




Abstract
The risks of breast cancer in African American (AA) women associated with inherited mutations in breast cancer predisposition genes are not well defined. Thus, whether multigene germline hereditary cancer testing panels are applicable to this population is unknown. We assessed associations between mutations in panel-based genes and breast cancer risk in 5054 AA women with breast cancer and 4993 unaffected AA women drawn from 10 epidemiologic studies.
Germline DNA samples were sequenced for mutations in 23 cancer predisposition genes using a QIAseq multiplex amplicon panel. Prevalence of mutations and odds ratios (ORs) for associations with breast cancer risk were estimated with adjustment for study design, age, and family history of breast cancer.
Pathogenic mutations were identified in 10.3% of women with estrogen receptor (ER)-negative breast cancer, 5.2% of women with ER-positive breast cancer, and 2.3% of unaffected women. Mutations in BRCA1, BRCA2, and PALB2 were associated with high risks of breast cancer (OR = 47.55, 95% confidence interval [CI] = 10.43 to >100; OR = 7.25, 95% CI = 4.07 to 14.12; OR = 8.54, 95% CI = 3.67 to 24.95, respectively). RAD51D mutations were associated with high risk of ER-negative disease (OR = 7.82, 95% CI = 1.61 to 57.42). Moderate risks were observed for CHEK2, ATM, ERCC3, and FANCC mutations with ER-positive cancer, and RECQL mutations with all breast cancer.
The study identifies genes that predispose to breast cancer in the AA population, demonstrates the validity of current breast cancer testing panels for use in AA women, and provides a basis for increased referral of AA patients for cancer genetic testing.
In recent years, there have been notable advances in knowledge of both prevalence and penetrance of germline inactivating mutations in genes that are associated with a moderate (relative risk 2–4) or high (relative risk >4) risk of breast cancer (1,2). In addition to BRCA1 and BRCA2 (3), at least 10 other genes [ATM (4,5), BARD1 (6,7), CDH1 (8), CHEK2 (9), NF1 (10), PALB2 (11,12), PTEN (13), RAD51C (14), RAD51D (15), and TP53 (16)] have been associated with moderate or high risk of breast cancer in women of European ancestry (EA). This information has been used to inform cancer risk management such as prophylactic surgery or enhanced screening and is increasingly being used to guide targeted treatments.
However, limited data are available from women of African ancestry, including from African American (AA) women, who have a higher incidence of breast cancer at young ages, a higher incidence of estrogen receptor (ER)-negative breast cancer, and a 42% higher breast cancer mortality rate than non-Hispanic white women (17,18). A recent study of African ancestry women reported relative risks for BRCA1 and BRCA2 only (19). Stable estimates of the prevalence of pathogenic mutations in AA women and the magnitude of associations between mutations and breast cancer risk are not available, despite being critical for informing appropriate recommendations for genetic testing and for counseling on preventive strategies. To fill these critical gaps, we assembled 5054 AA women with breast cancer and 4993 unaffected AA women from 10 epidemiologic studies and conducted uniform targeted multigene panel testing.
Methods
Study Sample
Participants were drawn from 5 prospective cohort studies, 3 case-control studies, 1 case-cohort study, and 1 case-only study (see Table 1; Supplementary Table 1, available online). The Northern California Breast Cancer Family Registry (27) preferentially selected women with a family history of breast cancer and the Black Women: Etiology and Survival of TNBC study (26) and the University of California Irvine Breast Cancer Study (28) preferentially selected women with breast cancer at young ages. Participants in all other studies were unselected with regard to family history or young age at diagnosis. For the cohort studies, 1 to 2 unaffected AA women were selected from among all unaffected women at the time of case patient diagnosis, matched to case patients on age. Most biospecimen samples in the cohort studies (83%) were obtained either before breast cancer diagnosis or less than a year after diagnosis. An additional study, the NIEHS Sister Study (31), which enrolled women who had a sister with breast cancer, contributed data only to stratified analyses restricted to women with a family history of breast cancer. Further descriptions of the studies are given in Supplementary Materials, including Supplementary Table 1 (available online). Institutional review boards at the Mayo Clinic and all contributing sites approved the research. All participants provided written informed consent.
Characteristics of study participants by breast cancer status*
| Participant characteristics | Affected (n = 5054) No. (%) | Unaffected (n = 4993) No. (%) |
|---|---|---|
| Age in years, mean (SD) | 54.4 (12.0) | 55.2 (11.4) |
| Age in categories, y | ||
| 18–40 | 604 (12.0) | 526 (10.6) |
| 41–50 | 1411 (28.0) | 1124 (22.6) |
| 51–60 | 1452 (28.9) | 1781 (35.8) |
| 61–70 | 1039 (20.7) | 1002 (20.2) |
| ≥71 | 739 (14.7) | 816 (16.4) |
| Missing | 16 (0.32) | 15 (0.30) |
| Study | ||
| BWHS | 1425 (28.2) | 2871 (57.5) |
| CPS3 | 32 (0.6) | 78 (1.6) |
| CPSII | 58 (1.1) | 48 (1.0) |
| CTS | 55 (1.1) | 50 (1.0) |
| MEC | 681 (13.5) | 702 (14.1) |
| BEST | 397 (7.9) | 0 (0.0) |
| NC-BCFR | 667 (13.2) | 54 (1.1) |
| UCIBCS | 74 (1.5) | 14 (0.3) |
| WCHS | 1611 (31.9) | 1120 (22.4) |
| WWHS | 54 (1.1) | 56 (1.1) |
| First-degree family history of breast cancer | ||
| No | 4038 (81.8) | 4403 (89.2) |
| Yes | 897 (18.2) | 531 (10.8) |
| Unknown | 119 | 59 |
| Estrogen receptor status | ||
| Negative | 1340 (30.6) | — |
| Positive | 3038 (69.4) | — |
| Unknown | 676 | — |
| Triple-negative breast cancer | ||
| No | 3370 (83.7) | — |
| Yes | 654 (16.3) | — |
| Unknown | 1030 | — |
| Participant characteristics | Affected (n = 5054) No. (%) | Unaffected (n = 4993) No. (%) |
|---|---|---|
| Age in years, mean (SD) | 54.4 (12.0) | 55.2 (11.4) |
| Age in categories, y | ||
| 18–40 | 604 (12.0) | 526 (10.6) |
| 41–50 | 1411 (28.0) | 1124 (22.6) |
| 51–60 | 1452 (28.9) | 1781 (35.8) |
| 61–70 | 1039 (20.7) | 1002 (20.2) |
| ≥71 | 739 (14.7) | 816 (16.4) |
| Missing | 16 (0.32) | 15 (0.30) |
| Study | ||
| BWHS | 1425 (28.2) | 2871 (57.5) |
| CPS3 | 32 (0.6) | 78 (1.6) |
| CPSII | 58 (1.1) | 48 (1.0) |
| CTS | 55 (1.1) | 50 (1.0) |
| MEC | 681 (13.5) | 702 (14.1) |
| BEST | 397 (7.9) | 0 (0.0) |
| NC-BCFR | 667 (13.2) | 54 (1.1) |
| UCIBCS | 74 (1.5) | 14 (0.3) |
| WCHS | 1611 (31.9) | 1120 (22.4) |
| WWHS | 54 (1.1) | 56 (1.1) |
| First-degree family history of breast cancer | ||
| No | 4038 (81.8) | 4403 (89.2) |
| Yes | 897 (18.2) | 531 (10.8) |
| Unknown | 119 | 59 |
| Estrogen receptor status | ||
| Negative | 1340 (30.6) | — |
| Positive | 3038 (69.4) | — |
| Unknown | 676 | — |
| Triple-negative breast cancer | ||
| No | 3370 (83.7) | — |
| Yes | 654 (16.3) | — |
| Unknown | 1030 | — |
BWHS = Black Women’s Health Study (20,21); CPS3 = Cancer Prevention Study 3 (22); CPSII = Cancer Prevention Study II (23); CTS = California Teachers Study (24); MEC = Multiethnic Cohort (25); BEST = Black Women: Etiology and Survival of TNBC (26); NC-BCFR = Northern California Breast Cancer Family Registry (27); UCIBCS = University of California Breast Cancer Study (28); WCHS = Women Circle of Health (29); WWHS = Wisconsin Women’s Health Study (30).
Characteristics of study participants by breast cancer status*
| Participant characteristics | Affected (n = 5054) No. (%) | Unaffected (n = 4993) No. (%) |
|---|---|---|
| Age in years, mean (SD) | 54.4 (12.0) | 55.2 (11.4) |
| Age in categories, y | ||
| 18–40 | 604 (12.0) | 526 (10.6) |
| 41–50 | 1411 (28.0) | 1124 (22.6) |
| 51–60 | 1452 (28.9) | 1781 (35.8) |
| 61–70 | 1039 (20.7) | 1002 (20.2) |
| ≥71 | 739 (14.7) | 816 (16.4) |
| Missing | 16 (0.32) | 15 (0.30) |
| Study | ||
| BWHS | 1425 (28.2) | 2871 (57.5) |
| CPS3 | 32 (0.6) | 78 (1.6) |
| CPSII | 58 (1.1) | 48 (1.0) |
| CTS | 55 (1.1) | 50 (1.0) |
| MEC | 681 (13.5) | 702 (14.1) |
| BEST | 397 (7.9) | 0 (0.0) |
| NC-BCFR | 667 (13.2) | 54 (1.1) |
| UCIBCS | 74 (1.5) | 14 (0.3) |
| WCHS | 1611 (31.9) | 1120 (22.4) |
| WWHS | 54 (1.1) | 56 (1.1) |
| First-degree family history of breast cancer | ||
| No | 4038 (81.8) | 4403 (89.2) |
| Yes | 897 (18.2) | 531 (10.8) |
| Unknown | 119 | 59 |
| Estrogen receptor status | ||
| Negative | 1340 (30.6) | — |
| Positive | 3038 (69.4) | — |
| Unknown | 676 | — |
| Triple-negative breast cancer | ||
| No | 3370 (83.7) | — |
| Yes | 654 (16.3) | — |
| Unknown | 1030 | — |
| Participant characteristics | Affected (n = 5054) No. (%) | Unaffected (n = 4993) No. (%) |
|---|---|---|
| Age in years, mean (SD) | 54.4 (12.0) | 55.2 (11.4) |
| Age in categories, y | ||
| 18–40 | 604 (12.0) | 526 (10.6) |
| 41–50 | 1411 (28.0) | 1124 (22.6) |
| 51–60 | 1452 (28.9) | 1781 (35.8) |
| 61–70 | 1039 (20.7) | 1002 (20.2) |
| ≥71 | 739 (14.7) | 816 (16.4) |
| Missing | 16 (0.32) | 15 (0.30) |
| Study | ||
| BWHS | 1425 (28.2) | 2871 (57.5) |
| CPS3 | 32 (0.6) | 78 (1.6) |
| CPSII | 58 (1.1) | 48 (1.0) |
| CTS | 55 (1.1) | 50 (1.0) |
| MEC | 681 (13.5) | 702 (14.1) |
| BEST | 397 (7.9) | 0 (0.0) |
| NC-BCFR | 667 (13.2) | 54 (1.1) |
| UCIBCS | 74 (1.5) | 14 (0.3) |
| WCHS | 1611 (31.9) | 1120 (22.4) |
| WWHS | 54 (1.1) | 56 (1.1) |
| First-degree family history of breast cancer | ||
| No | 4038 (81.8) | 4403 (89.2) |
| Yes | 897 (18.2) | 531 (10.8) |
| Unknown | 119 | 59 |
| Estrogen receptor status | ||
| Negative | 1340 (30.6) | — |
| Positive | 3038 (69.4) | — |
| Unknown | 676 | — |
| Triple-negative breast cancer | ||
| No | 3370 (83.7) | — |
| Yes | 654 (16.3) | — |
| Unknown | 1030 | — |
BWHS = Black Women’s Health Study (20,21); CPS3 = Cancer Prevention Study 3 (22); CPSII = Cancer Prevention Study II (23); CTS = California Teachers Study (24); MEC = Multiethnic Cohort (25); BEST = Black Women: Etiology and Survival of TNBC (26); NC-BCFR = Northern California Breast Cancer Family Registry (27); UCIBCS = University of California Breast Cancer Study (28); WCHS = Women Circle of Health (29); WWHS = Wisconsin Women’s Health Study (30).
DNA Sequencing
Genomic DNA samples were subjected to multiplex amplicon-based analysis of 746 target regions covering all coding regions and consensus splice sites from 37 cancer predisposition genes using a QIAseq (QIAGEN) (32) custom panel. These genes were selected because of inclusion on commercial hereditary cancer genetic testing panels or because of previous reports suggesting associations with breast, ovarian, endometrial, colorectal, or pancreatic cancer (2,33–35). The QIAseq protocol was optimized for high-throughput robotic processing of DNA samples and validated as previously described (36). Libraries were individually bar coded by dual indexing and sequenced in pools of 768 on a HiSeq4000. Median sequence read depth was 200X. Twenty-three genes previously implicated in breast cancer were evaluated for this study: ATM, BARD1, BRCA1, BRCA2, BRIP1, CDH1, CDKN2A, CHEK2, ERCC3, FANCC, FANCM, MLH1, MRE11A, MSH2, MSH6, NBN, NF1, PALB2, PTEN, RAD51C, RAD51D, RECQL, and TP53 (Supplementary Table 2, available online).
Bioinformatics Analysis
FASTQ files of DNA sequences were generated for each sample from pools of 768 using dual indexing. Reads were trimmed with Cutadapt v1.10 and aligned with bwa-mem v0.7.10. Sequence realignment, recalibration, haplotype calling, and depth of coverage were conducted using GATK v3.4–46. Nucleotide reads of greater than 20X was set as the quality control threshold for coverage, and 99.8% of samples had sequencing coverage above 20X for more than 90% of target nucleotides. Samples with high levels of homozygosity were excluded. Annotation of variants was provided through the BioR toolkit (37) leveraging dbNSFP v3.0 (38), ClinVar (39), and CAVA (40). Variants were viewed and filtered with VCF-Miner (41). Bam files of classified pathogenic variants were viewed by Integrative Genomics Viewer. All loss of function variants [nonsense, frameshift, consensus splice sites (+/-1 or 2)] and any intronic or missense variants defined as pathogenic or likely pathogenic in ClinVar by 2 or more clinical laboratories (Ambry Genetics, SCRP, InVitae, GeneDX, Counsyl, InSiGHT) were considered pathogenic. All suspected mosaic somatic variants (allele ratio > 80:20) and truncating variants in the last 55 bp of the penultimate exon or last exon that potentially avoid nonsense-mediated mRNA decay and do not influence known functional domains were excluded. Variants positioned after established cutoffs for protein function (eg, BRCA2 p. Tyr3208X) were excluded. Reduced penetrance variants, all CHEK2 missense variants, and variants with minor allele frequency greater than 0.3%, other than common founder mutations (eg, CHEK2 c.1100delC), were excluded.
Statistical Analysis
Frequencies of mutations in each gene were estimated in affected and unaffected women for all studies combined. Associations between combined mutations in each gene and breast cancer risk were assessed using logistic regression adjusted for age, first-degree family history of breast cancer, and study design (cohort, case control, other). Separate analyses restricted to ER-positive, ER-negative, and triple-negative breast cancer (TNBC) (ER-negative, progesterone receptor negative, HER2-negative) status, and analyses stratified by age and family history were also conducted. A case-only logistic regression analysis for enrichment of mutations by ER-positive relative to ER-negative status was conducted. All analyses were performed in R (version 3.4.2), and all tests were two-sided. A P value of less than .05 was considered statistically significant. Lifetime absolute risk of breast cancer was estimated for carriers of mutations in specific genes by combining odds ratio (OR) estimates with age-specific AA breast cancer incidence rates from the Surveillance, Epidemiology, and End Results program and age-specific mortality rates from the Centers for Disease Control and Prevention in a competing risk model (Supplementary Materials, available online) (42).
Results
As shown in Table 1, mean age at diagnosis for women with breast cancer was 54.4 years, and 40% were diagnosed at age 50 years or younger. Eighteen percent of affected and 10.8% of unaffected women had a first-degree relative with breast cancer. Tumor ER status was available for 86% of breast cancers: 1340 (30.6%) were ER-negative and 3038 (69.4%) ER-positive.
Pathogenic mutations in the 23 genes tested were identified in 416 (8.2%) of 5054 affected women and 114 (2.3%) of 4993 unaffected women (Table 2). Among women with breast cancer, 81 (1.6%) had mutations in BRCA1, 98 (1.9%) in BRCA2, and 53 (1.0%) in PALB2. In contrast, only 1 mutation in BRCA1 (0.02%), 12 (0.24%) in BRCA2, and 5 (0.10%) in PALB2 were observed in unaffected women. We compared BRCA1 mutations classified as benign or as variants of unknown significance and found similar frequencies in affected vs unaffected women (6.0% vs 6.5% for benign and 5.2% vs 4.5% for variants of unknown significance; data not shown), suggesting that the low frequency of BRCA1 mutations in unaffected women was not caused by sequencing issues. Mutations in genes associated with complex syndromes including CDH1, NF1, PTEN, and TP53 were observed in 15 (0.30%) affected and 4 (0.08%) unaffected women. When we restricted to the 12 genes previously shown to confer moderate or high risk of breast cancer in women of EA (ATM, BARD1, BRCA1, BRCA2, CDH1, CHEK2, NF1, PALB2, PTEN, RAD51C, RAD51D, and TP53) (1, 2), mutations were identified in 6.5% of affected and 1.1% of unaffected women.
Frequency of pathogenic mutations in known or suspected breast cancer susceptibility genes and associations with breast cancer risk in African American women
| Gene | Affected (n = 5054) | Unaffected (n = 4993) | ||
|---|---|---|---|---|
| No. of mutated alleles (mutation frequency, %) | No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | |
| ATM | 39 (0.77) | 16 (0.32) | 1.81 (1.00 to 3.44) | .058 |
| BARD1 | 7 (0.14) | 8 (0.16) | 0.78 (0.26 to 2.27) | .64 |
| BRCA1 | 81 (1.60) | 1 (0.02) | 47.55 (10.43 to >100) | <.001 |
| BRCA2 | 98 (1.94) | 12 (0.24) | 7.25 (4.07 to 14.12) | <.001 |
| BRIP1 | 9 (0.18) | 6 (0.12) | 1.24 (0.42 to 3.95) | .70 |
| CDH1 | 4 (0.08) | 2 (0.04) | 1.53 (0.27 to 12.02 | .64 |
| CDKN2A | 1 (0.02) | — | —‡ | — |
| CHEK2 | 19 (0.38) | 6 (0.12) | 3.23 (1.31 to 9.16) | .016 |
| ERCC3 | 14 (0.28) | 9 (0.18) | 2.40 (1.04 to 5.86) | .044 |
| FANCC | 21 (0.42) | 10 (0.20) | 2.03 (0.93 to 4.69) | .084 |
| FANCM | 13 (0.26) | 11 (0.22) | 1.14 (0.48 to 2.72) | .76 |
| MLH1 | — | 1 (0.02) | — | — |
| MSH2 | — | — | — | — |
| MRE11A | 2 (0.04) | 3 (0.06) | — | — |
| MSH6 | 4 (0.08) | 2 (0.04) | 1.77 (0.31 to 13.74) | .53 |
| NBN | 7 (0.14) | 10 (0.20) | 0.58 (0.20 to 1.59) | .29 |
| NF1 | 6 (0.12) | 1 (0.02) | — | — |
| PALB2 | 53 (1.05) | 5 (0.10) | 8.54 (3.67 to 24.95) | <.001 |
| PTEN | — | — | — | — |
| RAD51C | 9 (0.18) | 3 (0.06) | 3.00 (0.86 to 13.85) | .11 |
| RAD51D | 8 (0.16) | 2 (0.04) | 2.85 (0.66 to 19.90) | .21 |
| RECQL | 16 (0.32) | 5 (0.10) | 3.04 (1.15 to 9.54) | .036 |
| TP53 | 5 (0.10) | 1 (0.02) | — | — |
| Total | 416 (8.23) | 114 (2.28) |
| Gene | Affected (n = 5054) | Unaffected (n = 4993) | ||
|---|---|---|---|---|
| No. of mutated alleles (mutation frequency, %) | No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | |
| ATM | 39 (0.77) | 16 (0.32) | 1.81 (1.00 to 3.44) | .058 |
| BARD1 | 7 (0.14) | 8 (0.16) | 0.78 (0.26 to 2.27) | .64 |
| BRCA1 | 81 (1.60) | 1 (0.02) | 47.55 (10.43 to >100) | <.001 |
| BRCA2 | 98 (1.94) | 12 (0.24) | 7.25 (4.07 to 14.12) | <.001 |
| BRIP1 | 9 (0.18) | 6 (0.12) | 1.24 (0.42 to 3.95) | .70 |
| CDH1 | 4 (0.08) | 2 (0.04) | 1.53 (0.27 to 12.02 | .64 |
| CDKN2A | 1 (0.02) | — | —‡ | — |
| CHEK2 | 19 (0.38) | 6 (0.12) | 3.23 (1.31 to 9.16) | .016 |
| ERCC3 | 14 (0.28) | 9 (0.18) | 2.40 (1.04 to 5.86) | .044 |
| FANCC | 21 (0.42) | 10 (0.20) | 2.03 (0.93 to 4.69) | .084 |
| FANCM | 13 (0.26) | 11 (0.22) | 1.14 (0.48 to 2.72) | .76 |
| MLH1 | — | 1 (0.02) | — | — |
| MSH2 | — | — | — | — |
| MRE11A | 2 (0.04) | 3 (0.06) | — | — |
| MSH6 | 4 (0.08) | 2 (0.04) | 1.77 (0.31 to 13.74) | .53 |
| NBN | 7 (0.14) | 10 (0.20) | 0.58 (0.20 to 1.59) | .29 |
| NF1 | 6 (0.12) | 1 (0.02) | — | — |
| PALB2 | 53 (1.05) | 5 (0.10) | 8.54 (3.67 to 24.95) | <.001 |
| PTEN | — | — | — | — |
| RAD51C | 9 (0.18) | 3 (0.06) | 3.00 (0.86 to 13.85) | .11 |
| RAD51D | 8 (0.16) | 2 (0.04) | 2.85 (0.66 to 19.90) | .21 |
| RECQL | 16 (0.32) | 5 (0.10) | 3.04 (1.15 to 9.54) | .036 |
| TP53 | 5 (0.10) | 1 (0.02) | — | — |
| Total | 416 (8.23) | 114 (2.28) |
Odds ratios (ORs) adjusted for study design, age, and first-degree family history of breast cancer. Reference group is women who have no mutations in the given gene. CI = confidence interval.
Two-sided P values from logistic regression analysis.
ORs not calculated because of small numbers of mutations.
Frequency of pathogenic mutations in known or suspected breast cancer susceptibility genes and associations with breast cancer risk in African American women
| Gene | Affected (n = 5054) | Unaffected (n = 4993) | ||
|---|---|---|---|---|
| No. of mutated alleles (mutation frequency, %) | No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | |
| ATM | 39 (0.77) | 16 (0.32) | 1.81 (1.00 to 3.44) | .058 |
| BARD1 | 7 (0.14) | 8 (0.16) | 0.78 (0.26 to 2.27) | .64 |
| BRCA1 | 81 (1.60) | 1 (0.02) | 47.55 (10.43 to >100) | <.001 |
| BRCA2 | 98 (1.94) | 12 (0.24) | 7.25 (4.07 to 14.12) | <.001 |
| BRIP1 | 9 (0.18) | 6 (0.12) | 1.24 (0.42 to 3.95) | .70 |
| CDH1 | 4 (0.08) | 2 (0.04) | 1.53 (0.27 to 12.02 | .64 |
| CDKN2A | 1 (0.02) | — | —‡ | — |
| CHEK2 | 19 (0.38) | 6 (0.12) | 3.23 (1.31 to 9.16) | .016 |
| ERCC3 | 14 (0.28) | 9 (0.18) | 2.40 (1.04 to 5.86) | .044 |
| FANCC | 21 (0.42) | 10 (0.20) | 2.03 (0.93 to 4.69) | .084 |
| FANCM | 13 (0.26) | 11 (0.22) | 1.14 (0.48 to 2.72) | .76 |
| MLH1 | — | 1 (0.02) | — | — |
| MSH2 | — | — | — | — |
| MRE11A | 2 (0.04) | 3 (0.06) | — | — |
| MSH6 | 4 (0.08) | 2 (0.04) | 1.77 (0.31 to 13.74) | .53 |
| NBN | 7 (0.14) | 10 (0.20) | 0.58 (0.20 to 1.59) | .29 |
| NF1 | 6 (0.12) | 1 (0.02) | — | — |
| PALB2 | 53 (1.05) | 5 (0.10) | 8.54 (3.67 to 24.95) | <.001 |
| PTEN | — | — | — | — |
| RAD51C | 9 (0.18) | 3 (0.06) | 3.00 (0.86 to 13.85) | .11 |
| RAD51D | 8 (0.16) | 2 (0.04) | 2.85 (0.66 to 19.90) | .21 |
| RECQL | 16 (0.32) | 5 (0.10) | 3.04 (1.15 to 9.54) | .036 |
| TP53 | 5 (0.10) | 1 (0.02) | — | — |
| Total | 416 (8.23) | 114 (2.28) |
| Gene | Affected (n = 5054) | Unaffected (n = 4993) | ||
|---|---|---|---|---|
| No. of mutated alleles (mutation frequency, %) | No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | |
| ATM | 39 (0.77) | 16 (0.32) | 1.81 (1.00 to 3.44) | .058 |
| BARD1 | 7 (0.14) | 8 (0.16) | 0.78 (0.26 to 2.27) | .64 |
| BRCA1 | 81 (1.60) | 1 (0.02) | 47.55 (10.43 to >100) | <.001 |
| BRCA2 | 98 (1.94) | 12 (0.24) | 7.25 (4.07 to 14.12) | <.001 |
| BRIP1 | 9 (0.18) | 6 (0.12) | 1.24 (0.42 to 3.95) | .70 |
| CDH1 | 4 (0.08) | 2 (0.04) | 1.53 (0.27 to 12.02 | .64 |
| CDKN2A | 1 (0.02) | — | —‡ | — |
| CHEK2 | 19 (0.38) | 6 (0.12) | 3.23 (1.31 to 9.16) | .016 |
| ERCC3 | 14 (0.28) | 9 (0.18) | 2.40 (1.04 to 5.86) | .044 |
| FANCC | 21 (0.42) | 10 (0.20) | 2.03 (0.93 to 4.69) | .084 |
| FANCM | 13 (0.26) | 11 (0.22) | 1.14 (0.48 to 2.72) | .76 |
| MLH1 | — | 1 (0.02) | — | — |
| MSH2 | — | — | — | — |
| MRE11A | 2 (0.04) | 3 (0.06) | — | — |
| MSH6 | 4 (0.08) | 2 (0.04) | 1.77 (0.31 to 13.74) | .53 |
| NBN | 7 (0.14) | 10 (0.20) | 0.58 (0.20 to 1.59) | .29 |
| NF1 | 6 (0.12) | 1 (0.02) | — | — |
| PALB2 | 53 (1.05) | 5 (0.10) | 8.54 (3.67 to 24.95) | <.001 |
| PTEN | — | — | — | — |
| RAD51C | 9 (0.18) | 3 (0.06) | 3.00 (0.86 to 13.85) | .11 |
| RAD51D | 8 (0.16) | 2 (0.04) | 2.85 (0.66 to 19.90) | .21 |
| RECQL | 16 (0.32) | 5 (0.10) | 3.04 (1.15 to 9.54) | .036 |
| TP53 | 5 (0.10) | 1 (0.02) | — | — |
| Total | 416 (8.23) | 114 (2.28) |
Odds ratios (ORs) adjusted for study design, age, and first-degree family history of breast cancer. Reference group is women who have no mutations in the given gene. CI = confidence interval.
Two-sided P values from logistic regression analysis.
ORs not calculated because of small numbers of mutations.
Several recurrent mutations were observed, including 8 that accounted for 51% of the 81 mutations in BRCA1 among affected women (Supplementary Table 3, available online). The most frequent recurrent BRCA1 mutation (c.815_824dup10) has been previously reported as being of African origin (43). The 5 most common mutations in BRCA2 accounted for only 22% of all mutations. The c.1100delC CHEK2 recurrent mutation from non-Hispanic whites accounted for 9 of 19 and 2 of 6 CHEK2 mutations in affected and unaffected women, respectively; c.1354C>T, p. Arg452X in ERCC3 accounted for 6 of 14 and 5 of 9 ERCC3 mutations in affected and unaffected, respectively; c.355_360delTCTCATinsA in FANCC accounted for 13 of 21 and 7 of 10 FANCC mutations in affected and unaffected, respectively; and c.3323delA accounted for 8 of 53 and 1 of 5 PALB2 mutations in affected and unaffected, respectively.
As shown in Table 2, statistically significant associations with increased breast cancer risk were observed for 6 genes (BRCA1, BRCA2, CHEK2, ERCC3, PALB2, and RECQL). In addition, the odds ratio for an association of breast cancer with mutations in ATM was 1.81 (95% CI = 1.00 to 3.44). Odds ratios were greater than 4.0 for BRCA1 (OR = 47.55, 95% CI = 10.43 to 842), BRCA2 (OR = 7.25, 95% CI = 4.07 to 14.12), and PALB2 (OR = 8.54, 95% CI = 3.67 to 24.95). Protein truncating mutations in CHEK2 (OR = 3.23, 95% CI = 1.31 to 9.16), ERCC3 (OR = 2.40, 95% CI = 1.04 to 5.86), and RECQL (OR = 3.04, 95% CI = 1.15 to 9.54) were associated with moderately increased risks of breast cancer. In an analysis restricted to population-based studies (Table 3), results were similar, and further control for individual study did not materially change the odds ratio estimates (Supplementary Table 4, available online). In a sensitivity analysis that excluded affected women if samples were provided more than a year after breast cancer diagnosis (excluded n = 837), odds ratios were essentially unchanged (eg, OR = 31.9, 95% CI = 6.7 to >100 for BRCA1; OR = 7.1, 95% CI = 3.9 to 14.2 for BRCA2; and OR = 9.7, 95% CI = 4.1 to 28.9 for PALB2).
Frequency of pathogenic mutations in known or suspected breast cancer susceptibility genes and associations with breast cancer risk in African American women, in population-based studies*
| Gene | Affected (n = 3916) | Unaffected (n = 4925) | ||
|---|---|---|---|---|
| No. of mutated alleles (mutation frequency, %) | No. of mutated alleles (mutation frequency, %) | OR†(95% CI) | P‡ | |
| ATM | 28 (0.72) | 16 (0.33) | 1.81 (0.97 to 3.48) | .067 |
| BARD1 | 7 (0.18) | 8 (0.16) | 0.98 (0.34 to 2.80) | .97 |
| BRCA1 | 41 (1.05) | 1 (0.02) | 42.79 (9.24 to >100) | <.001 |
| BRCA2 | 72 (1.84) | 12 (0.24) | 7.31 (4.08 to 14.29) | <.001 |
| BRIP1 | 6 (0.15) | 6 (0.12) | 1.14 (0.34 to 3.79) | .83 |
| CHEK2 | 15 (0.38) | 6 (0.12) | 3.17 (1.26 to 9.06) | .020 |
| ERCC3 | 13 (0.33) | 9 (0.18) | 2.35 (1.01 to 5.76) | .051 |
| FANCC | 16 (0.41) | 10 (0.20) | 2.24 (1.02 to 5.18) | .049 |
| FANCM | 11 (0.28) | 11 (0.22) | 1.17 (0.49 to 2.82) | .72 |
| NBN | 4 (0.10) | 9 (0.18) | 0.51 (0.13 to 1.63) | .28 |
| PALB2 | 39 (1.00) | 5 (0.10) | 8.37 (3.56 to 24.57) | <.001 |
| RAD51C | 7 (0.18) | 3 (0.06) | 2.95 (0.80 to 13.72) | .12 |
| RAD51D | 6 (0.15) | 2 (0.04) | 3.06 (0.67 to 21.50) | .18 |
| RECQL | 12 (0.31) | 5 (0.10) | 2.94 (1.07 to 9.37) | .047 |
| Total | 277 (7.07) | 103 (2.09) |
| Gene | Affected (n = 3916) | Unaffected (n = 4925) | ||
|---|---|---|---|---|
| No. of mutated alleles (mutation frequency, %) | No. of mutated alleles (mutation frequency, %) | OR†(95% CI) | P‡ | |
| ATM | 28 (0.72) | 16 (0.33) | 1.81 (0.97 to 3.48) | .067 |
| BARD1 | 7 (0.18) | 8 (0.16) | 0.98 (0.34 to 2.80) | .97 |
| BRCA1 | 41 (1.05) | 1 (0.02) | 42.79 (9.24 to >100) | <.001 |
| BRCA2 | 72 (1.84) | 12 (0.24) | 7.31 (4.08 to 14.29) | <.001 |
| BRIP1 | 6 (0.15) | 6 (0.12) | 1.14 (0.34 to 3.79) | .83 |
| CHEK2 | 15 (0.38) | 6 (0.12) | 3.17 (1.26 to 9.06) | .020 |
| ERCC3 | 13 (0.33) | 9 (0.18) | 2.35 (1.01 to 5.76) | .051 |
| FANCC | 16 (0.41) | 10 (0.20) | 2.24 (1.02 to 5.18) | .049 |
| FANCM | 11 (0.28) | 11 (0.22) | 1.17 (0.49 to 2.82) | .72 |
| NBN | 4 (0.10) | 9 (0.18) | 0.51 (0.13 to 1.63) | .28 |
| PALB2 | 39 (1.00) | 5 (0.10) | 8.37 (3.56 to 24.57) | <.001 |
| RAD51C | 7 (0.18) | 3 (0.06) | 2.95 (0.80 to 13.72) | .12 |
| RAD51D | 6 (0.15) | 2 (0.04) | 3.06 (0.67 to 21.50) | .18 |
| RECQL | 12 (0.31) | 5 (0.10) | 2.94 (1.07 to 9.37) | .047 |
| Total | 277 (7.07) | 103 (2.09) |
Studies that did not preferentially enroll cases based on family history or age; studies included were Black Women’s Health Study, Cancer Prevention Study II, Cancer Prevention Study 3, California Teachers Study, Multiethnic Cohort, Women Circle of Health, and Wisconsin Women’s Health Study. CI = confidence interval.
Odds ratios (ORs) adjusted for study design, age, and first-degree family history of breast cancer. Reference group is women who have no mutations in the given gene.
Two-sided P values from logistic regression analysis.
Frequency of pathogenic mutations in known or suspected breast cancer susceptibility genes and associations with breast cancer risk in African American women, in population-based studies*
| Gene | Affected (n = 3916) | Unaffected (n = 4925) | ||
|---|---|---|---|---|
| No. of mutated alleles (mutation frequency, %) | No. of mutated alleles (mutation frequency, %) | OR†(95% CI) | P‡ | |
| ATM | 28 (0.72) | 16 (0.33) | 1.81 (0.97 to 3.48) | .067 |
| BARD1 | 7 (0.18) | 8 (0.16) | 0.98 (0.34 to 2.80) | .97 |
| BRCA1 | 41 (1.05) | 1 (0.02) | 42.79 (9.24 to >100) | <.001 |
| BRCA2 | 72 (1.84) | 12 (0.24) | 7.31 (4.08 to 14.29) | <.001 |
| BRIP1 | 6 (0.15) | 6 (0.12) | 1.14 (0.34 to 3.79) | .83 |
| CHEK2 | 15 (0.38) | 6 (0.12) | 3.17 (1.26 to 9.06) | .020 |
| ERCC3 | 13 (0.33) | 9 (0.18) | 2.35 (1.01 to 5.76) | .051 |
| FANCC | 16 (0.41) | 10 (0.20) | 2.24 (1.02 to 5.18) | .049 |
| FANCM | 11 (0.28) | 11 (0.22) | 1.17 (0.49 to 2.82) | .72 |
| NBN | 4 (0.10) | 9 (0.18) | 0.51 (0.13 to 1.63) | .28 |
| PALB2 | 39 (1.00) | 5 (0.10) | 8.37 (3.56 to 24.57) | <.001 |
| RAD51C | 7 (0.18) | 3 (0.06) | 2.95 (0.80 to 13.72) | .12 |
| RAD51D | 6 (0.15) | 2 (0.04) | 3.06 (0.67 to 21.50) | .18 |
| RECQL | 12 (0.31) | 5 (0.10) | 2.94 (1.07 to 9.37) | .047 |
| Total | 277 (7.07) | 103 (2.09) |
| Gene | Affected (n = 3916) | Unaffected (n = 4925) | ||
|---|---|---|---|---|
| No. of mutated alleles (mutation frequency, %) | No. of mutated alleles (mutation frequency, %) | OR†(95% CI) | P‡ | |
| ATM | 28 (0.72) | 16 (0.33) | 1.81 (0.97 to 3.48) | .067 |
| BARD1 | 7 (0.18) | 8 (0.16) | 0.98 (0.34 to 2.80) | .97 |
| BRCA1 | 41 (1.05) | 1 (0.02) | 42.79 (9.24 to >100) | <.001 |
| BRCA2 | 72 (1.84) | 12 (0.24) | 7.31 (4.08 to 14.29) | <.001 |
| BRIP1 | 6 (0.15) | 6 (0.12) | 1.14 (0.34 to 3.79) | .83 |
| CHEK2 | 15 (0.38) | 6 (0.12) | 3.17 (1.26 to 9.06) | .020 |
| ERCC3 | 13 (0.33) | 9 (0.18) | 2.35 (1.01 to 5.76) | .051 |
| FANCC | 16 (0.41) | 10 (0.20) | 2.24 (1.02 to 5.18) | .049 |
| FANCM | 11 (0.28) | 11 (0.22) | 1.17 (0.49 to 2.82) | .72 |
| NBN | 4 (0.10) | 9 (0.18) | 0.51 (0.13 to 1.63) | .28 |
| PALB2 | 39 (1.00) | 5 (0.10) | 8.37 (3.56 to 24.57) | <.001 |
| RAD51C | 7 (0.18) | 3 (0.06) | 2.95 (0.80 to 13.72) | .12 |
| RAD51D | 6 (0.15) | 2 (0.04) | 3.06 (0.67 to 21.50) | .18 |
| RECQL | 12 (0.31) | 5 (0.10) | 2.94 (1.07 to 9.37) | .047 |
| Total | 277 (7.07) | 103 (2.09) |
Studies that did not preferentially enroll cases based on family history or age; studies included were Black Women’s Health Study, Cancer Prevention Study II, Cancer Prevention Study 3, California Teachers Study, Multiethnic Cohort, Women Circle of Health, and Wisconsin Women’s Health Study. CI = confidence interval.
Odds ratios (ORs) adjusted for study design, age, and first-degree family history of breast cancer. Reference group is women who have no mutations in the given gene.
Two-sided P values from logistic regression analysis.
Table 4 provides mutation data and association results separately for ER-negative and ER-positive AA breast cancer. Pathogenic mutations were identified in 10.3% of women with ER-negative breast cancer, 5.2% of women with ER-positive breast cancer, and 2.3% of unaffected women. BRCA1, BRCA2, and PALB2 mutations were associated with increased risks of ER-negative breast cancer (Table 4) and TNBC (Supplementary Table 5, available online). There was evidence of association for both RAD51D (OR = 7.82, 95% CI = 1.61 to 57.42) and RAD51C (OR = 4.23, 95% CI = 0.88 to 22.72) with increased risk of ER-negative breast cancer (Table 4). BRCA1 (P < .001), PALB2 (P = .003), and RAD51D (P = .015) mutations were more strongly associated with ER-negative than ER-positive breast cancer (Supplementary Table 6, available online), although odds ratios for BRCA1 and PALB2 were above 5.0 for both ER subtypes. ATM, CHEK2, ERCC3, and FANCC were associated with ER-positive breast cancer only.
Associations between pathogenic mutations in breast cancer predisposition genes and estrogen receptor tumor subtype in African American women
| Gene | Estrogen receptor-negative breast cancer | Estrogen receptor-positive breast cancer | ||||
|---|---|---|---|---|---|---|
| Affected (n = 1340)No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | Affected (n = 3038)No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | |
| ATM | 6 (0.44) | 1.00 (0.34 to 2.60) | .99 | 28 (0.92) | 2.08 (1.09 to 4.08) | .029 |
| BARD1 | 3 (0.22) | 1.21 (0.25 to 4.54) | .78 | 3 (0.10) | 0.66 (0.14 to 2.41) | .55 |
| BRCA1 | 60 (4.48) | 129.7 (28.0 to >100) | <.001 | 19 (0.63) | 15.58 (3.09 to >100) | .008 |
| BRCA2 | 31 (2.31) | 9.38 (4.76 to 19.62) | <.001 | 57 (1.88) | 6.83 (3.67 to 13.72) | <.001 |
| BRIP1 | 3 (0.22) | 1.72 (0.34 to 7.23) | .47 | 4 (0.13) | 0.85 (0.20 to 3.30) | .82 |
| CDH1 | 3 (0.22) | 4.75 (0.69 to 40.6) | .47 | 1 (0.03) | — | — |
| CHEK2 | 2 (0.15) | —‡ | — | 14 (0.46) | 4.02 (1.52 to 11.86) | .007 |
| ERCC3 | 3 (0.22) | 1.95 (0.42 to 6.81) | .33 | 10 (0.33) | 2.76 (1.08 to 7.10) | .032 |
| FANCC | 5 (0.37) | 2.01 (0.60 to 6.01) | .23 | 14 (0.46) | 2.42 (1.00 to 5.97) | .050 |
| NF1 | 2 (0.15) | — | — | 4 (0.13) | 9.94 (1.37 to >100) | .045 |
| PALB2 | 22 (1.64) | 15.57 (6.09 to 47.97) | < .001 | 22 (0.72) | 5.44 (2.07 to 17.13) | .001 |
| RAD51C | 4 (0.30) | 4.23 (0.88 to 22.72) | .071 | 4 (0.13) | 2.22 (0.47 to 11.71) | .31 |
| RAD51D | 6 (0.44) | 7.82 (1.61 to 57.42) | .018 | 2 (0.07) | — | — |
| RECQL | 4 (0.30) | 2.44 (0.56 to 9.99) | .21 | 8 (0.26) | 2.65 (0.83 to 9.20) | .10 |
| TP53 | — | — | — | 5 (0.16) | 9.24 (1.29 to >100) | .053 |
| Gene | Estrogen receptor-negative breast cancer | Estrogen receptor-positive breast cancer | ||||
|---|---|---|---|---|---|---|
| Affected (n = 1340)No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | Affected (n = 3038)No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | |
| ATM | 6 (0.44) | 1.00 (0.34 to 2.60) | .99 | 28 (0.92) | 2.08 (1.09 to 4.08) | .029 |
| BARD1 | 3 (0.22) | 1.21 (0.25 to 4.54) | .78 | 3 (0.10) | 0.66 (0.14 to 2.41) | .55 |
| BRCA1 | 60 (4.48) | 129.7 (28.0 to >100) | <.001 | 19 (0.63) | 15.58 (3.09 to >100) | .008 |
| BRCA2 | 31 (2.31) | 9.38 (4.76 to 19.62) | <.001 | 57 (1.88) | 6.83 (3.67 to 13.72) | <.001 |
| BRIP1 | 3 (0.22) | 1.72 (0.34 to 7.23) | .47 | 4 (0.13) | 0.85 (0.20 to 3.30) | .82 |
| CDH1 | 3 (0.22) | 4.75 (0.69 to 40.6) | .47 | 1 (0.03) | — | — |
| CHEK2 | 2 (0.15) | —‡ | — | 14 (0.46) | 4.02 (1.52 to 11.86) | .007 |
| ERCC3 | 3 (0.22) | 1.95 (0.42 to 6.81) | .33 | 10 (0.33) | 2.76 (1.08 to 7.10) | .032 |
| FANCC | 5 (0.37) | 2.01 (0.60 to 6.01) | .23 | 14 (0.46) | 2.42 (1.00 to 5.97) | .050 |
| NF1 | 2 (0.15) | — | — | 4 (0.13) | 9.94 (1.37 to >100) | .045 |
| PALB2 | 22 (1.64) | 15.57 (6.09 to 47.97) | < .001 | 22 (0.72) | 5.44 (2.07 to 17.13) | .001 |
| RAD51C | 4 (0.30) | 4.23 (0.88 to 22.72) | .071 | 4 (0.13) | 2.22 (0.47 to 11.71) | .31 |
| RAD51D | 6 (0.44) | 7.82 (1.61 to 57.42) | .018 | 2 (0.07) | — | — |
| RECQL | 4 (0.30) | 2.44 (0.56 to 9.99) | .21 | 8 (0.26) | 2.65 (0.83 to 9.20) | .10 |
| TP53 | — | — | — | 5 (0.16) | 9.24 (1.29 to >100) | .053 |
Odds ratios (ORs) adjusted for study design, age, and first-degree family history of breast cancer. Reference group is women who have no mutations in a given gene. CI = confidence interval.
Two-sided P values from logistic regression analysis.
ORs not calculated because of small numbers of mutations.
Associations between pathogenic mutations in breast cancer predisposition genes and estrogen receptor tumor subtype in African American women
| Gene | Estrogen receptor-negative breast cancer | Estrogen receptor-positive breast cancer | ||||
|---|---|---|---|---|---|---|
| Affected (n = 1340)No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | Affected (n = 3038)No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | |
| ATM | 6 (0.44) | 1.00 (0.34 to 2.60) | .99 | 28 (0.92) | 2.08 (1.09 to 4.08) | .029 |
| BARD1 | 3 (0.22) | 1.21 (0.25 to 4.54) | .78 | 3 (0.10) | 0.66 (0.14 to 2.41) | .55 |
| BRCA1 | 60 (4.48) | 129.7 (28.0 to >100) | <.001 | 19 (0.63) | 15.58 (3.09 to >100) | .008 |
| BRCA2 | 31 (2.31) | 9.38 (4.76 to 19.62) | <.001 | 57 (1.88) | 6.83 (3.67 to 13.72) | <.001 |
| BRIP1 | 3 (0.22) | 1.72 (0.34 to 7.23) | .47 | 4 (0.13) | 0.85 (0.20 to 3.30) | .82 |
| CDH1 | 3 (0.22) | 4.75 (0.69 to 40.6) | .47 | 1 (0.03) | — | — |
| CHEK2 | 2 (0.15) | —‡ | — | 14 (0.46) | 4.02 (1.52 to 11.86) | .007 |
| ERCC3 | 3 (0.22) | 1.95 (0.42 to 6.81) | .33 | 10 (0.33) | 2.76 (1.08 to 7.10) | .032 |
| FANCC | 5 (0.37) | 2.01 (0.60 to 6.01) | .23 | 14 (0.46) | 2.42 (1.00 to 5.97) | .050 |
| NF1 | 2 (0.15) | — | — | 4 (0.13) | 9.94 (1.37 to >100) | .045 |
| PALB2 | 22 (1.64) | 15.57 (6.09 to 47.97) | < .001 | 22 (0.72) | 5.44 (2.07 to 17.13) | .001 |
| RAD51C | 4 (0.30) | 4.23 (0.88 to 22.72) | .071 | 4 (0.13) | 2.22 (0.47 to 11.71) | .31 |
| RAD51D | 6 (0.44) | 7.82 (1.61 to 57.42) | .018 | 2 (0.07) | — | — |
| RECQL | 4 (0.30) | 2.44 (0.56 to 9.99) | .21 | 8 (0.26) | 2.65 (0.83 to 9.20) | .10 |
| TP53 | — | — | — | 5 (0.16) | 9.24 (1.29 to >100) | .053 |
| Gene | Estrogen receptor-negative breast cancer | Estrogen receptor-positive breast cancer | ||||
|---|---|---|---|---|---|---|
| Affected (n = 1340)No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | Affected (n = 3038)No. of mutated alleles (mutation frequency, %) | OR* (95% CI) | P† | |
| ATM | 6 (0.44) | 1.00 (0.34 to 2.60) | .99 | 28 (0.92) | 2.08 (1.09 to 4.08) | .029 |
| BARD1 | 3 (0.22) | 1.21 (0.25 to 4.54) | .78 | 3 (0.10) | 0.66 (0.14 to 2.41) | .55 |
| BRCA1 | 60 (4.48) | 129.7 (28.0 to >100) | <.001 | 19 (0.63) | 15.58 (3.09 to >100) | .008 |
| BRCA2 | 31 (2.31) | 9.38 (4.76 to 19.62) | <.001 | 57 (1.88) | 6.83 (3.67 to 13.72) | <.001 |
| BRIP1 | 3 (0.22) | 1.72 (0.34 to 7.23) | .47 | 4 (0.13) | 0.85 (0.20 to 3.30) | .82 |
| CDH1 | 3 (0.22) | 4.75 (0.69 to 40.6) | .47 | 1 (0.03) | — | — |
| CHEK2 | 2 (0.15) | —‡ | — | 14 (0.46) | 4.02 (1.52 to 11.86) | .007 |
| ERCC3 | 3 (0.22) | 1.95 (0.42 to 6.81) | .33 | 10 (0.33) | 2.76 (1.08 to 7.10) | .032 |
| FANCC | 5 (0.37) | 2.01 (0.60 to 6.01) | .23 | 14 (0.46) | 2.42 (1.00 to 5.97) | .050 |
| NF1 | 2 (0.15) | — | — | 4 (0.13) | 9.94 (1.37 to >100) | .045 |
| PALB2 | 22 (1.64) | 15.57 (6.09 to 47.97) | < .001 | 22 (0.72) | 5.44 (2.07 to 17.13) | .001 |
| RAD51C | 4 (0.30) | 4.23 (0.88 to 22.72) | .071 | 4 (0.13) | 2.22 (0.47 to 11.71) | .31 |
| RAD51D | 6 (0.44) | 7.82 (1.61 to 57.42) | .018 | 2 (0.07) | — | — |
| RECQL | 4 (0.30) | 2.44 (0.56 to 9.99) | .21 | 8 (0.26) | 2.65 (0.83 to 9.20) | .10 |
| TP53 | — | — | — | 5 (0.16) | 9.24 (1.29 to >100) | .053 |
Odds ratios (ORs) adjusted for study design, age, and first-degree family history of breast cancer. Reference group is women who have no mutations in a given gene. CI = confidence interval.
Two-sided P values from logistic regression analysis.
ORs not calculated because of small numbers of mutations.
In an effort to confirm validity of the sequencing, we compared mutation frequencies in the AA unaffected women with frequencies in approximately 7500 gnomAD African/African American reference samples (Supplementary Table 7, available online). Comparing AA women with breast cancer with gnomAD African/African American controls yielded odds ratios of 2.4, 2.6, and 2.0 for ERCC3, FANCC, and RECQL, respectively, consistent with the results from the primary analysis, and the odds ratio for BRCA1 was 13.4, based on 9 controls in gnomAD (Supplementary Table 7, available online).
Results of association analyses stratified on age (younger than 50 years and 50 years and older) (Supplementary Table 8, available online) and by first-degree family history of breast cancer (Supplementary Tables 9 and 10, available online) are also provided. Associations were generally stronger in younger women. Odds ratios were similar after exclusion of women with a family history of breast cancer.
Mutation frequencies in patient categories defined by age and first-degree family history of breast cancer are presented in Figure 1 and Supplementary Table 11, available online. As expected, a high proportion of AA women with breast cancer diagnosed before age 40 years and with a first-degree family history of breast cancer had BRCA1 mutations, and the prevalence of BRCA1 mutations decreased sharply with age at diagnosis. Overall, there was a higher frequency of BRCA1 mutations in women with ER-negative breast cancer (4.5%) than in women with ER-positive cancer (0.63%). In contrast, women with ER-negative breast cancer and those with ER-positive breast cancer had similar frequencies of BRCA2 mutations.
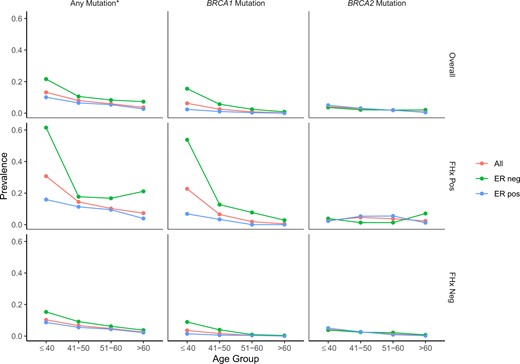
Prevalence of mutations in women with any breast cancer, estrogen receptor-negative (ER-neg) breast cancer, and ER-positive (ER-pos) breast cancer, according to age (in years) at diagnosis and first-degree family history (FHx) of breast cancer. *Any mutation indicates any pathogenic mutation in 12 known breast cancer predisposition genes (ATM, BARD1, BRCA1, BRCA2, CDH1, CHEK2, NF1, PALB2, PTEN, RAD51C, RAD51D, and TP53).
When mutations in any of the 12 genes that have been shown to be associated with moderate or high increase in breast cancer risk (2) were considered, mutation frequencies were strikingly different for ER-negative and ER-positive breast cancer (Figure 1; Supplementary Table 11, available online). In every age group, the prevalence of mutations was approximately twofold higher for ER-negative than for ER-positive disease. Among women aged 40 years and younger, 21% of all those with ER-negative cancer carried a mutation; among women older than 60 years of age, the proportion was 7.0%. As expected, the prevalence of mutations was highest among women with a first-degree family history of breast cancer.
Characteristics of breast cancers from AA women in the population-based studies were similar to characteristics of breast cancers reported to Surveillance, Epidemiology, and End Results registries for AA women during the same time period, as shown in Supplementary Table 12 (available online). Based on mutation frequency and relative risk, we were able to compute estimated absolute risks of breast cancer in BRCA2, PALB2, CHEK2, and ATM AA mutation carriers; absolute risks were 48%, 58%, 30%, and 21% by age 85 years, respectively (Figure 2).
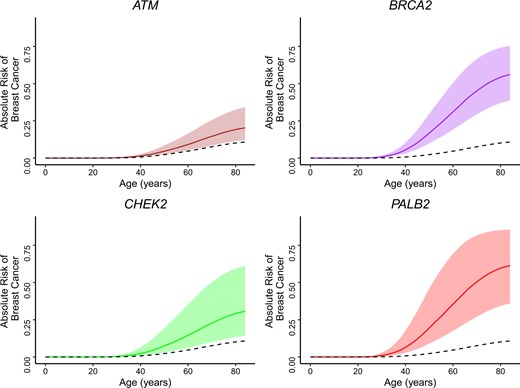
Estimates of absolute risk of breast cancer through age 85 years in African American women who are carriers of pathogenic mutations in 4 specific genes. Dotted line in each figure represents absolute risk of US population of African American women regardless of carrier status.
Discussion
The present findings come from the first large study aimed at identifying breast cancer predisposition genes in an African ancestry population, with 5054 affected and 4993 unaffected AA women. Pathogenic mutations in the 12 genes for which there is the most evidence of association (2), primarily from EA populations, were identified in 6.5% of AA women with breast cancer and 1.1% of unaffected AA women. The frequency of pathogenic mutations was especially high (10.3%) in women with ER-negative breast cancer. This study provides the first estimates of breast cancer risk in African ancestry women associated with predisposition genes other than BRCA1 and BRCA2. The observed associations confirm the utility of current hereditary cancer multigene testing panels for AA women.
We could not accurately estimate relative risk of breast cancer for women with mutations in the BRCA1 gene because only 1 (age 52 years) of the 4993 unaffected women had a pathogenic mutation in BRCA1 (frequency 0.02%). Sequencing problems were excluded as the reason for the low number of mutations in unaffected women. Because the expected number of mutations is quite small, the result could be attributed to unstable estimates. Alternatively, this finding may indicate that BRCA1 mutations are highly penetrant in women of African ancestry. There are limited data on BRCA1 mutation frequency in African ancestry women without breast cancer. The earliest reports on mutation frequencies in breast cancer susceptibility genes among AA women with breast cancer were based on small numbers of patients, ranging from 30 to 483 (44–49). Among 213 unaffected women in a US case-control study (44), no BRCA1 mutations were identified, and among 1089 unselected women in the Bahamas (50), only 1 (0.09%) had a mutation. We examined data from the gnomAD database (noncancer gnomAD v2.1) for African ancestry women without cancer; only 3 individuals out of approximately 10 000 screened had a BRCA1 mutation. Similarly, in data from the Exome Aggregation Consortium African ancestry population, with exclusion of The Cancer Genome Atlas cases, no BRCA1 mutations were observed, whereas the prevalence of BRCA2 mutations was 0.16% (51). These very low frequencies are in line with our results. In contrast, 3 of 997 control patients (0.3%) in a Nigerian case-control study (19) had pathogenic mutations in BRCA1, perhaps due to their younger ages and higher proportion of TNBCs.
This study also yielded data suggesting that mutations in ERCC3 and FANCC are associated with increased risk of breast cancer in the AA population. Previous studies of associations between these genes and breast cancer risk were focused on the c.1354C>T, p. Arg452X ERCC3 recurrent mutation in the Ashkenazi Jewish population (52) and the c.355_360delTCTCATinsA mutation in FANCC in EA women (53). However, in the current study, other pathogenic mutations in these genes contributed to the associations. For RECQL, mutations observed in the present study (c.1667_1667 + 3delAGTA) were previously associated with increased risk of breast cancer in a Polish population (54). Furthermore, we noted that the estimated relative risk for mutations in ATM was lower than previous findings in EA populations (2). Given the potential for multiple testing effects, further analyses of these genes in the AA population will be needed to verify the associations with breast cancer risk.
The present study included 1340 women with ER-negative breast cancer, allowing for ER-specific analyses as well as analyses of TNBC. Our results are generally consistent with an earlier report from sequencing of germline DNA from 2148 TNBC patients unselected for family history of breast cancer (55,56) and 8753 TNBC patients subjected to clinical testing (56), most of European ancestry. The present sample was underpowered for assessment of associations of TNBC with mutations in BARD1 and BRIP1, which were reported in the earlier research (56,57).
The major limitation of the present study is sample size. Although there were 5 times as many affected women as in the next largest study of African ancestry breast cancer (19), confidence intervals were wide, preventing certainty about the magnitude of associations. However, inclusion of a sizable number of affected women without a family history of breast cancer was a strength of the study. This allowed estimation of the prevalence of mutations within age and family history strata— information that is critical for establishing genetic testing guidelines for AA women. Although samples were from multiple studies, sequencing of all samples was performed at a single site under uniform conditions. Most study participants came from either population-based breast cancer case-control studies or prospective cohort studies in which affected and unaffected women arose from the same population. All analyses were controlled for study design, first-degree family history of breast cancer, and age.
In summary, there are several key findings from the present study. First, multiple genes previously established as breast cancer susceptibility genes in EA populations are also of importance for breast cancer in AA women. Second, mutations were identified in approximately 2 times as many women with ER-negative breast cancer as compared with women with ER-positive cancer; these findings support the importance of genetic testing in AA women with ER-negative breast cancer or TNBC, which disproportionately occurs in AA women. Finally, mutations in ERCC3, FANCC, and RECQL may be associated with AA breast cancer risk, although further studies are needed to confirm these findings.
Multiple studies have demonstrated that rates of BRCA1 and BRCA2 testing in the United States are substantially lower in AA than EA women (58–62). Disparities in testing are partly driven by differences in recommendations given to AA women, possibly because of misconceptions among physicians about the prevalence of mutations and associated risks in AA women (62). Genetic test results could impact decisions about risk-reducing surgeries or genetic testing of family members. The present results demonstrate, for the first time, the validity and utility of gene-panel testing, beyond BRCA1 and BRCA2, for breast cancer in AA women. Testing will be particularly valuable for women diagnosed with ER-negative and/or TNBC and their families.
Funding
This research was supported in part by National Institutes of Health grants R01CA192393, R01CA225662, P50CA116201, U01CA164974, R01CA098663, R01CA100598, P01CA151135, P30CA16056, U01CA164973, U01CA164920, R01CA204819, R01CA77398, U01CA199277, P30CA014520, U01CA82004, R01CA047147, and R01CA067264; by the American Cancer Society; and by the Susan G. Komen Foundation (JRP, SMD), Breast Cancer Research Foundation (FJC, CBA, JMW, SMD, KLN), and Karin Grunebaum Cancer Research Foundation (JRP).
Notes
Role of funder: The National Institutes of Health and other funders did not have any role in the study design; collection, analysis, or interpretation of data; the writing of the manuscript; or the decision to submit the manuscript for publication.
Conflicts of interest: The authors have no conflicts of interest. Drs. Couch and Domchek have the following disclosures: Fergus Couch—Honoraria/Speakers BureAmbry Genetics, Qiagen, AstraZeneca; Corporate Sponsored Research: GRAIL. Susan Domchek—Honoraria: AstraZeneca, Clovis, BMS; Corporate-Sponsored Research: the University of Pennsylvania has received research funding for clinical trials from Clovis and AstraZeneca.
Acknowledgments; We thank the study participants for their involvement in this research. Pathology data were obtained from several of the following state cancer registries (AZ, CA, CO, CT, DE, DC, FL, GA, IL, IN, KY, LA, MD, MA, MI, NJ, NY, NC, OK, PA, SC, TN, TX, VA); results reported do not necessarily represent their views.
References
Maxwell KN, Domchek SM, Nathanson KL, Robson ME. Population frequency of germline BRCA1/2 mutations. J Clinical Oncol. 2016;34(34):4183–4185.


{kind=link}
{kind=link}