Abstract
Concomitant traumatic injury in the burn patient complicates care coordination and increases morbidity and mortality. The incidence of concomitant injury, however, is uncommon and reported to range from 5–7%. In May 2020, our level 1 trauma center began seeing 40% more patients per month that the 12 months prior. We sought to determine the incidence of concomitant injury in burn patients during this time of increased trauma volume and to examine the associated traumatic injuries in this group.
The burn registry at a single ABA-verified burn center was examined from 5/20–9/20. Patients with concomitant burn and traumatic injury were examined with respect to: %TBSA burn, mechanism of injury, operative interventions, associated traumatic injuries, and length of hospital stay. Continuous data was presented as mean (standard deviation).
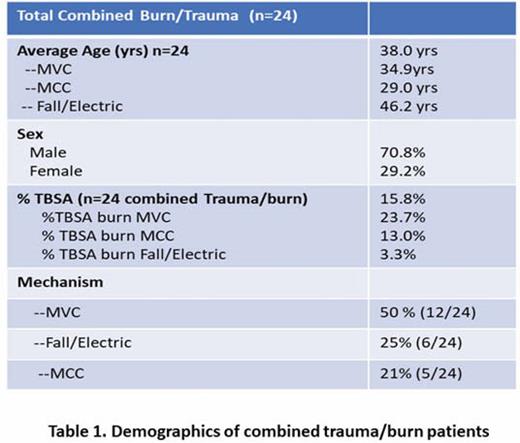
Eighty-nine burn patients were admitted during this period, of whom 24 (26.9%) had concomitant traumatic injuries. The cohort was young and mostly male; the mean TBSA was 16% () (Table 1). The most common mechanism of injury was motor vehicle collision (12 or 50%), followed by fall after high voltage electrical injury (6 or 25%) and motorcycle collisions (5 or 21%).
The most common associated injuries were: pulmonary contusions 29.1% (7/24); long bone fractures 25% (6/24); pelvic/acetabular fractures 20.8% (5/24); femur fractures 16.6% (4/24); and solid organ injury: 16.6% (4/24).
Twenty patients (83.3%) required burn or trauma operative intervention during hospital stay. Of the 20 patients who required operative intervention, 85% underwent burn surgery and 55% underwent trauma surgery (solid organ or orthopedic). Forty percent of these patients required operation for both burn and traumatic injury. In looking specifically at the electric injury group, all six patients required operative intervention for burn injuries, and four required extremity fasciotomy. Patients with electrical injury had a significantly longer hospital stay relative to their TBSA (p< 0.04).
Concomitant trauma and burn injuries are infrequent yet present a major clinical challenge. Our recent increase in overall trauma volume was paralleled by an increase in patients with concomitant burn injuries. The associated traumatic injuries require a multi-disciplinary approach to minimize morbidity and restore function.