





Abstract
Evidence is still scarce regarding the use of e-cigarettes by young people for weight-control reasons. This study aimed to test a model in which the prospective association between negative body esteem and e-cigarette use is mediated by weight-control outcome expectancies for e-cigarette use. The model was tested across genders.
Data were collected at three time points, 6 months apart, from 2327 young adults (mean age = 21.2; SD = 2.2; 54% women). Self-reported data were collected on demographics, body mass index, body esteem, weight-control outcome expectancies for e-cigarette use, and current e-cigarette use and cigarette smoking.
Among women, we found a significant indirect effect of lower body esteem on higher likelihood of current e-cigarette use 1 year later, mediated by higher weight-control outcome expectancies at 6-month follow-up, adjusting for demographics, body mass index, and baseline e-cigarette use and cigarette smoking. Among men, body esteem was not found to have significant effect on either weight-control expectancies or e-cigarette use.
Based on the current findings, young adult women who have higher negative body esteem are at increased risk for using e-cigarettes for weight-control motives.
The current findings are some of the first to show prospective associations among weight-control motives and e-cigarette use among young adults. These findings suggest that a group of vulnerable young women may be using e-cigarettes to lose or control weight. More research is needed to understand their choice of flavors, nicotine concentration, and device type. In addition, research is needed to understand whether e-cigarettes are being marketed, directly or indirectly, as being useful for weight loss or control. There may be a need for health promotion strategies that provide healthier alternatives to young women struggling with low body esteem who use e-cigarettes for weight loss or control.
Introduction
Between 2017 and 2018, e-cigarette use rates increased 78% (from 11.7% to 20.8%) among U.S. high school students.1 Among adults 18 and over, young adults (18–25 year olds) show the highest prevalence of current e-cigarette use in the United States.2 Approximately 15% of current e-cigarette users are likely to report having never smoked a cigarette.1 To develop strategies to prevent misuse of e-cigarette use among young people, understanding why they use e-cigarettes is important. Several studies have examined e-cigarette use motives and outcome expectancies among youths and adults.3–6 Outcome expectancies are beliefs that certain outcomes are expected if one engages in a behavior. Outcome expectancies underlie motives and are part of several cognitive models of substance use etiology.7–9 The assumption is that positive outcomes associated with a behavior encourage the behavior, whereas negative outcomes discourage the behavior. For example, positive outcome expectancies for cigarette smoking, such as positive (e.g., stimulation, pleasure) or negative reinforcement (e.g., stress reduction) beliefs associated with cigarette smoking, have been found to predict dependence and cessation among adult smokers10–12 as well as initiation and escalation among young adults.13–15 There is robust evidence demonstrating associations between weight concerns, weight-control outcome expectancies and higher cigarette smoking, cigarette use initiation, and reduced smoking cessation, particularly among women.16–19
Furthermore, research on cigarette smoking suggests that women struggling with low body esteem or negative body image are more likely to smoke cigarettes for weight-control purposes.20–22 Body image may be defined as a person’s perception of his or her own body and the resulting feelings: positive, negative, or neutral.23 Body esteem is a closely related concept and may be defined as the amount of self-esteem a person derives from the perceived physical condition and/or attractiveness of his or her body. That is, individuals who are dissatisfied with their body image or physical condition are likely to have lower body esteem.24,25 However, body esteem may be gender specific, dependent on different factors for men and women.25 For example, even though perceived physical condition may be an indicator of body esteem for both men and women, weight concerns may preponderate for women while upper body strength may do so for men.25
As for e-cigarettes, studies show that positive outcome expectancies, such as social enhancement, affect regulation, and positive sensory experience are associated with higher use among current users and increased use susceptibility among never users.3,4 At present, however, little is known about weight control outcome expectancies for e-cigarette use among young people. Recent research suggests that weight-control motives may influence e-cigarette use as well.26–28 Approximately 15% of current e-cigarette users, including young adult users, appear to report weight control or weight loss as a motive for e-cigarette use.28,29 Bloom et al.30 found that among adult cigarette smokers, those who scored higher on “smoking to suppress appetite” and “smoking to prevent overeating” motives were also likely to use e-cigarettes. Another study, with young adults, found higher weight concerns to be associated with higher e-cigarette use frequency.31 As with cigarette smoking, women are likely to endorse weight control as a motive for e-cigarette use than men.32 Some preliminary evidence suggests that low body esteem may also be a risk factor for e-cigarette use.28
Clearly, more research is needed to understand the relationships among body esteem, weight-control outcome expectancies, and e-cigarette use. Such knowledge may inform efforts to control e-cigarette misuse among never or former smokers, or promote smoking cessation among smokers who smoke to control weight or fear quitting because of fear of gaining weight. At present, the evidence that weight-control e-cigarette use expectancies are predictive of higher e-cigarette use among youth and young adults is scant and relatively weak. Most such research is cross-sectional. Moreover, such research has not examined antecedents of weight-control expectancies such as perceived body image or esteem.
To address these current gaps in the literature, the present study tested the hypothesis that, among young adults, weight-control outcome expectancies for e-cigarette use would mediate the association between low body esteem at baseline and current e-cigarette use a year later. The assumption underlying our hypothesis is that those with lower body esteem are likely to report higher weight-control outcome expectancies, which in turn would predict higher likelihood of current e-cigarette use. The hypothesis was tested separately for men and women, using three waves of data, each separated from the subsequent wave by 6 months.
Methods
Procedures
Participants were recruited from two 4-year and four 2-year (community) colleges on Oahu, HI. All institutions belonged to the same University system. E-mail addresses were obtained for all 18–25 year olds enrolled across campuses. Invitation to participate in the screener survey was sent to randomly selected e-mail addresses. The link to the screener survey was accompanied by an invitation text, which described the study in generic terms, as a study on marketing and young adult health behavior. The screener survey asked questions about age, sex, tobacco, alcohol, and dietary behaviors. The screener survey also asked students for their contact information, including phone number.
Students were given on average two weeks of time to respond to the screener survey and provided up to three reminders. Approximately 60% of those who were sent the invitation, completed the screener survey. This response rate is similar to or higher than rates reported for other studies33,34 recruiting young adults from colleges through e-mail invitations. However, those who responded to the e-mail invitations were predominantly women who had never smoked a cigarette. In order to obtain a sample that was more gender balanced as well as included proportions of cigarette smokers and experimenters comparable to or higher than the national distribution of smokers in the 18–25 years age group, we supplemented the e-mail recruitment with classroom-based recruitment. We randomly selected on average 40 classes from each participating campus and presented the study in those classrooms. Students approached in the classrooms completed the paper-and-pencil version of the screener survey. The average response rate across classrooms was 80%.
Across the e-mail and classroom methods, a total of 3664 were screened to be eligible to participate in the study and were invited to participate in the study. Figure 1 shows flow of sample sizes through recruitment and data collection procedures. Participants provided written consent to participate in the longitudinal study and were sent a unique link to the baseline survey via e-mail. The baseline participants were contacted 6 and 12 months later to complete 6-month and 1-year follow-up surveys. The 1-year follow-rate was 89%. Both the baseline and follow-up surveys were programmed on Inquisit.35
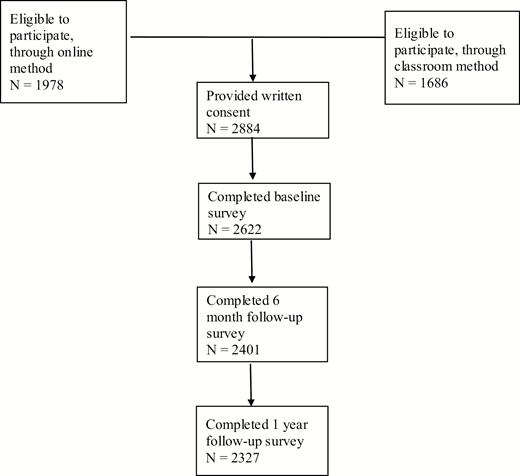
Flowchart showing sample sizes across three waves of data collection.
Measures
Demographics
Demographic information was collected on self-reported age, ethnicity, sex, parental income, height, and weight. Each participant’s body mass index (BMI) was calculated based on their self-reported height and weight.
Body Esteem
Body esteem was assessed using the Body Esteem Scale (BES).25 BES was designed for use among young adults, both men and women, and has been validated among college students.25 The scale represents multiple dimensions that differ for men and women.32 These factors include “physical attractiveness” for men or “sexual attractiveness” for women; “upper body strength” for men or “weight concern” for women; and “physical condition” for both men and women. The present study employed 19 out of the original 35 BES items. The 19 items were selected to include all items pertaining to the “physical condition” and “weight concern/upper body strength” factors. In the interest of saving survey space, we excluded “sexual attractiveness” items, which included the majority of “physical attractiveness” items for men.
Among women, the 19 items represented weight concern (nine items; α = 0.89) and physical condition (10 items; α = 0.92) factors. Among men, 13 items (α = 0.93) represented physical condition, 3 items (α = 0.86) represented upper body strength, and 2 items (α = 0.73) represented physical attractiveness. The items represented a list of body parts (e.g., waist, stomach, legs, hips, buttocks, biceps, thigh) or characteristics (e.g., weight, agility, figure or physique, body build, physical coordination, energy level). Participants were instructed to indicate how they felt about each with regard to their own body (5-point scale; “Have strong negative feelings” to “Have strong positive feelings”). The scores were reversed for analysis purposes in the current study.
E-cigarette Weight-Control Outcome Expectancies
A list of statements representing potential outcomes of e-cigarette use was provided, and participants were asked to indicate on a scale from 0 to 9 the likelihood that each outcome would occur to them if they were to use an e-cigarette. Three items (α = 0.79) were used to measure weight-control outcome expectancies. The three items (e.g., “Lose weight,” “Control appetite”) are additions to a self-report inventory of e-cigarette use outcome expectancies.3,4
E-cigarette Use and Cigarette Smoking
Current e-cigarette use and cigarette smoking were assessed in terms of past 30-day use: participants indicated their frequency of use in the past 30 days (7-point scale; “0 days,” 1–2 days,” “3–5 days”…“All 30 days”).
Data Analyses
Data were analyzed among 2327 participants who participated in all three waves of data collection. To determine whether the longitudinal sample differed from the baseline sample due to attrition, we compared the longitudinal sample with the baseline sample on key study variables. The mediation hypothesis was tested using structural equation modeling in Mplus.36 A measurement model was estimated for body esteem as a latent variable with weight concern and physical condition as indicators for women, and upper body strength, physical attractiveness, and physical condition as indicators for men. In addition, weight-control expectancies for e-cigarette use was estimated as a latent variable. Because the measurement model for body esteem differed between genders, a separate model was estimated for each gender, instead of conducting a multigroup analysis on the same configural model. Missing data were imputed by Mplus using the missing at random maximum likelihood estimation.
Across genders, weight-control outcome expectancies at 6-month follow-up were specified as the mediator. Baseline body esteem, BMI, age, family/household income, ethnicity (dummy coded as Asian, Filipino, Native/Hawaiian/Other Pacific Islander, and Other, relative to White), and college type (2 years vs. 4 years) were specified as exogenous variables. Past-30-day e-cigarette use and cigarette smoking at baseline were also specified as exogenous variables. Past-30-day e-cigarette use at 1-year follow-up was specified as the criterion variable.
All exogenous variables were specified to correlate with each other. For each gender, the model was set up by specifying direct paths from all exogenous variables to the mediator variable and the criterion variable, and from the mediator variable to the criterion variable. Then the model was estimated across genders using the Weighted Least Square Mean and Variance (WLSMV) Adjusted estimator (past-30-day cigarette and e-cigarette use were treated as ordinal variables). The final model was estimated by including only those regression paths that were statistically significant for one or both genders. Indirect effects were estimated in Mplus, which uses multivariate delta method to compute standard errors of the indirect effects.37,38
Results
Participants
Table 1 shows the characteristics of the one-year prospective sample (N = 2327) across genders. Women were more likely to represent Whites and those who reported their family/household income to be less than $39 000/year. Women tended to report higher average BMI. Men were more likely to be enrolled in 2-year colleges and report past-30-day e-cigarette use. There were no gender differences in cigarette smoking. The longitudinal sample was not found to differ statistically significantly from the baseline sample (N = 2622) on any of the variables considered in the present study.
Participant Characteristics for the Longitudinal Sample (N = 2327)
| Men | Women | Range | |||
|---|---|---|---|---|---|
| Mean (SD) | Frequency | Mean (SD) | Frequency | ||
| Age | 21.1 (2.2) | 21.2 (2.1) | 18–25 | ||
| Ethnicity* | |||||
| White | 22% | 27% | |||
| Asian | 30% | 24% | |||
| Filipino | 19% | 19% | |||
| Native Hawaiian/Pacific Islander | 21% | 19% | |||
| Other | 9% | 12% | |||
| Family income | |||||
| 0–39 999 | 20% | 24% | |||
| 40 000–79 999 | 33% | 34% | |||
| 80 000–119 999 | 27% | 25% | |||
| 120 000–159 999 | 12% | 9% | |||
| 160 000 or over | 8% | 8% | |||
| T1 body mass index* | 25.2 (5.6) | 24.6 (6.0) | 15–61 | ||
| College type* | |||||
| 4 y | 46% | 67% | |||
| 2 y | 54% | 33% | |||
| T2 E-cig weight control expectancies | 4.8 (6.4) | 4.8 (6.3) | 0–27 | ||
| T1 Poor body esteem | |||||
| Physical condition | 34.7 (11.1) | 32.7 (9.6) | 11–65 | ||
| Weight concerns | 26.3 (7.9) | 5–45 | |||
| Physical appearance | 5.5 (1.9) | 2–15 | |||
| Upper body strength | 8.3 (3.2) | 2–10 | |||
| T1 past-30-day e-cigarette use*** | 27% | 17% | |||
| T3 past-30-day e-cigarette use*** | 28% | 21% | |||
| T1 past-30-day cigarette smoking | 18% | 18% | |||
| T3 past-30-day cigarette smoking | 15% | 15% |
| Men | Women | Range | |||
|---|---|---|---|---|---|
| Mean (SD) | Frequency | Mean (SD) | Frequency | ||
| Age | 21.1 (2.2) | 21.2 (2.1) | 18–25 | ||
| Ethnicity* | |||||
| White | 22% | 27% | |||
| Asian | 30% | 24% | |||
| Filipino | 19% | 19% | |||
| Native Hawaiian/Pacific Islander | 21% | 19% | |||
| Other | 9% | 12% | |||
| Family income | |||||
| 0–39 999 | 20% | 24% | |||
| 40 000–79 999 | 33% | 34% | |||
| 80 000–119 999 | 27% | 25% | |||
| 120 000–159 999 | 12% | 9% | |||
| 160 000 or over | 8% | 8% | |||
| T1 body mass index* | 25.2 (5.6) | 24.6 (6.0) | 15–61 | ||
| College type* | |||||
| 4 y | 46% | 67% | |||
| 2 y | 54% | 33% | |||
| T2 E-cig weight control expectancies | 4.8 (6.4) | 4.8 (6.3) | 0–27 | ||
| T1 Poor body esteem | |||||
| Physical condition | 34.7 (11.1) | 32.7 (9.6) | 11–65 | ||
| Weight concerns | 26.3 (7.9) | 5–45 | |||
| Physical appearance | 5.5 (1.9) | 2–15 | |||
| Upper body strength | 8.3 (3.2) | 2–10 | |||
| T1 past-30-day e-cigarette use*** | 27% | 17% | |||
| T3 past-30-day e-cigarette use*** | 28% | 21% | |||
| T1 past-30-day cigarette smoking | 18% | 18% | |||
| T3 past-30-day cigarette smoking | 15% | 15% |
T1 = baseline; T2 = 6-month follow-up; T3 = 1-y follow-up.
*p < .05; **p < .01; ***p < .001.
Participant Characteristics for the Longitudinal Sample (N = 2327)
| Men | Women | Range | |||
|---|---|---|---|---|---|
| Mean (SD) | Frequency | Mean (SD) | Frequency | ||
| Age | 21.1 (2.2) | 21.2 (2.1) | 18–25 | ||
| Ethnicity* | |||||
| White | 22% | 27% | |||
| Asian | 30% | 24% | |||
| Filipino | 19% | 19% | |||
| Native Hawaiian/Pacific Islander | 21% | 19% | |||
| Other | 9% | 12% | |||
| Family income | |||||
| 0–39 999 | 20% | 24% | |||
| 40 000–79 999 | 33% | 34% | |||
| 80 000–119 999 | 27% | 25% | |||
| 120 000–159 999 | 12% | 9% | |||
| 160 000 or over | 8% | 8% | |||
| T1 body mass index* | 25.2 (5.6) | 24.6 (6.0) | 15–61 | ||
| College type* | |||||
| 4 y | 46% | 67% | |||
| 2 y | 54% | 33% | |||
| T2 E-cig weight control expectancies | 4.8 (6.4) | 4.8 (6.3) | 0–27 | ||
| T1 Poor body esteem | |||||
| Physical condition | 34.7 (11.1) | 32.7 (9.6) | 11–65 | ||
| Weight concerns | 26.3 (7.9) | 5–45 | |||
| Physical appearance | 5.5 (1.9) | 2–15 | |||
| Upper body strength | 8.3 (3.2) | 2–10 | |||
| T1 past-30-day e-cigarette use*** | 27% | 17% | |||
| T3 past-30-day e-cigarette use*** | 28% | 21% | |||
| T1 past-30-day cigarette smoking | 18% | 18% | |||
| T3 past-30-day cigarette smoking | 15% | 15% |
| Men | Women | Range | |||
|---|---|---|---|---|---|
| Mean (SD) | Frequency | Mean (SD) | Frequency | ||
| Age | 21.1 (2.2) | 21.2 (2.1) | 18–25 | ||
| Ethnicity* | |||||
| White | 22% | 27% | |||
| Asian | 30% | 24% | |||
| Filipino | 19% | 19% | |||
| Native Hawaiian/Pacific Islander | 21% | 19% | |||
| Other | 9% | 12% | |||
| Family income | |||||
| 0–39 999 | 20% | 24% | |||
| 40 000–79 999 | 33% | 34% | |||
| 80 000–119 999 | 27% | 25% | |||
| 120 000–159 999 | 12% | 9% | |||
| 160 000 or over | 8% | 8% | |||
| T1 body mass index* | 25.2 (5.6) | 24.6 (6.0) | 15–61 | ||
| College type* | |||||
| 4 y | 46% | 67% | |||
| 2 y | 54% | 33% | |||
| T2 E-cig weight control expectancies | 4.8 (6.4) | 4.8 (6.3) | 0–27 | ||
| T1 Poor body esteem | |||||
| Physical condition | 34.7 (11.1) | 32.7 (9.6) | 11–65 | ||
| Weight concerns | 26.3 (7.9) | 5–45 | |||
| Physical appearance | 5.5 (1.9) | 2–15 | |||
| Upper body strength | 8.3 (3.2) | 2–10 | |||
| T1 past-30-day e-cigarette use*** | 27% | 17% | |||
| T3 past-30-day e-cigarette use*** | 28% | 21% | |||
| T1 past-30-day cigarette smoking | 18% | 18% | |||
| T3 past-30-day cigarette smoking | 15% | 15% |
T1 = baseline; T2 = 6-month follow-up; T3 = 1-y follow-up.
*p < .05; **p < .01; ***p < .001.
Zero-Order Correlations
Tables 2 and 3 show the zero-order correlations between key study variables among men and women, respectively. For men, none of the body esteem indicators—that is, physical condition, upper body strength, or physical attractiveness—were significantly associated with weight-control outcome expectancies, or cigarette or e-cigarette use at any time-point. However, higher weight-control outcome expectancies correlated with higher cigarette and e-cigarette use. Native Hawaiian/Pacific Islander ethnicity was positively correlated with BMI. BMI was not correlated with cigarette or e-cigarette use.
Zero-Order Correlations Among Key Study Variables for Men (n = 1040)
| AGE | A | F | NH | O | INCM | PC | PA | UBS | T2 WT EXP | T1 BMI | T1 CIG | T3 CIG | T1 ECIG | T3 ECIG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1 | ||||||||||||||
| A | −.06* | 1 | |||||||||||||
| F | −.06* | −.33*** | 1 | ||||||||||||
| NH | −.02 | −.21*** | −.25*** | 1 | |||||||||||
| O | .05 | −.02 | −.15*** | −.17*** | 1 | ||||||||||
| INCM | .05 | −05 | −.10** | −.09** | −.01 | 1 | |||||||||
| T1 PC | −.02 | .05 | .09** | −.004 | −.07* | −.08* | 1 | ||||||||
| T1 PA | .01 | .05 | .07 | −.04 | −.04 | −.07* | .72*** | 1 | |||||||
| T1 UBS | −.03 | .04 | .06 | .02 | −.03 | −.06 | .77*** | .63*** | 1 | ||||||
| T2 WT EXP | .04 | −.01 | .02 | .03 | −.02 | −.08* | .04 | .03 | .01 | 1 | |||||
| T1 BMI | .07 | −.13*** | .04 | .18*** | .01 | −.08* | .26*** | .13** | .05 | .03 | 1 | ||||
| T1 CIG | .19*** | −.04 | −.05 | .01 | .01 | .03 | .01 | −.005 | −.006 | .14*** | .03 | 1 | |||
| T3 CIG | .15*** | −.02 | −.04 | .05 | −.03 | −.02 | .01 | −.008 | −.004 | .08** | .02 | .59*** | 1 | ||
| T1 ECIG | .02 | −.01 | .04 | .07 | −.04 | −.04 | .03 | .017 | −.01 | .19*** | .03 | .25*** | .14*** | 1 | |
| T3 ECIG | .03 | −.002 | .02 | .08 | −.04 | −.01 | .05 | .02 | .006 | .16*** | .02 | .24*** | .20*** | .64*** | 1 |
| AGE | A | F | NH | O | INCM | PC | PA | UBS | T2 WT EXP | T1 BMI | T1 CIG | T3 CIG | T1 ECIG | T3 ECIG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1 | ||||||||||||||
| A | −.06* | 1 | |||||||||||||
| F | −.06* | −.33*** | 1 | ||||||||||||
| NH | −.02 | −.21*** | −.25*** | 1 | |||||||||||
| O | .05 | −.02 | −.15*** | −.17*** | 1 | ||||||||||
| INCM | .05 | −05 | −.10** | −.09** | −.01 | 1 | |||||||||
| T1 PC | −.02 | .05 | .09** | −.004 | −.07* | −.08* | 1 | ||||||||
| T1 PA | .01 | .05 | .07 | −.04 | −.04 | −.07* | .72*** | 1 | |||||||
| T1 UBS | −.03 | .04 | .06 | .02 | −.03 | −.06 | .77*** | .63*** | 1 | ||||||
| T2 WT EXP | .04 | −.01 | .02 | .03 | −.02 | −.08* | .04 | .03 | .01 | 1 | |||||
| T1 BMI | .07 | −.13*** | .04 | .18*** | .01 | −.08* | .26*** | .13** | .05 | .03 | 1 | ||||
| T1 CIG | .19*** | −.04 | −.05 | .01 | .01 | .03 | .01 | −.005 | −.006 | .14*** | .03 | 1 | |||
| T3 CIG | .15*** | −.02 | −.04 | .05 | −.03 | −.02 | .01 | −.008 | −.004 | .08** | .02 | .59*** | 1 | ||
| T1 ECIG | .02 | −.01 | .04 | .07 | −.04 | −.04 | .03 | .017 | −.01 | .19*** | .03 | .25*** | .14*** | 1 | |
| T3 ECIG | .03 | −.002 | .02 | .08 | −.04 | −.01 | .05 | .02 | .006 | .16*** | .02 | .24*** | .20*** | .64*** | 1 |
A = Asian; F = Filipino; NH = Native Hawaiian; O = other; INCM = family income; PC = baseline physical condition (body esteem); PA = baseline physical attractiveness (body esteem); UBS = baseline upper body strength; T2 WT EXP = e-cigarette use weight-control outcome expectancies at T2 (i.e., 6-month follow-up); T1 BMI = baseline body mass index; T1 CIG = baseline past-30-day cigarette smoking; T1 ECIG = baseline past-30-day e-cigarette use; T3 ECIG = past-30-day e-cigarette use at 1-y follow-up.
*p < .05, **p < .01, ***p < .001.
Zero-Order Correlations Among Key Study Variables for Men (n = 1040)
| AGE | A | F | NH | O | INCM | PC | PA | UBS | T2 WT EXP | T1 BMI | T1 CIG | T3 CIG | T1 ECIG | T3 ECIG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1 | ||||||||||||||
| A | −.06* | 1 | |||||||||||||
| F | −.06* | −.33*** | 1 | ||||||||||||
| NH | −.02 | −.21*** | −.25*** | 1 | |||||||||||
| O | .05 | −.02 | −.15*** | −.17*** | 1 | ||||||||||
| INCM | .05 | −05 | −.10** | −.09** | −.01 | 1 | |||||||||
| T1 PC | −.02 | .05 | .09** | −.004 | −.07* | −.08* | 1 | ||||||||
| T1 PA | .01 | .05 | .07 | −.04 | −.04 | −.07* | .72*** | 1 | |||||||
| T1 UBS | −.03 | .04 | .06 | .02 | −.03 | −.06 | .77*** | .63*** | 1 | ||||||
| T2 WT EXP | .04 | −.01 | .02 | .03 | −.02 | −.08* | .04 | .03 | .01 | 1 | |||||
| T1 BMI | .07 | −.13*** | .04 | .18*** | .01 | −.08* | .26*** | .13** | .05 | .03 | 1 | ||||
| T1 CIG | .19*** | −.04 | −.05 | .01 | .01 | .03 | .01 | −.005 | −.006 | .14*** | .03 | 1 | |||
| T3 CIG | .15*** | −.02 | −.04 | .05 | −.03 | −.02 | .01 | −.008 | −.004 | .08** | .02 | .59*** | 1 | ||
| T1 ECIG | .02 | −.01 | .04 | .07 | −.04 | −.04 | .03 | .017 | −.01 | .19*** | .03 | .25*** | .14*** | 1 | |
| T3 ECIG | .03 | −.002 | .02 | .08 | −.04 | −.01 | .05 | .02 | .006 | .16*** | .02 | .24*** | .20*** | .64*** | 1 |
| AGE | A | F | NH | O | INCM | PC | PA | UBS | T2 WT EXP | T1 BMI | T1 CIG | T3 CIG | T1 ECIG | T3 ECIG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1 | ||||||||||||||
| A | −.06* | 1 | |||||||||||||
| F | −.06* | −.33*** | 1 | ||||||||||||
| NH | −.02 | −.21*** | −.25*** | 1 | |||||||||||
| O | .05 | −.02 | −.15*** | −.17*** | 1 | ||||||||||
| INCM | .05 | −05 | −.10** | −.09** | −.01 | 1 | |||||||||
| T1 PC | −.02 | .05 | .09** | −.004 | −.07* | −.08* | 1 | ||||||||
| T1 PA | .01 | .05 | .07 | −.04 | −.04 | −.07* | .72*** | 1 | |||||||
| T1 UBS | −.03 | .04 | .06 | .02 | −.03 | −.06 | .77*** | .63*** | 1 | ||||||
| T2 WT EXP | .04 | −.01 | .02 | .03 | −.02 | −.08* | .04 | .03 | .01 | 1 | |||||
| T1 BMI | .07 | −.13*** | .04 | .18*** | .01 | −.08* | .26*** | .13** | .05 | .03 | 1 | ||||
| T1 CIG | .19*** | −.04 | −.05 | .01 | .01 | .03 | .01 | −.005 | −.006 | .14*** | .03 | 1 | |||
| T3 CIG | .15*** | −.02 | −.04 | .05 | −.03 | −.02 | .01 | −.008 | −.004 | .08** | .02 | .59*** | 1 | ||
| T1 ECIG | .02 | −.01 | .04 | .07 | −.04 | −.04 | .03 | .017 | −.01 | .19*** | .03 | .25*** | .14*** | 1 | |
| T3 ECIG | .03 | −.002 | .02 | .08 | −.04 | −.01 | .05 | .02 | .006 | .16*** | .02 | .24*** | .20*** | .64*** | 1 |
A = Asian; F = Filipino; NH = Native Hawaiian; O = other; INCM = family income; PC = baseline physical condition (body esteem); PA = baseline physical attractiveness (body esteem); UBS = baseline upper body strength; T2 WT EXP = e-cigarette use weight-control outcome expectancies at T2 (i.e., 6-month follow-up); T1 BMI = baseline body mass index; T1 CIG = baseline past-30-day cigarette smoking; T1 ECIG = baseline past-30-day e-cigarette use; T3 ECIG = past-30-day e-cigarette use at 1-y follow-up.
*p < .05, **p < .01, ***p < .001.
Zero-Order Correlations Among Key Study Variables for Women (n = 1282).
| AGE | A | F | NH | O | INCM | PC | WC | T2 WT EXP | T1 BMI | T1 CIG | T3 CIG | T1 ECIG | T3 ECIG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1 | |||||||||||||
| A | −.04 | 1 | ||||||||||||
| F | −.01 | −.27*** | 1 | |||||||||||
| NH | .04 | −.27*** | −.23*** | 1 | ||||||||||
| O | −.01 | −.20*** | −.17*** | −.18*** | 1 | |||||||||
| INCM | −.06* | −.01 | −.03 | −.08** | −.06* | 1 | ||||||||
| PC | .01 | .04 | −.01 | .05 | −.08** | −.06* | 1 | |||||||
| WC | −.01 | .11 | −.01 | .04 | −.07* | −.08** | .74*** | 1 | ||||||
| T2 WT EXP | .01 | −.05 | −.002 | −.05 | .05 | .04 | .14*** | .11** | 1 | |||||
| T1 BMI | .16*** | −.13 | .02 | .20*** | −.002 | −.12*** | .33*** | .23*** | .03 | 1 | ||||
| T1 CIG | .19*** | −.01 | −.05 | .08* | −.04 | −.008 | .09** | .12*** | .10** | .12** | 1 | |||
| T3 CIG | .15*** | −.05 | −.04 | .08** | −.05 | .05 | .08** | .10** | .07* | .09** | .70*** | 1 | ||
| T1 ECIG | .02 | −.04 | .05 | .02 | −.06* | −.03 | .03 | .11** | .14*** | .02 | .26*** | .15*** | 1 | |
| T3 ECIG | .0002 | .01 | .03 | .05 | −.03 | −.03 | .06* | .09** | .12*** | .03 | .27*** | .18*** | .54*** | 1 |
| AGE | A | F | NH | O | INCM | PC | WC | T2 WT EXP | T1 BMI | T1 CIG | T3 CIG | T1 ECIG | T3 ECIG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1 | |||||||||||||
| A | −.04 | 1 | ||||||||||||
| F | −.01 | −.27*** | 1 | |||||||||||
| NH | .04 | −.27*** | −.23*** | 1 | ||||||||||
| O | −.01 | −.20*** | −.17*** | −.18*** | 1 | |||||||||
| INCM | −.06* | −.01 | −.03 | −.08** | −.06* | 1 | ||||||||
| PC | .01 | .04 | −.01 | .05 | −.08** | −.06* | 1 | |||||||
| WC | −.01 | .11 | −.01 | .04 | −.07* | −.08** | .74*** | 1 | ||||||
| T2 WT EXP | .01 | −.05 | −.002 | −.05 | .05 | .04 | .14*** | .11** | 1 | |||||
| T1 BMI | .16*** | −.13 | .02 | .20*** | −.002 | −.12*** | .33*** | .23*** | .03 | 1 | ||||
| T1 CIG | .19*** | −.01 | −.05 | .08* | −.04 | −.008 | .09** | .12*** | .10** | .12** | 1 | |||
| T3 CIG | .15*** | −.05 | −.04 | .08** | −.05 | .05 | .08** | .10** | .07* | .09** | .70*** | 1 | ||
| T1 ECIG | .02 | −.04 | .05 | .02 | −.06* | −.03 | .03 | .11** | .14*** | .02 | .26*** | .15*** | 1 | |
| T3 ECIG | .0002 | .01 | .03 | .05 | −.03 | −.03 | .06* | .09** | .12*** | .03 | .27*** | .18*** | .54*** | 1 |
A = Asian; F = Filipino; NH = Native Hawaiian; O = other; INCM = family income; PC = baseline physical condition (body esteem); WC = baseline weight concerns (body esteem); T2 WT EXP = e-cigarette use weight-control outcome expectancies at T2 (i.e., 6-month follow-up); T1 BMI = baseline body mass index; T1 CIG = Bbaseline past-30-day cigarette smoking; T1 ECIG = baseline past-30-day e-cigarette use; T3 ECIG = past-30-day e-cigarette use at 1-y follow-up.
*p < .05, **p < .01, ***p < .001.
Zero-Order Correlations Among Key Study Variables for Women (n = 1282).
| AGE | A | F | NH | O | INCM | PC | WC | T2 WT EXP | T1 BMI | T1 CIG | T3 CIG | T1 ECIG | T3 ECIG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1 | |||||||||||||
| A | −.04 | 1 | ||||||||||||
| F | −.01 | −.27*** | 1 | |||||||||||
| NH | .04 | −.27*** | −.23*** | 1 | ||||||||||
| O | −.01 | −.20*** | −.17*** | −.18*** | 1 | |||||||||
| INCM | −.06* | −.01 | −.03 | −.08** | −.06* | 1 | ||||||||
| PC | .01 | .04 | −.01 | .05 | −.08** | −.06* | 1 | |||||||
| WC | −.01 | .11 | −.01 | .04 | −.07* | −.08** | .74*** | 1 | ||||||
| T2 WT EXP | .01 | −.05 | −.002 | −.05 | .05 | .04 | .14*** | .11** | 1 | |||||
| T1 BMI | .16*** | −.13 | .02 | .20*** | −.002 | −.12*** | .33*** | .23*** | .03 | 1 | ||||
| T1 CIG | .19*** | −.01 | −.05 | .08* | −.04 | −.008 | .09** | .12*** | .10** | .12** | 1 | |||
| T3 CIG | .15*** | −.05 | −.04 | .08** | −.05 | .05 | .08** | .10** | .07* | .09** | .70*** | 1 | ||
| T1 ECIG | .02 | −.04 | .05 | .02 | −.06* | −.03 | .03 | .11** | .14*** | .02 | .26*** | .15*** | 1 | |
| T3 ECIG | .0002 | .01 | .03 | .05 | −.03 | −.03 | .06* | .09** | .12*** | .03 | .27*** | .18*** | .54*** | 1 |
| AGE | A | F | NH | O | INCM | PC | WC | T2 WT EXP | T1 BMI | T1 CIG | T3 CIG | T1 ECIG | T3 ECIG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AGE | 1 | |||||||||||||
| A | −.04 | 1 | ||||||||||||
| F | −.01 | −.27*** | 1 | |||||||||||
| NH | .04 | −.27*** | −.23*** | 1 | ||||||||||
| O | −.01 | −.20*** | −.17*** | −.18*** | 1 | |||||||||
| INCM | −.06* | −.01 | −.03 | −.08** | −.06* | 1 | ||||||||
| PC | .01 | .04 | −.01 | .05 | −.08** | −.06* | 1 | |||||||
| WC | −.01 | .11 | −.01 | .04 | −.07* | −.08** | .74*** | 1 | ||||||
| T2 WT EXP | .01 | −.05 | −.002 | −.05 | .05 | .04 | .14*** | .11** | 1 | |||||
| T1 BMI | .16*** | −.13 | .02 | .20*** | −.002 | −.12*** | .33*** | .23*** | .03 | 1 | ||||
| T1 CIG | .19*** | −.01 | −.05 | .08* | −.04 | −.008 | .09** | .12*** | .10** | .12** | 1 | |||
| T3 CIG | .15*** | −.05 | −.04 | .08** | −.05 | .05 | .08** | .10** | .07* | .09** | .70*** | 1 | ||
| T1 ECIG | .02 | −.04 | .05 | .02 | −.06* | −.03 | .03 | .11** | .14*** | .02 | .26*** | .15*** | 1 | |
| T3 ECIG | .0002 | .01 | .03 | .05 | −.03 | −.03 | .06* | .09** | .12*** | .03 | .27*** | .18*** | .54*** | 1 |
A = Asian; F = Filipino; NH = Native Hawaiian; O = other; INCM = family income; PC = baseline physical condition (body esteem); WC = baseline weight concerns (body esteem); T2 WT EXP = e-cigarette use weight-control outcome expectancies at T2 (i.e., 6-month follow-up); T1 BMI = baseline body mass index; T1 CIG = Bbaseline past-30-day cigarette smoking; T1 ECIG = baseline past-30-day e-cigarette use; T3 ECIG = past-30-day e-cigarette use at 1-y follow-up.
*p < .05, **p < .01, ***p < .001.
Among women, lower perceived physical condition was correlated with higher BMI, higher weight-control outcome expectancies, and higher cigarette smoking. Similarly, higher weight concern was correlated with higher BMI, higher weight-control outcome expectancies, and higher cigarette smoking and e-cigarette use. Native Hawaiian/Pacific Islander ethnicity was positively correlated with BMI, and BMI was positively correlated with higher cigarette smoking.
Structural Equation Model
Figures 2 and 3 show the results of the structural equation models testing the proposed mediational hypothesis for men and women, respectively. For men, the model presented in Figure 1 fit well to the data (χ 2 = 152, df = 80, p < .0001; root mean square error of approximation = 0.03 [90% confidence interval = 0.02–0.04; confirmatory fit index = 0.94]). Among men, we did not find direct or indirect effects of baseline body esteem on past-30-day e-cigarette use 1 year later. However, a significant association was found between weight-control outcome expectancies at 6-month follow-up and e-cigarette use at 1-year follow-up. Baseline cigarette and e-cigarette use had significant effects on higher weight-control expectancies at 6-month follow-up and higher cigarette and e-cigarette use at 1-year follow-up.
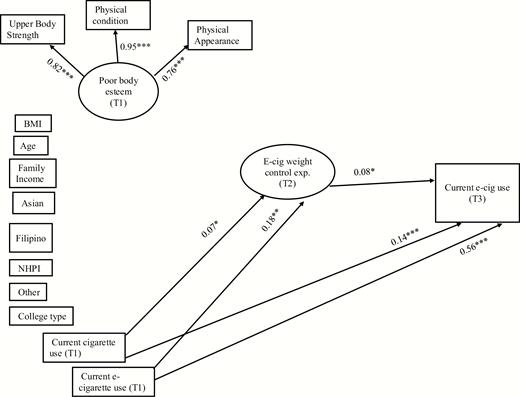
Structural equation model showing the associations among poor body esteem at baseline (T1), weight-control outcome expectancies for e-cigarette use at 6-month follow-up (T2), and past-30-day e-cigarette use at 1-year follow-up among men (T3; N = 1040). BMI = body mass index; NHPI = Native Hawaii/Pacific Islander; college type = 4-year or 2-year college. Ethnicity (Asian, Filipino, NHPI, and Other) were dummy coded with reference to White. Circles represent latent variables, and rectangles represent manifest variables. Indicators for weight-control expectancies are not shown for simplicity. Straight arrows represent regression paths. Numbers represent standardized path coefficients. Only statistically significant paths are shown. Correlations between exogenous variables were included in the analysis but are not shown in the figure. ***p < .001, **p < .01, *p < .05.
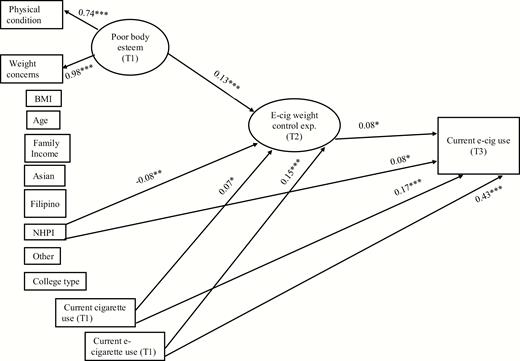
Structural equation model showing the associations among poor body esteem at baseline (T1), weight-control outcome expectancies for e-cigarette use at 6-month follow-up (T2), and past-30-day e-cigarette use at 1-year follow-up among women (T3; N = 1282). BMI = body mass index; NHPI = Native Hawaii/Pacific Islander; college type = 4-year or 2-year college. Ethnicity (Asian, Filipino, NHPI, and other) were dummy coded with reference to White. Circles represent latent variables, and rectangles represent manifest variables. Indicators for weight-control expectancies are not shown for simplicity. Straight arrows represent regression paths. Numbers represent standardized path coefficients. Only statistically significant paths are shown. Correlations between exogenous variables were included in the analysis but are not shown in the figure. ***p < .001, **p < .01, *p < .05.
The model for women fit reasonably well to the data (χ 2 = 193, df = 70, p < .0001; root mean square error of approximation = 0.035 [90% confidence interval = 0.03–0.04; confirmatory fit index = 0.91]). Low body esteem was found to have significant indirect effect on higher e-cigarette use via higher weight-control outcome expectancies for e-cigarette use (indirect effect = 0.01 [SE = 0.005]; p < .05). A direct path was found from Native Hawaiian/Pacific Islander status to higher e-cigarette use a year later. In addition, we found significant paths from baseline cigarette and e-cigarette use to weight-control outcome expectancies 6 months later and e-cigarette use 1 year later.
Discussion
The present study examined weight-control outcome expectancies for e-cigarette use as a mediator of the prospective effects of negative body esteem on current e-cigarette use among young adults. The mediation hypothesis was tested for men and women separately. We found a significant indirect effect of positive body esteem on lower current e-cigarette use 1 year later among women, but not among men. However, among men, there was a significant direct path from weight-control expectancies to follow-up e-cigarette use. These findings are novel and important in several regards.
This may be the first study to prospectively demonstrate that weight-control outcome expectancies are a unique predictor of e-cigarette use among young adults. Our findings further suggest that young adults struggling with negative body esteem may be particularly vulnerable to using e-cigarettes for weight-control motives. The current findings are particularly strong as evidence because our model accounted for the potential demographic confounders, including BMI, and adjusted for the effects of baseline cigarette smoking and e-cigarette use. Past several studies have found body image dissatisfaction to be associated with higher cigarette smoking among girls and young women.39–41 However, this is the first study to show that negative body esteem may also lead to increased e-cigarette use. The prospective effect of cigarette smoking on e-cigarette use is not surprising, as e-cigarettes are considered as an alternative to cigarettes and regular e-cigarette users are often dual users of e-cigarettes and cigarettes.42 Because e-cigarettes are perceived as being less harmful than cigarettes,43 women smoking cigarettes to lose weight or control appetite may switch over to using e-cigarettes or use e-cigarettes to reduce smoking.
The lack of association between negative body esteem and future e-cigarette use among men may be explained in terms of how body esteem is manifested for men versus women. Note that based on the BES, the body parts and functions represented within “weight concern” among women are indicative of “physical attractiveness” and “upper body strength” among men.32 As Franzoi and Shields32 have argued, gender differences in body esteem is, to a great extent, shaped by differences in social norms about what is considered “beautiful” or “attractive” for men and women. For example, a slim body may be perceived as attractive for women whereas a muscular body may be considered attractive for men. As a result, losing weight may be more important for women’s body esteem and gaining muscles may be more important for men’s body esteem. Thus, this may be a reason why body esteem is associated with weight-control outcome expectancies for e-cigarette use among women but not men. We, however, found that higher weight-control outcome expectancies were a predictor of higher e-cigarette use among men as well.
The current findings draw attention to women struggling with body esteem as a vulnerable group potentially at high risk for e-cigarette use. In addition, the research highlights that weight-control outcome expectancies are likely to be strong predictors of e-cigarette for both men and women. Hence, more research is needed to understand how young adults using e-cigarettes in terms of choice of devices, flavors, and nicotine concentrations. Such knowledge would help understand how e-cigarettes are being used for weight control and provide an insight into the level of risk. Research is also needed to understand whether e-cigarette marketing is, directly or indirectly, propagating the message that e-cigarette use leads to weight control. There is evidence suggesting that e-cigarette companies are actively patenting e-cigarette-based technologies for weight loss.44
The current findings also draw attention to the need to understand whether e-cigarette use does indeed help young adults reduce or maintain weight. If yes, then e-cigarettes may be increasingly adopted by cigarette smokers, presumably women smokers, who have difficulty quitting cigarettes because of fear of weight gain.45 Future research may need to examine the positive and negative consequences of switching to e-cigarettes by cigarette smokers to maintain weight.
There are some limitations to this study. First, the current sample included 18–25 year olds; hence, the findings may not generalize to adolescents or older adults. Second, the present study used self-report data, which always leaves room for unintentional and intentional error in participant reporting. Third, 11% of the baseline participants were lost to follow-up, which may have introduced some bias into the sample. Fourth, we did not assess dietary intakes; thus, we have no information regarding energy intake or diet quality. Last, the present study did not use the body esteem scale in its original entirety. This may have limited the breadth of our findings.
Despite the limitations, the present study is significant for demonstrating the roles of body esteem and weight-control expectancies in influencing e-cigarette use behavior among young adults. The present findings have implications for prevention programs. As the scientific community focuses on developing evidence-based e-cigarette use prevention programs, it is crucial to understand why and how young people are using e-cigarettes. The present study stresses the need to address factors such as body esteem and weight-control outcome expectancies in such programs. For example, the programs may help young people correct misperceptions about e-cigarette use outcomes or help them find alternative, healthier strategies for weight control. In summary, based on prospective data, the study provides strong evidence that young adult women with negative body esteem may be at risk for using e-cigarettes for weight-control motives.
Funding
This research was supported by grants from the National Cancer Institute, National Institutes of Health, USA (R01CA202277 and R01CA228905).
Declaration of Interests
The authors have no conflict to declare.
References

{kind=link}
{kind=link}
{kind=link}
Comments