






Abstract
Cowden syndrome is a phosphatase and tensin homologue on chromosome ten (PTEN) hamartoma tumour syndrome. The loss of function of the PTEN protein is associated with the risk of development and progression of several types of tumours, such as pulmonary neuroendocrine tumours and carcinoids. We present a 65-year old male non-smoker, who was diagnosed with Cowden syndrome and had a pulmonary tumour. He underwent wedge resection via video-assisted thoracoscopic surgery and was histopathologically diagnosed with an atypical carcinoid. To our knowledge, this is the first report on a pulmonary atypical carcinoid in a patient with Cowden syndrome. The present findings suggest a potential link between phosphoinositide-3 kinase/protein kinase B signalling in Cowden syndrome and the development of pulmonary neuroendocrine tumours, such as carcinoids.
INTRODUCTION
Cowden syndrome—an inherited autosomal dominant disease—is a phosphatase and tensin homologue on chromosome ten (PTEN) hamartoma tumour syndrome [1]. The PTEN gene is a tumour suppressor gene located on human chromosome 10q22–23 and induces apoptosis, proliferation, migration and angiogenesis by interfering with phosphoinositide-3 kinase/protein kinase B (PI3K/Akt) signalling. PI3K/Akt signalling is over-activated in many types of tumours, including carcinoids [2]. Thus, Cowden syndrome is characterized by a high risk of both benign and cancerous tumours of the breast, thyroid, endometrium and colorectum. Some reports have described cases of neuroendocrine tumours, such as skin neuroendocrine tumours, in patients with Cowden syndrome [3]. Here, we present a patient with Cowden syndrome, who had a pulmonary carcinoid. To our knowledge, this is the first report on a pulmonary atypical carcinoid in a patient with Cowden syndrome.
CASE
A 65-year old male non-smoker, who was genetically diagnosed with Cowden syndrome ∼20 years previously, presented to the Osaka General Hospital of West Japan Railway Company with a pulmonary lesion that was increasing in size. He had undergone resection of papillomas on the tongue, transcatheter embolization of brain arterio-venous fistulae, laser therapy for cutaneous lesions and periodic endoscopic examinations for gastrointestinal lesions (Fig. 1A and B). His other manifestations of Cowden syndrome included a thyroid follicular tumour and macrocephaly (head circumference, 63 cm). His son was also genetically diagnosed with Cowden syndrome.

(A) The nose showing cutaneous facial papules. (B) Gastrointestinal endoscopy showing multiple hamartomas of the oesophagus. (C and D) Computed tomography scans at 6 years previously and during the current presentation, showing a solid tumour mass in the left inferior lobe of the lung that slowly grew in size.
Six years previously, computed tomography showed a round, 9-mm nodule in the lower left lobe of the lung (S6c), which progressively grew into a lobulated 14-mm nodule (Fig. 1C and D). We considered lobectomy and segmentectomy; however, we selected wide wedge resection because he had underlying diseases such as ischaemic heart disease. He underwent wedge resection via video-assisted thoracoscopic surgery. It was necessary to pull the tumour away from the inter-lobar pulmonary artery, as the tumour was present in the central parenchyma. We dissected the oblique fissure to expose the inter-lobar pulmonary artery and ligated the superior segmental artery. The tumour was grasped with ring-shaped forceps and completely excised with staplers, maintaining a surgical margin of ∼15 mm, which was similar to the tumour diameter. The tumour showed a yellowish round nodular configuration. He was discharged from the hospital 5 days after surgery, without any complications.
The histopathological findings of the tumour are presented in Fig. 2. The tumour included cells that had ovoid to round nuclei, were arranged in an alveolar pattern and were of different sizes. Some of the cells were arranged in a trabecular pattern. Immunohistochemical analysis revealed cytoplasmatic expression of synaptophysin, plasma membrane-associated expression of the neural cell adhesion molecule and a Ki-67 labelling index of 14%. The tumour exhibited 5 mitoses per 10 high-power fields, and areas of tumour necrosis were identified. Based on the results of a tissue morphology examination using haematoxylin–eosin staining, and the immunohistochemical expression profile, a diagnosis of a carcinoid with atypical features was made. He is being carefully monitored and followed, without any additional treatment, while considering his underlying diseases.
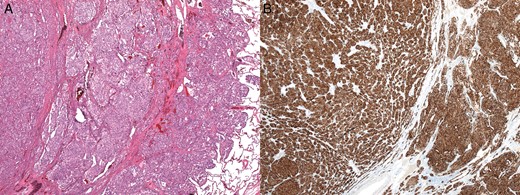
(A and B) Histopathological findings. On microscopic examination, the tumour cells are arranged in an alveolar pattern and are immune-positive for synaptophysin.
DISCUSSION
Cowden syndrome was first described in 1963 by Lloyd and Dennis as a dominantly inherited disease that is associated with increased risks for benign and malignant tumours [1]. Cowden syndrome reportedly affects approximately one in every 200 000 individuals, according to a statement issued by the National Comprehensive Cancer Network. The PTEN gene is a tumour suppressor gene and induces PI3K/Akt signalling. The loss of function of the PTEN protein is associated with the risk of development and progression of several types of tumours, such as pulmonary neuroendocrine tumours [4] and carcinoids [2]. There are few reports about the relationship between carcinioids and the PTEN protein. One report showed that decreased PTEN expression may be related to age in patients with carcinoids [2], and another report showed that carcinoids with reduced PTEN expression have a high metastatic potential [5]. Further studies are needed to determine the relationship between Cowden syndrome and carcinoids. Given the high risk of malignancy in patients with Cowden syndrome, cancer surveillance of the whole body is one of the most important medical management steps in these patients. Although cases of benign thoracic nodules, such as hamartomas, have already been described in Cowden syndrome, it is essential to consider neuroendocrine tumours, including pulmonary carcinoids, in the differential diagnosis.
We described a unique case of an atypical pulmonary carcinoid in a patient with Cowden syndrome. The current findings suggest a potential link between PI3/Akt signalling in Cowden syndrome and the development of pulmonary neuroendocrine tumours, including carcinoids.
Conflict of interest: none declared.

{kind=link}
{kind=link}