






CLINICAL PROBLEM
Open repair is the gold standard with which to compare any surgical alternative therapy for aortic arch diseases. Arch open repairs necessitate the use of cardiopulmonary bypass and usually prolonged periods of hypothermic circulatory arrest. However, many patients with aortic arch disease are too sick to support these morbid operations.
CASE DESCRIPTION
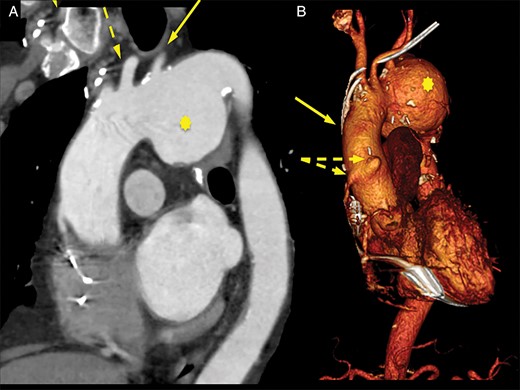
(A) Oblique sagittal reconstruction shows the pseudoaneurysm (asterisk), LSA (solid arrow) and LCCA (dashed arrow). (B) Three-dimensional reconstruction shows the relationship between the aortocoronary grafts (dashed arrows) and the BCT (solid arrow).
Preoperative 3D reconstruction of the arch pseudoaneurysm.
The patient, as other significant comorbidities, presented severe peripheral arterial disease with previous surgery on the abdominal aorta, previous coronary artery bypass grafting with two aortocoronary saphenous vein bypass grafts and two internal thoracic artery grafts, including a patent left internal mammary artery to left anterior descending artery, and severe left ventricle dysfunction. The patient's logistic EuroSCORE was 64.52%.

{kind=link}