






Abstract

To study the influence of sternal transection and costal chondrotomies on the stiffness and stresses in the rib cage of adult patients undergoing Nuss pectus excavatum procedure.
Four pectus excavatum models with different Haller indexes were created by parameterizing a 3D model of a rib cage obtained based on a computed tomography scan of a patient with no pectus deformity. Using the finite element method, insertion of intrathoracic bars into all models was simulated in 3 conditions, namely, non-intervened, transverse sternal section and costal chondrotomies. Stiffness, stress distribution and maximum stresses for each case were obtained and compared.
Transverse sternotomy provided a reduction of 44% to 54% in the stiffness of the rib cage, depending on the Haller index analysed, while chondrotomies promoted a stiffness reduction of 70%. Stress distribution in the rib cage followed similar pattern for all the tested Haller index, but the maximum stress decreased by 36% when performing a transverse sternotomy, whereas when performing costal chondrotomies, it decreased by 47%.
Computational results report that transverse sternotomy reduces appreciably the stiffness of the rib cage, while costal chondrotomies promote even a higher stiffness reduction. Thus, these surgical procedures could improve the clinical outcomes of adult patients undergoing a pectus excavatum repair.
INTRODUCTION
The incidence of pectus excavatum (PE) is about 1 in 1000 children and constitutes more than 87% of all the chest wall deformities [1]. The minimally invasive surgical repair of PE (MIRPE) developed by Nuss et al. [2] is considered to be the gold standard to treat paediatric and young patients with PE due to its excellent cosmetic results. However, the performance of the MIRPE technique in adult patients is controversial. In this subgroup of patients, where the stiffness of the costal cartilage is high, the introduction of the bar is more difficult and produces high stresses in the rib cage [3]. The problems related to high stresses in the thorax can appear immediately or months after the surgery. These problems range from intolerable pain, which can require premature removal of the bar [4], to bar complications such as displacement, which has been reported to occur in 9.5% of all cases, particularly in teenaged patients [5].
Avoiding bar displacement is so relevant that bar stabilization is essential for a successful outcome [6]. In an effort to make the technique both safer and more effective, several modifications have been proposed [7]. These modifications include the introduction and development of new fixation techniques, such as the ‘third point fixation’ [5], modifications of the bar stabilizers or stabilizers position [8], the modelling of the bar [9] or the use of 2 bars [6]. However, there is another way to minimize the displacement or flip tendency of the bar, i.e. to reduce the rib cage stiffness by performing a transverse sternotomy. This procedure is not usually associated with the MIRPE technique, but it has been already applied to facilitate the correction of the deformity and to reduce the probability of bar migration [10–12]. One more extreme way to reduce the stiffness of the rib cage is to perform costal chondrotomies. This procedure is consubstantial with the classic Ravitch technique [13], but, as far as the authors of this research know, it has not been reported in the MIRPE technique, probably because, unless a specific tool is developed, it is a difficult procedure. However, a variation of the MIRPE technique named minor open videoendoscopically assisted repair of pectus excavatum put these chondrotomies into practice [14].
The aim of this paper was to study the influence of the sternal and costal chondrotomies in the stiffness and stresses of the rib cage by finite element analysis of a parametric model of the chest.
MATERIALS AND METHODS
Reconstruction of 3D thoracic model
In this study, several numerical simulations were carried out based on a rib cage of a 35-year-old male adult without PE. In order to have a reference model, all the cases analysed come from the mentioned patient, avoiding the variability of parameters among patients that can make difficult to compare the measured variables. To assess the severity of a PE, the most widely used parameter is Haller index (HI), measured at the level of the osseous end of the sternal body [15]. The chest of the patient, with a non-pathological HI (2.4), was scanned by a clinical computed tomography (VCT 64 c/s, General Electric, Chicago, IL, USA) with a scanning interval of 0.6 mm, and the data were saved as a DICOM file. Then, the data were imported into the Simpleware ScanIP FE Module (Synopsys Inc., Mountain View, CA, USA) to reconstruct the 3D model. Ligaments, muscles and skin were not considered because these elements do not provide appreciable stiffness to the rib cage [16]. Also, the floating ribs were removed due to the same reason. To avoid the influence of asymmetry that would complicate the study and make difficult to draw conclusions, a symmetry operation was performed in the mid-sagittal plane to reproduce the right half symmetric to the left half and the spine was considered as a rigid object and simplified as a cylinder to reduce the amount of calculation, since spine has only slight change after Nuss operation [17].
A parametric model was generated in order to create thoraces with different PE severity, similar to previous simulations [18]. This parametric model allowed to assess the influence of different HI in the stiffness of the rib cage. The rib cortical bone thickness was assumed to be 0.75 mm [19]. Based on the original non-deformed parametric model (Fig. 1), 4 different displacements of the osseous end of the sternal body were used, 30, 47, 65 and 79 mm, creating 3.4, 4.8, 7.2 and 10 HI models, respectively. Finally, the 3D models were saved as Parasolid files and imported into Abaqus 6.14 (SIMULIA, Dassault Systemes, RI, USA) to conduct the finite element analysis.
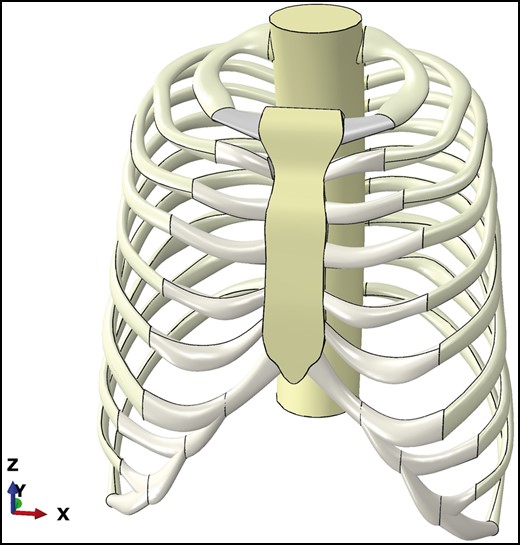
Original non-deformed parametric model (2.4 Haller index).
Finite element analysis
All the rib cage materials were considered isotropic, homogeneous and linear elastic. The material properties of bone and cartilage, Young modulus and Poisson’s ratio, were taken from the literature [20–22]. The spine was assumed to be cortical bone to simulate a rigid body. All contact pairs between anatomic parts were treated as ties: sternum/costal cartilage, costal cartilage/cortical bone, cortical bone/trabecular bone and cartilage/trabecular bone. The spine was considered to be fixed. The type of element selected for the mesh was a 10-node quadratic tetrahedral element (C3D10), after conducting the relevant sensitivity tests.
The simulation was conducted on the assumption that a correction bar was placed at the fifth intercostal space. For each model, a force was applied on the posterior aspect of the sternum, at the point where the bar would be placed, outwards the rib cage in the y-axis direction. The value of the force was the suitable to correct the PE, that is, to revert the displacement imposed to the original model and reach the original 2.4 HI. To mimic the real implantation of the bar, the forces exerted by the bar at the fixation points on the rib were considered. Thus, at the bar attachment points, 2 equal opposite forces summing the same value of the sternal force were also placed. In an iterative process, the force to correct the PE and the maximum principal stresses were calculated. The stiffness was calculated as the relation between the force applied to the sternum and its displacement in the same direction at the point where the HI was measured. The large displacement non-linear solution was used to ensure the accuracy of the simulation results [16, 23].
A total of 12 simulations were carried out, 3 different cases for each of the 4 models. The first case (Fig. 2a) was performed keeping the rib cage integrity, PE; the second case (Fig. 2b) simulated a transverse sternotomy at the second intercostal space, PETS (pectus excavatum with transverse sternotomy); the third case (Fig. 2c) simulated costal cartilage chondrotomies for the third, fourth and fifth ribs at the chondrosternal joints, PECC (pectus excavatum with costal chondrotomies).
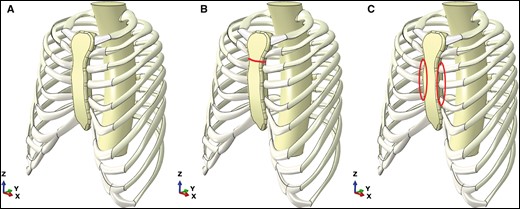
The 3 different cases for the 4.8 Haller index model, showing in red the sternal osteotomy or the chondrotomies. (A) Pectus excavatum, (B) pectus excavatum with transverse sternotomy and (C) pectus excavatum with costal chondrotomies.
RESULTS
Force required to elevate the sternum to correct PE, stiffness and maximum principal stress are shown in Table 1. The force and stiffness reduction when performing the transverse sternotomy was 44% for 3.4 HI and 54% for the other 3 HI values. However, the reduction when performing the costal chondrotomies was not affected by the HI and was of 70% for all the HI values.
Results of the models obtained in the analyses
| Rib Cage Model | HI | Force (N) | Stiffness (N/mm) | Maximum Principal Stresses (MPa) |
|---|---|---|---|---|
| PE | 3.4 | 149 | 4.93 | 59 |
| 4.8 | 186 | 3.93 | 73 | |
| 7.2 | 195 | 2.97 | 76 | |
| 10 | 202 | 2.54 | 81 | |
| PETS | 3.4 | 83 | 2.75 | 38 |
| 4.8 | 85 | 1.79 | 50 | |
| 7.2 | 90 | 1.37 | 56 | |
| 10 | 92 | 1.16 | 65 | |
| PECC | 3.4 | 45 | 1.49 | 31 |
| 4.8 | 54 | 1.14 | 42 | |
| 7.2 | 58 | 0.88 | 49 | |
| 10 | 61 | 0.77 | 57 |
| Rib Cage Model | HI | Force (N) | Stiffness (N/mm) | Maximum Principal Stresses (MPa) |
|---|---|---|---|---|
| PE | 3.4 | 149 | 4.93 | 59 |
| 4.8 | 186 | 3.93 | 73 | |
| 7.2 | 195 | 2.97 | 76 | |
| 10 | 202 | 2.54 | 81 | |
| PETS | 3.4 | 83 | 2.75 | 38 |
| 4.8 | 85 | 1.79 | 50 | |
| 7.2 | 90 | 1.37 | 56 | |
| 10 | 92 | 1.16 | 65 | |
| PECC | 3.4 | 45 | 1.49 | 31 |
| 4.8 | 54 | 1.14 | 42 | |
| 7.2 | 58 | 0.88 | 49 | |
| 10 | 61 | 0.77 | 57 |
PE: pectus excavatum; PETS: pectus excavatum with transverse sternotomy; PECC: pectus excavatum with costal chondrotomies.
Results of the models obtained in the analyses
| Rib Cage Model | HI | Force (N) | Stiffness (N/mm) | Maximum Principal Stresses (MPa) |
|---|---|---|---|---|
| PE | 3.4 | 149 | 4.93 | 59 |
| 4.8 | 186 | 3.93 | 73 | |
| 7.2 | 195 | 2.97 | 76 | |
| 10 | 202 | 2.54 | 81 | |
| PETS | 3.4 | 83 | 2.75 | 38 |
| 4.8 | 85 | 1.79 | 50 | |
| 7.2 | 90 | 1.37 | 56 | |
| 10 | 92 | 1.16 | 65 | |
| PECC | 3.4 | 45 | 1.49 | 31 |
| 4.8 | 54 | 1.14 | 42 | |
| 7.2 | 58 | 0.88 | 49 | |
| 10 | 61 | 0.77 | 57 |
| Rib Cage Model | HI | Force (N) | Stiffness (N/mm) | Maximum Principal Stresses (MPa) |
|---|---|---|---|---|
| PE | 3.4 | 149 | 4.93 | 59 |
| 4.8 | 186 | 3.93 | 73 | |
| 7.2 | 195 | 2.97 | 76 | |
| 10 | 202 | 2.54 | 81 | |
| PETS | 3.4 | 83 | 2.75 | 38 |
| 4.8 | 85 | 1.79 | 50 | |
| 7.2 | 90 | 1.37 | 56 | |
| 10 | 92 | 1.16 | 65 | |
| PECC | 3.4 | 45 | 1.49 | 31 |
| 4.8 | 54 | 1.14 | 42 | |
| 7.2 | 58 | 0.88 | 49 | |
| 10 | 61 | 0.77 | 57 |
PE: pectus excavatum; PETS: pectus excavatum with transverse sternotomy; PECC: pectus excavatum with costal chondrotomies.
Stress distribution in the rib cage follows similar pattern for all the tested HI. Figure 3 shows the stress distribution for the 3 cases of the 4.8 HI model. The areas where the maximum stresses were located were always the back ends of the sixth ribs for the PE and PETS models, and the lateral parts of the sixth and seventh ribs for the PECC. The maximum stress increased with the HI within the same case (PE, PETS or PECC), but it decreased by 36% (HI 3.4) or by 20% (HI 10) when performing a transverse sternotomy. In the case of costal chondrotomies, the reduction of maximum stress was 47% for HI 3.4 and 30% for HI 10.
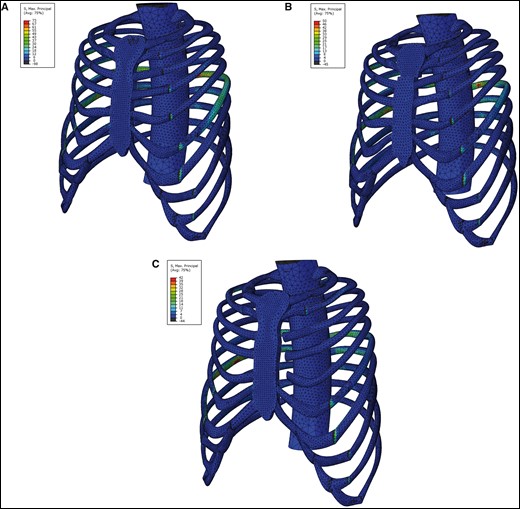
Stress distribution (MPa) in the rib cage after corrective surgery. (A) Pectus excavatum model, (B) pectus excavatum with transverse sternotomy model and (C) pectus excavatum with costal chondrotomies model.
DISCUSSION
The MIRPE is the gold standard technique for paediatric patients [24, 25], although still controversial in adult patients since in these patients, high stresses occur because their costal cartilages are less flexible than those of paediatric patients, and the risk of failure is higher [3]. Therefore, a reduction of the stiffness in the rib cage seems to be an interesting option prior to the insertion of the pectus bar. This reduction of the needed force to raise the sternum enhances the bar stability and is also related to less postoperative pain [9].
Two different procedures to reduce the rib cage stiffness were analysed in this study, namely, transverse sternotomy and costal chondrotomies. The results showed that both procedures produce an appreciable reduction in the rib cage stiffness, minimizing therefore the force to be exerted by a corrective PE bar. To our knowledge, no clinical study has evaluated the reduction in force required to elevate the sternum before and after performing a transverse sternotomy exclusively. The biomechanical rib cage model simulated showed that a transverse sternotomy promotes stiffness reduction from 44% to 54%, depending on HI. Performing transverse sternotomy is not a usual procedure in minimally invasive repairs for chest wall surgical correction, but it has been reported as a feasible and not technically challenging procedure [11, 12]. This means that with a relatively simple incision that produces a small scar, the stiffness can be significantly reduced, reaching higher surgical safety and decreasing further complications. Consequently, based on the results of this study, a routinely transverse sternotomy for adult patients is suggested.
Simulated costal chondrotomies showed that, despite the high stiffness of the rib cage in adult patients, such stiffness can be reduced by 70%. This result is similar to previous clinical data showing that the average force required to elevate the sternum (patients over 19 years old, 5.6 mean HI) was 183 N before a subperichondrial partial costal cartilage excision, and 45 N after it, resulting in a force reduction of 75% [26]. Another clinical study [27] showed a 44% reduction in stiffness when performing costal chondrotomies, but such reduction could be due to the fact that an inferior number of chondrotomies were carried out. However, performing costal chondrotomies while maintaining a minimally invasive surgical technique is very challenging, and unless a safe tool or technique is developed, a semi-open surgery is suggested in the case of very stiff rib cage. Accordingly, the surgeon should consider whether a technique like minor open videoendoscopically assisted repair of pectus excavatum could be the solution or not since, on the one hand, this procedure facilitates the surgery, but on the other hand, it produces more scars [14].
The simulations also showed that increasing the HI in a rib cage with PE led to an increment in the amount of force required to elevate the sternum, but not in a proportional manner. Thus, an increase in HI from 3.4 to 7.2 (112%) would only change the required force from 149 to 195 N (31%). However, it is remarkable that the percentage of reduction in the stiffness of the rib cage when performing a transverse sternotomy is slightly affected by the HI (44% to 54% from 3.4 HI to 10 HI), and no affected at all when performing costal chondrotomies (70% of reduction for all HI tested). Therefore, the decision of performing osteotomy, chondrotomies or none of both, should not be affected by the HI, but because the initial stiffness of the rib cage.
PE models showed the stress distribution that will appear after an MIRPE if no reduction of stiffness were carried out. It is shown that the higher the HI, the higher the maximum stress, but again, as in the force required, not in a proportional manner. However, the pattern of stress distribution in these models was quite similar regardless of the HI, presenting the maximum stress at the backends of the sixth ribs for the PE and the PETS models, and the lateral parts of the sixth and seventh ribs for the PECC. The maximum stress is related to postoperative pain [3], so reducing stress is also a goal in any type of PE repair. One way to reduce stresses, and consequently postoperative pain, can be achieved by using 2 bars in the MIRPE technique [4]. However, 2 bars cause difficulties for their insertion and extraction in performing the technique [28]. The maximum stress reduction achieved in this study was of 36% in the case of transverse sternotomy and of 47% in the case of costal chondrotomies, both for HI 3.4. Again, costal chondrotomies had the best performance from a biomechanical point of view, but not from the aesthetic outcomes if a minor open videoendoscopically assisted repair of pectus excavatum is needed.
Limitations
This study has some limitations, and the most important one is that no clinical serial data are available. However, the aim of this study is to give surgeons suggestions about performing stiffness reduction in the rib cage when performing an MIRPE. Another limitation is that the rib cage anatomy, the costal cartilages and the ribs and sternum mechanical properties vary widely between patients, so the results of this study must be considered not in absolute values, but as a tendency when performing transverse sternotomy or costal chondrotomies.
CONCLUSION
The results of this paper suggest that the transverse sternotomy is a key factor to improve the MIRPE technique because with a relatively simple incision in the rib cage, its stiffness is significantly reduced, and consequently the displacement tendency of the implanted bar and the postoperative pain are also reduced. Furthermore, performing costal chondrotomies reduces even more than with transverse sternotomy the stiffness of the rib cage, but surgeons must evaluate the clinical and aesthetic impact of the extra incisions needed to perform this improvement and decide at their discretion what procedure is more suitable for each type of patient.
Conflict of interest: none declared.
Author contributions
Ángel Gabriel Vega-Artiles: Investigation; Software; Writing—original draft; Writing—review & editing. David Pérez: Conceptualization; Supervision; Writing—review & editing. Oscar Martel: Conceptualization; Methodology; Writing—original draft; Writing—review & editing. Alberto Cuadrado: Investigation; Methodology; Software. Alejandro Yánez: Conceptualization; Supervision; Writing—original draft.
Reviewer information
Interactive CardioVascular and Thoracic Surgery thanks Toru Bando, Mohsen Ibrahim and the other anonymous reviewer(s) for their contribution to the peer review process of this article.
REFERENCES
ABBREVIATIONS
- HI
Haller index
- MIRPE
Minimally invasive surgical repair of pectus excavatum
- PE
Pectus excavatum
- PECC
Pectus excavatum with costal chondrotomies
- PETS
Pectus excavatum with transverse sternotomy

{kind=link}
{kind=link}
{kind=link}
{kind=link}