6) | 25 (30.5) | ||
| Public | 72 (37.5) | 23 (24.5) | 36 (43.9) | ||
| Private | 41 (21.4) | 15 (16.0) | 21 (25.6) | ||
| Missing | 0 | 2 | 2 | ||
| Length of stay, d | 15.5 (7.0–33.5) | 16.5 (7.0–33.0) | 10.5 (6.5–20.5) | 0.1397b | – |
| Rural-Urban Continuum Category | 0.1195d | – | |||
| Metropolitan | 148 (77.5) | 70 (74.5) | 60 (72.3) | ||
| Micropolitan | 16 (8.4) | 11 (11.7) | 14 (16.9) | ||
| Small Town | 7 (3.7) | 2 (2.1) | 5 (6.0) | ||
| Rural | 20 (10.5) | 11 (11.7) | 4 (4.8) | ||
| Missing | 1 | 0 | 1 | ||
| Hepatitis C test result | 0.0631c | – | |||
| Positive | 60 (65.9) | 27 (58.7) | 11 (40.7) | ||
| Negative | 31 (34.1) | 19 (41.3) | 16 (59.3) | ||
| Not tested or NA result | 101 | 48 | 57 | ||
| Meth use indicated, yes | 0 (0.0) | 94 (100.0) | 46 (54.8) | – | – |
| Addiction medicine consultation, yes | 185 (96.4) | 92 (97.9) | 80 (95.2) | 0.6286c | – |
| Time to addiction medicine consultation | 3.0 (1.0–5.0) | 2.0 (1.0–5.0) | 4.0 (2.5–6.0) | 0.0003b | 0.4633b |
| Missing | 7 | 2 | 4 | ||
Table statistics are reported as median (IQR) for continuous factors and frequency (column percentage) for categorical factors. Missing data are reported and not included in summary statistics, and column totals may be >100% due to rounding. Bold formatting indicates a significant P value at the .05 level.
Abbreviations: IQR, interquartile range; OUD, opioid use disorder.
Stated statistical tests are unadjusted and compare only those who have indicated OUD at sentinel hospital visit.
Kruskal-Wallis P value.
Pearson chi-square P value.
Mantel-Haenszel row mean scores P value.
Demographics by OUD Status, Sentinel Admission
| Presentation at Sentinel Visit | |||||
|---|---|---|---|---|---|
| OUD Only (n = 192) | OUD & Meth Use (n = 94) | Other (n = 84) | Overall | OUD Only vs OUD & Meth Usea | |
| Age, y | 38.0 (31.0–46.0) | 36.0 (29.0–41.0) | 41.0 (33.0–51.0) | 0.0024b | 0.0473b |
| Gender, male | 102 (53.1) | 55 (58.5) | 60 (71.4) | 0.0177c | 0.3899c |
| Race | <0.0001c | 0.0371c | |||
| White | 175 (91.1) | 93 (98.9) | 58 (69.0) | ||
| Black or African American | 12 (6.3) | 1 (1.1) | 23 (27.4) | ||
| Other | 5 (2.6) | 0 (0.0) | 3 (3.6) | ||
| Insurance plan type | 0.0029c | 0.0129c | |||
| Uninsured | 79 (41.1) | 56 (59.6) | 25 (30.5) | ||
| Public | 72 (37.5) | 23 (24.5) | 36 (43.9) | ||
| Private | 41 (21.4) | 15 (16.0) | 21 (25.6) | ||
| Missing | 0 | 2 | 2 | ||
| Length of stay, d | 15.5 (7.0–33.5) | 16.5 (7.0–33.0) | 10.5 (6.5–20.5) | 0.1397b | – |
| Rural-Urban Continuum Category | 0.1195d | – | |||
| Metropolitan | 148 (77.5) | 70 (74.5) | 60 (72.3) | ||
| Micropolitan | 16 (8.4) | 11 (11.7) | 14 (16.9) | ||
| Small Town | 7 (3.7) | 2 (2.1) | 5 (6.0) | ||
| Rural | 20 (10.5) | 11 (11.7) | 4 (4.8) | ||
| Missing | 1 | 0 | 1 | ||
| Hepatitis C test result | 0.0631c | – | |||
| Positive | 60 (65.9) | 27 (58.7) | 11 (40.7) | ||
| Negative | 31 (34.1) | 19 (41.3) | 16 (59.3) | ||
| Not tested or NA result | 101 | 48 | 57 | ||
| Meth use indicated, yes | 0 (0.0) | 94 (100.0) | 46 (54.8) | – | – |
| Addiction medicine consultation, yes | 185 (96.4) | 92 (97.9) | 80 (95.2) | 0.6286c | – |
| Time to addiction medicine consultation | 3.0 (1.0–5.0) | 2.0 (1.0–5.0) | 4.0 (2.5–6.0) | 0.0003b | 0.4633b |
| Missing | 7 | 2 | 4 | ||
| Presentation at Sentinel Visit | |||||
|---|---|---|---|---|---|
| OUD Only (n = 192) | OUD & Meth Use (n = 94) | Other (n = 84) | Overall | OUD Only vs OUD & Meth Usea | |
| Age, y | 38.0 (31.0–46.0) | 36.0 (29.0–41.0) | 41.0 (33.0–51.0) | 0.0024b | 0.0473b |
| Gender, male | 102 (53.1) | 55 (58.5) | 60 (71.4) | 0.0177c | 0.3899c |
| Race | <0.0001c | 0.0371c | |||
| White | 175 (91.1) | 93 (98.9) | 58 (69.0) | ||
| Black or African American | 12 (6.3) | 1 (1.1) | 23 (27.4) | ||
| Other | 5 (2.6) | 0 (0.0) | 3 (3.6) | ||
| Insurance plan type | 0.0029c | 0.0129c | |||
| Uninsured | 79 (41.1) | 56 (59.6) | 25 (30.5) | ||
| Public | 72 (37.5) | 23 (24.5) | 36 (43.9) | ||
| Private | 41 (21.4) | 15 (16.0) | 21 (25.6) | ||
| Missing | 0 | 2 | 2 | ||
| Length of stay, d | 15.5 (7.0–33.5) | 16.5 (7.0–33.0) | 10.5 (6.5–20.5) | 0.1397b | – |
| Rural-Urban Continuum Category | 0.1195d | – | |||
| Metropolitan | 148 (77.5) | 70 (74.5) | 60 (72.3) | ||
| Micropolitan | 16 (8.4) | 11 (11.7) | 14 (16.9) | ||
| Small Town | 7 (3.7) | 2 (2.1) | 5 (6.0) | ||
| Rural | 20 (10.5) | 11 (11.7) | 4 (4.8) | ||
| Missing | 1 | 0 | 1 | ||
| Hepatitis C test result | 0.0631c | – | |||
| Positive | 60 (65.9) | 27 (58.7) | 11 (40.7) | ||
| Negative | 31 (34.1) | 19 (41.3) | 16 (59.3) | ||
| Not tested or NA result | 101 | 48 | 57 | ||
| Meth use indicated, yes | 0 (0.0) | 94 (100.0) | 46 (54.8) | – | – |
| Addiction medicine consultation, yes | 185 (96.4) | 92 (97.9) | 80 (95.2) | 0.6286c | – |
| Time to addiction medicine consultation | 3.0 (1.0–5.0) | 2.0 (1.0–5.0) | 4.0 (2.5–6.0) | 0.0003b | 0.4633b |
| Missing | 7 | 2 | 4 | ||
Table statistics are reported as median (IQR) for continuous factors and frequency (column percentage) for categorical factors. Missing data are reported and not included in summary statistics, and column totals may be >100% due to rounding. Bold formatting indicates a significant P value at the .05 level.
Abbreviations: IQR, interquartile range; OUD, opioid use disorder.
Stated statistical tests are unadjusted and compare only those who have indicated OUD at sentinel hospital visit.
Kruskal-Wallis P value.
Pearson chi-square P value.
Mantel-Haenszel row mean scores P value.
Patient Outcomes by OUD Status, Sentinel Admission
| Presentation at Sentinel Visit | |||||
|---|---|---|---|---|---|
| OUD Only (n = 192) | OUD & Meth Use (n = 94) | Other (n = 84) | Overall | OUD Only vs OUD & Meth Use | |
| Patient-directed discharge, yes | 35 (18.2) | 22 (23.4) | 6 (7.2) | 0.01411a | 0.3034a |
| Missing | 0 | 0 | 1 | ||
| ED visit within 12 mo after sentinel admission, yes | 65 (33.9) | 33 (35.1) | 30 (35.7) | 0.9494a | – |
| Readmission within 12 mo after sentinel admission, yes | 186 (96.9) | 91 (96.8) | 83 (98.8) | 0.6231a | – |
| Outpatient visit within 12 mo after sentinel admission, yes | 83 (43.2) | 36 (38.3) | 41 (48.8) | 0.3684a | – |
| Death occurs within 12 mo of sentinel admission, yes | 21 (10.9) | 2 (2.1) | 6 (7.1) | 0.0325a | 0.0101a |
| Presentation at Sentinel Visit | |||||
|---|---|---|---|---|---|
| OUD Only (n = 192) | OUD & Meth Use (n = 94) | Other (n = 84) | Overall | OUD Only vs OUD & Meth Use | |
| Patient-directed discharge, yes | 35 (18.2) | 22 (23.4) | 6 (7.2) | 0.01411a | 0.3034a |
| Missing | 0 | 0 | 1 | ||
| ED visit within 12 mo after sentinel admission, yes | 65 (33.9) | 33 (35.1) | 30 (35.7) | 0.9494a | – |
| Readmission within 12 mo after sentinel admission, yes | 186 (96.9) | 91 (96.8) | 83 (98.8) | 0.6231a | – |
| Outpatient visit within 12 mo after sentinel admission, yes | 83 (43.2) | 36 (38.3) | 41 (48.8) | 0.3684a | – |
| Death occurs within 12 mo of sentinel admission, yes | 21 (10.9) | 2 (2.1) | 6 (7.1) | 0.0325a | 0.0101a |
Table statistics are reported as frequency (column percentage) for categorical factors. Missing data are reported and not included in summary statistics. Bold formatting indicates a significant P value at the .05 level.
Abbreviations: ED, emergency department; OUD, opioid use disorder.
Pearson chi-square P value.
Stated statistical tests are unadjusted and compare only those who have indicated OUD at sentinel hospital visit.
Patient Outcomes by OUD Status, Sentinel Admission
| Presentation at Sentinel Visit | |||||
|---|---|---|---|---|---|
| OUD Only (n = 192) | OUD & Meth Use (n = 94) | Other (n = 84) | Overall | OUD Only vs OUD & Meth Use | |
| Patient-directed discharge, yes | 35 (18.2) | 22 (23.4) | 6 (7.2) | 0.01411a | 0.3034a |
| Missing | 0 | 0 | 1 | ||
| ED visit within 12 mo after sentinel admission, yes | 65 (33.9) | 33 (35.1) | 30 (35.7) | 0.9494a | – |
| Readmission within 12 mo after sentinel admission, yes | 186 (96.9) | 91 (96.8) | 83 (98.8) | 0.6231a | – |
| Outpatient visit within 12 mo after sentinel admission, yes | 83 (43.2) | 36 (38.3) | 41 (48.8) | 0.3684a | – |
| Death occurs within 12 mo of sentinel admission, yes | 21 (10.9) | 2 (2.1) | 6 (7.1) | 0.0325a | 0.0101a |
| Presentation at Sentinel Visit | |||||
|---|---|---|---|---|---|
| OUD Only (n = 192) | OUD & Meth Use (n = 94) | Other (n = 84) | Overall | OUD Only vs OUD & Meth Use | |
| Patient-directed discharge, yes | 35 (18.2) | 22 (23.4) | 6 (7.2) | 0.01411a | 0.3034a |
| Missing | 0 | 0 | 1 | ||
| ED visit within 12 mo after sentinel admission, yes | 65 (33.9) | 33 (35.1) | 30 (35.7) | 0.9494a | – |
| Readmission within 12 mo after sentinel admission, yes | 186 (96.9) | 91 (96.8) | 83 (98.8) | 0.6231a | – |
| Outpatient visit within 12 mo after sentinel admission, yes | 83 (43.2) | 36 (38.3) | 41 (48.8) | 0.3684a | – |
| Death occurs within 12 mo of sentinel admission, yes | 21 (10.9) | 2 (2.1) | 6 (7.1) | 0.0325a | 0.0101a |
Table statistics are reported as frequency (column percentage) for categorical factors. Missing data are reported and not included in summary statistics. Bold formatting indicates a significant P value at the .05 level.
Abbreviations: ED, emergency department; OUD, opioid use disorder.
Pearson chi-square P value.
Stated statistical tests are unadjusted and compare only those who have indicated OUD at sentinel hospital visit.
We identified several differences in the sociodemographics of this population based on substance use across the 3 groups (Table 1). When comparing the median ages of patients across each group, individuals in the OUD/meth group were younger when compared with the OUD-only and other groups (P = .002). There were more men in the other group compared with the other 2 groups (P = .018). More individuals in the OUD/meth group were White (P = .037) and uninsured (P = .003) as compared with the other 2 groups.
We compared hospital and postdischarge outcomes across OUD status groups (Table 2). Overall, the rate of PDD significantly differed by substance use (P = .014), as those without OUD were less likely to have a PDD (7.2%) than others: Of OUD only, 18.2% experienced PDD, and of OUD/meth, 23.4% experienced PDD. Although PDD was high among those with OUD and OUD/meth, this association was not significant (P = .303). The OUD/meth group had the lowest rate of death within 12 months of admission (2%) among OUD status groups (P = .033), while the group without OUD had a marginally higher percentage of deaths (7%). The OUD-only group had the highest observed deaths 12 months following hospitalization (n = 21, 11%). The statistical significance of the association between death within 12 months and OUD without methamphetamine use is consistent when comparing OUD-specific groups (P = .010).
For patients with OUD overall (OUD only and OUD/meth), progress across the OUD care continuum steadily decreased at each stage: 53% (n = 152) received MOUD during admission, and 38% (n = 108) received MOUD at discharge. After discharge, retention in the OUD care continuum dropped, with only 5% (n = 14) of patients attending an outpatient visit in the health system. There were no significant differences in care continuum outcomes for patients with OUD vs OUD/meth.
DISCUSSION
This study of 370 patients receiving inpatient care for SIRI elucidates the characteristics, needs, and outcomes of an understudied group of PWID in the Southeastern United States. We identified a largely White, uninsured population of PWID with prevalent polysubstance use who required prolonged, resource-intensive, and frequent hospital care. During admission, almost all PWID received an addiction medicine consult, but less than half accessed outpatient services for addiction or infection within 12 months. Of those eligible, less than half received MOUD on discharge. Unfortunately, many experienced a subsequent ED visit, almost all were readmitted, and a relatively small yet significant group (9%) died within 12 months of hospital discharge.
Consistent with our hypothesis, we found some statistically significant differences by substance used: When compared with those with OUD only, PWID who use opioids and methamphetamine (OUD/meth) were younger, more likely to be uninsured, and more likely to be White. The fact that they are young and uninsured suggests that, if they continue with drug use, related complications like SIRI will be very resource-intensive over the course of their lives, especially in states like Alabama, with no Medicaid expansion. Furthermore, the size of this subset with OUD/meth use, representing 38% of all study participants, is concerning, as methamphetamine has been associated with infectious disease risk, morbidity, and mortality [18, 28, 29]. And yet, there are no FDA-approved pharmacotherapies for this substance use disorder.
Several additional differences between those with OUD only and OUD/meth did not meet statistical significance but suggest unique challenges: This subset with comorbid methamphetamine use received a more rapid addiction medicine consult (average of 2 days) relative to the OUD-only group, likely due to the severity of their addiction, withdrawal, or a shorter time to diagnosis of substance use. However, this earlier access to consultation did not translate to higher rates of MOUD use. This group was also more likely to leave prematurely, a metric associated with poor outcomes [11]. Perhaps this is related to more severe withdrawal, cravings, and/or stigma from providers and staff—factors known to contribute to PDD [4, 30]. Despite this higher rate of PDD, which abbreviates admissions, the overall length of stay in the OUD/meth group was longer (16.5 vs 15.5 days) when compared with the OUD-only group. While these differences did not reach statistical significance (Table 1), these findings suggest an emerging demographic at risk for poor hospital outcomes, which requires further study.
Surprisingly, mortality was higher in the OUD-only group. Because of the limitations of death data documented in medical records, we do not have access to cause of death for all patients. Hence, we cannot comment on the percentage of overdose deaths vs other fatal events. There are few data on differences in all-cause mortality in those who use methamphetamines relative to others, which makes this study unique. The existing literature on death in this subset (OUD/meth) focuses on overdose outcomes alone. For example, previous research suggests that individuals who use stimulants are more likely to overdose [31]. One prior Centers for Disease Control and Prevention report of opioid-related deaths in 2018 found that 63% of these co-occurred with at least 1 other substance [17]. Furthermore, the simultaneous injection of both heroin and methamphetamine has been linked to a ∼3-fold increase in reported overdose. It is important to note that, due to contamination of street drugs, people who use drugs rarely have control of the content of their drug supply, and therefore drug use and overdose may be unrelated to preference or drug of choice (opioids vs stimulants). Regardless, further study of all-cause mortality, including infection-related mortality and overdose, in those with OUD vs OUD/meth will allow us to identify relative risks and opportunities for intervention in those who use these substances.
Of all PWID in our study, 25% resided outside of a metropolitan area, which has significant implications for health care access and community-based care. Furthermore, 1 in 10 reported a rural residence. Rural and micropolitan counties have fewer resources such as infectious diseases and/or addiction providers and rehabilitation facilities, which necessitates a long commute to more urban medical centers [32]. These counties often lack robust emergency medical services to distribute life-saving interventions, such as naloxone [32]. Due to a lack of Medicaid expansion in Alabama, hospitals face financial hurdles when trying to care for their inpatients and safely transition them to outpatient settings [33, 34]. Any efforts to improve the OUD care continuum must account for rural geography, transportation challenges, and lack of insurance.
There were no significant differences in the OUD care continuum for PWID with OUD, regardless of methamphetamine use. Just over half with OUD received MOUD during admission, and fewer received MOUD on discharge. In our previous research, we identified many reasons that patients may not receive MOUD on admission including, most commonly, lack of addiction medicine consultation, provider perception that MOUD is not indicated, and patient disinterest [11]. We found additional reasons that MOUD was not prescribed on discharge: premature discharge, disinterest in MOUD, and acute indication for prescription opioids (pain control) [11].
Surprisingly, a notable percentage across all groups attended an outpatient infectious disease or addiction clinic visit (38%–48%) (Table 2), which may be related to inpatient social services that provide patients with scheduling assistance and arrange transportation for hospital follow-up appointments when needed. Alternatively, this could be due to the severe nature of SIRIs, which motivated patients to attend clinic appointments to ensure treatment response. This high rate of attendance highlights another touch point for addiction care, such as MOUD: hospital follow-up appointments. Unfortunately, only 5% attended an outpatient visit in the year following discharge and achieved the more proximal OUD continuum metrics (ie, MOUD during admission, on discharge) (Figure 1). In other words, only 5% received evidence-based OUD care across the outpatient treatment settings. We believe this gap is due to a lack of community-based services for PWID after discharge. For patients without community support, social services and case management often disappear after hospital discharge, and future appointments may become impossible to attend without scheduling assistance, appointment reminders, and transportation support. Lastly, the OUD continuum is not a perfect fit for all patients because not all patients will require long-term MOUD; some patients enter recovery or maintain OUD remission without clinical services or treatment. In these cases, a more appropriate model may emphasize remission as the primary outcome [12].
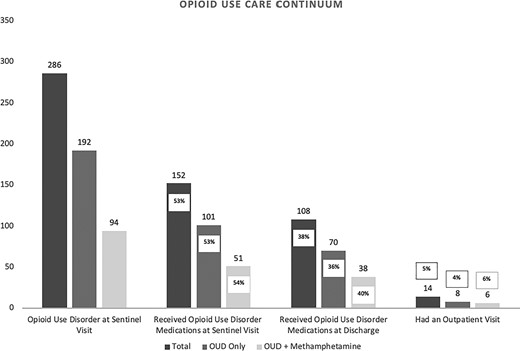
OUD care continuum. Abbreviation: OUD, opioid use disorder.
Given the large number of participants who were discharged without MOUD, there must be an opportunity for this group to later receive treatment, ideally before they experience another complication and admission. Telehealth is one promising modality that can help expand addiction services via remote administration of addiction treatment [35]. Telehealth also has the potential to extend addiction services into rural and poor regions where many of our SIRI patients reside postdischarge [36]. For example, if a patient is not ready to enter recovery during their inpatient stay, having the option to utilize telehealth postdischarge and begin MOUDs when they are ready is invaluable. As the COVID-19 pandemic resulted in increased barriers to care for PWID, it is more critical than ever to consider these remote methods to keep PWID safe and engaged in services after hospitalizations [37].
There are several important limitations to our study mostly due to underreporting or missing data. First, due to underreporting of both injection and substance use, we may have excluded some eligible participants who remain undiagnosed [20–24]. The study period (2016 to 2021) includes the COVID-19 pandemic, a time in which PWID experienced additional barriers to care. For this reason, PWID may have presented with more advanced infections and/or addiction. Data on substance use were dependent on patient report and provider documentation, which may have led some to be miscategorized as “other.” Area of residence was taken from each patient’s medical record and may not represent the patient’s true place of residency (eg, jail, shelter, rehabilitation facility). Data were limited to those deaths reported to county coroners, JCCMEO, and documented in the EMR. We anticipate that this is an underrepresentation of overall deaths as not all deaths are reported and identified, and many deaths may occur outside of our jurisdiction, making it unlikely that they were captured in our available databases. To this issue, roughly 59% of patients reported RUCA codes outside of Jefferson County.
The UAB emergency department aims to screen all patients for HIV and HCV per universal screening protocol; however, if the patient is severely ill, left via PDD, or is transferred from an outside hospital, they may not receive HIV and HCV testing. Additionally, ED visit data are only reflective of UAB ED data excluding visits at community hospitals. Similarly, any patient who had an outpatient follow-up visit outside the UAB health system (ie, community health clinic) would not be included in the continuum as having a follow-up visit. However, because Alabama has not expanded Medicaid and because of the complex nature of SIRI infections, we believe that most of these very sick and often uninsured patients who receive care receive it most often at UAB clinics, which are accessible regardless of insurance status. Further, general medicine clinicians at UAB and in Alabama do not routinely prescribe MOUD or treatment for addiction, infectious disease, or HIV services [38]. Therefore, general medicine visits postdischarge were not included in the care continuum.
In closing, we anticipate more young and uninsured patients presenting with polysubstance use who will benefit from tailored interventions to accommodate increasingly complex SIRI cases. Gaps in both hospital and community-based care of OUD leave patients untreated and vulnerable to subsequent infection and overdose. To improve health for PWID, communities must develop innovative, low-barrier interventions to facilitate the transitions from hospitals back to community settings.
Acknowledgments
Financial support. This work was supported by the University of Alabama at Birmingham (UAB) Center for AIDS Research (CFAR), an NIH-funded program (P30 AI027767)
Author contributions. Sera Levy conceptualized the project, conducted literature searches, and contributed to writing and preparing the manuscript for publication; John Bassler contributed to conceptualization of the project, conducted analysis and interpretation of the data, and contributed to writing and preparing the manuscript for publication; Kelly Gagnon contributed to conceptualization of the project and to writing and preparing the manuscript for publication; Myles Prados contributed to conceptualization of the project, conducted manual chart reviews to determine opioid use disorder status, and contributed to writing and preparing the manuscript for publication; Madison Jeziorski contributed to conceptualization of the project, conducted literature searches, and contributed to writing and preparing the manuscript for publication; Brandi McClesky contributed to conceptualization of the project, collected death data from the Jefferson County Coroner/Medical Examiner's Office, and contributed to writing and preparing the manuscript for publication; Kaylee Crockett contributed to conceptualization of the project and contributed to writing and preparing the manuscript for publication; Li Li contributed to conceptualization of the project and contributed to writing and preparing the manuscript for publication; Davis Bradford contributed to conceptualization of the project and contributed to writing and preparing the manuscript for publication; Karen Cropsey contributed to conceptualization of the project and contributed to writing and preparing the manuscript for publication; Ellen Eaton served as primary faculty mentor for the project, conceptualized the project, assisted with analysis and interpretation of the data, and contributed to writing and preparing the manuscript for publication.
Patient consent. This study does not include factors necessitating patient consent according to the UAB Institutional Review Board.
References
American Psychiatric
Author notes
Potential conflicts of interest. All authors: no reported conflicts of interest.


{kind=link}
Comments