






Abstract
Giant coronary artery aneurysm is a rare clinical entity and its involvement in the interatrial space is extremely rare. We here report the rare surgical case of a 67-year old man with giant right coronary artery aneurysm located in the atrial septum with fistula formation to the right atrium, complicated with congestive heart failure, rapid atrial fibrillation and left atrial appendage thrombus. The patient eventually recovered fully without sequelae.
INTRODUCTION
Giant coronary artery aneurysm is a rare clinical entity and its operative indication and procedures are controversial. We describe a case of giant right coronary artery aneurysm located in the atrial septum, with fistula formation to the right atrium in a 67-year old man who underwent surgical correction.
CASE REPORT
A 67-year old man was admitted with worsening orthopnoea. He had been diagnosed with an asymptomatic right coronary artery aneurysm 7 years before (Fig. 1A and B), but had declined further examination and treatment. He had undergone no follow-up examinations of the aneurysm since then.
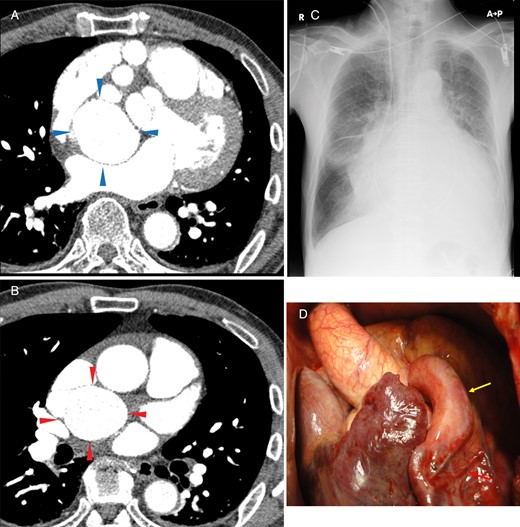
(A and B) Contrast-enhanced CT revealed two large masses. (A) Proximal aneurysm: dorsal to the right atrium and ventral to the left atrium, shown by blue arrows. (B) Distal aneurysm: dorsal to the superior vena cava and cranial to the right pulmonary artery, shown by red arrows. The abnormal vascular connections are not clearly understood because of the vessel tortuosity. (C) Preoperative chest X-ray showed a cardiothoracic ratio of 76%. (D) Intraoperative findings through median sternotomy. The dilated proximal right coronary artery and the right ventricle branch are shown by the yellow and red arrows, respectively.
On auscultation, a mild continuous murmur was heard at the right sternal border. Electrocardiography revealed atrial fibrillation and a heart rate of 140–150 bpm. Chest X-ray revealed a cardiothoracic ratio of 76% and pulmonary congestion (Fig. 1C). Transthoracic echocardiography showed a left ventricular ejection fraction of 76% using the modified Simpson's biplane method. Transoesophageal echocardiography showed an enlarged right coronary artery, a large interatrial mass of 60 × 50 mm with a fistula to the right atrium (Fig. 2A and B; Video 1), moderate tricuspid regurgitation, a small thrombus in the left atrial appendage (LAA) and pericardial and pleural effusion.
Video 1:Preoperative transoesophageal echocardiography showed a large mass of 60 × 50 mm in the interatrial space with a fistula to the right atrium. Preoperative coronary angiography at two angles (LAO30°–CRA0°, RAO30°–CRA0°) showed that the branched artery extending towards the interatrial space was enlarged. The outflow of the aneurysm or another abnormal vascular connection was not clearly detected.
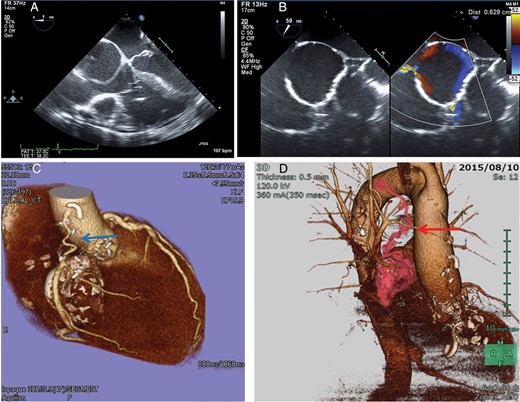
(A and B) Preoperative transoesophageal echocardiography showed a large mass of 60 × 50 mm in the interatrial space with a fistula to the right atrium. The size of the fistula was 6.3 mm. (C) Postoperative three-dimensional CT coronary angiography showed patent aortocoronary bypass of the radial artery conduit, shown by blue arrow. (D) Postoperative three-dimensional CT angiography demonstrated a residual abnormal vascular connection to the distal aneurysm from the bronchial artery, shown by red arrow.
Coronary angiography demonstrated that the proximal right coronary artery was dilated, and it gave off a tortuous branch to the atrial septum that was markedly dilated with a fistula to the right atrium (Video 1). However, neither outflow of the aneurysm nor another abnormal vascular connection was clearly visualized because of tachycardia and the very large aneurysm size of itself. The distal right coronary artery and left coronary artery appeared normal. We did not perform contrast-enhanced CT because of the uncontrollable rapid atrial fibrillation.
On the basis of these findings, a tentative diagnosis of right coronary artery dilatation and a giant aneurysm with fistula formation to the right atrium was made. Concomitant congestive heart failure, rapid atrial fibrillation and LAA thrombus necessitated urgent surgical intervention.
Surgery was performed through a median sternotomy (Fig. 1D) with usual cardiopulmonary bypass, cardiac arrest with antegrade and retrograde cardioplegia infusion. The dilated proximal right coronary artery was removed and the ostium was closed. After right atriotomy, a 6-mm-diameter communication was found between the roof of the right atrium and the aneurysmal branch. The aneurysm was removed en bloc with a part of the right atrium and interatrial septum; therefore, we reconstructed them with an autologous pericardium patch. The orifice of the distal aneurysm was ligated but not removed because of severe adhesion and poor orientation. We added aortocoronary bypass with a radial artery graft to the mid-right coronary artery (Fig. 2C), tricuspid annuloplasty with an Edwards 30-mm MC3 ring (Edwards Lifesciences, Inc., Irvine, CA, USA), Maze procedure and removal of the LAA.
The patient was smoothly weaned from cardiopulmonary bypass. Postoperative pathological examination of the aneurysm wall revealed severe atheromatous and fibrotic changes in the vessel structure.
The patient recovered completely with no tricuspid regurgitation and maintained a sinus rhythm. Postoperative CT angiography demonstrated an abnormal vascular connection from the bronchial artery to the ligated distal aneurysm (Fig. 2D). We performed coil embolization of the bronchial artery, and the patient was discharged after rehabilitation on postoperative day 25.
DISCUSSION
Giant coronary artery aneurysms exceeding 20 mm in diameter are extremely rare, with a reported incidence rate of 0.02% of patients who undergo cardiac surgery [1]. The proximal right coronary artery is often involved, and the area surrounding the atrium is the most frequent site of aneurysm development [2, 3]. Even on the basis of these previously published reports, few reports have described giant coronary aneurysms located in the atrial septum with fistula formation to the right atrium.
In the present case of a coronary aneurysm in a patient with congestive heart failure, we surgically removed the aneurysm and performed coronary artery bypass grafting, tricuspid annuloplasty and the Maze procedure. Because the patient's preoperative condition was not suitable for obtaining detailed information about the aneurysm and its connection with coronary and other arteries, we found another communicating artery to the aneurysm postoperatively and added the radiological intervention. As a result, we obtained a favourable outcome.
ACKNOWLEDGEMENTS
The authors thank Hiroshi Morishita of the Morishita Heart Clinic for providing the CT images.
Conflict of interest: none declared.

{kind=link}
{kind=link}