






Abstract
This report presents an extremely rare case of a rapidly growing giant pericardial cyst which was surgically removed 20 years after the first detection. A 38-year-old asymptomatic male was referred because of rapidly growing mass on the right diaphragm. This lesion was detected about 20 years earlier and checked by a chest roentgenogram once a year. However, this lesion showed rapid growth over the last year, therefore surgical removal was performed. A pathological examination revealed this lesion as a giant pericardial cyst without inflammatory, hemorrhage or malignant cells. Therefore, there was no pathological explanation for the rapid growth of this cyst. In conclusion, general thoracic surgeons should be aware of the possibility of rapid growth, even if the diagnosis is a pericardial cyst.
1. Introduction
Pericardial cysts are caused by an incomplete coalescence of fetal lacunae during the development of the pericardium. The estimated incidence of pericardial cyst is 1:100,000 and it represents 6–7% of all mediastinal masses [1, 2]. These cysts are usually unilocular and have thin and translucent wall lined by endothelium or mesothelium, containing a clear serous fluid. In addition, the natural history of the pericardial cyst is unknown.
Most cases are asymptomatic, however, some patients complain of chest pain, dyspnea, or paroxysmal tachypnea, due to the pressure of the surrounding organs [1–3]. Most happen to be found by medical checkup, and a roentgenogram shows a round homogeneous radiodense lesion at the cardiophrenic angle, which is most likely to occur in the right cavity. In principle, a pericardial cyst only requires follow-up, however, growing cases or symptomatic cases require surgical removal.
This report herein presents a rare case of rapidly growing giant pericardial cyst 20 years following its detection.
2. Case
A 38-year-old asymptomatic male had a 20-year's history of chest roentgenogram abnormality (Fig. 1f ). The patient was found to have a giant pericardial cyst in the right side of the heart; however, the size showed no change. However, this lesion showed a rapid growth over the last year, therefore, the patient was admitted for an investigation of evidence of malignancy. Fig. 1 shows the time course of the roentgenogram over 20 years. Chest roentgenogram revealed a rounded mass in the right cardiophrenic angle. From 1990 to 2006 (Fig. 1a–d), the size of this lesion showed no change. However, this lesion showed sudden growth in the roentgenogram of 2008 (Fig. 1e). Magnetic resonance imaging (MRI) showed the presence of a giant mass, measuring 12 cm in diameter and the internal density of this lesion was equivalent to that of water. Although the findings of the MRI showed this lesion to be a benign cystic lesion, surgical removal was considered due to the rapidly growing characteristics, which indicated the possibilities of inflammation, hemorrhaging or malignant transformation. The patient was referred to undergo surgical treatment of this cyst, and this lesion was resected by video-assisted thoracic surgery. The cyst, measuring 12×10 cm in diameter, did not adhere to either the lung or diaphragm. The cyst was connected to the inferior pericardial surface only by a thin pedicle. After this pedicle was ligated and cut, the cyst was completely removed. The lesion was a cystic lesion with a thin wall and filled with about 200 ml of clear serous fluid (Fig. 2a ). An intraoperative examination revealed this fluid to contain neither inflammatory, hemorrhage nor malignant cells. The cystic lesion (hematoxylin and eosin stain, 40×) was composed of a single layer of mesothelial cells and collagenous tissue without inflammatory, hemorrhage or malignant cells (Fig. 2b). These features were compatible with a benign pericardial cyst. The patient had an uneventful postoperative recovery without any complications.
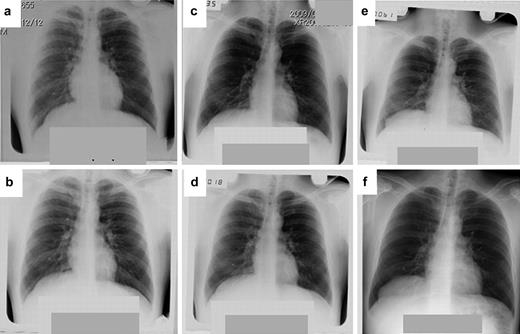
The time course of the 20-year natural history of chest roentgenogram in the giant pericardial cyst. (a) 1990, (b) 1995, (c) 2005, (d) 2006, (e) 2008 and (f) 2009.

(a) The macroscopic appearance of the giant pericardial cyst filled with clear serous fluid. (b) The cystic lesion (hematoxylin and eosin stain, 40×) consisted of a single layer of mesothelial cells and collagenous tissue. The features are compatible with a pericardial cyst. There is no evidence of malignancy.
3. Discussion
Pericardial cysts are uncommon congenital abnormalities and they usually have a diameter ranging from 1 to 5 cm [1, 4]. Pericardial cysts with a diameter over 10 cm are known as ‘giant pericardial cysts’, and they are extremely rare.
Most pericardial cysts are asymptomatic. Some patients with giant pericardial cysts, including the present case, are also asymptomatic [5]. However, some cases have demonstrated life-threatening complications [1–3]. Nina et al. reported a case of a cyst measuring 13 cm in size with symptom, such as progressive dyspnea, right-sided chest pain and dry cough due to mediastinal compression [1]. McMillan et al. presented a case complicated by a pericarditis [2] and Lesniak-Sobelga et al. also showed a case compressing the right ventricle [3].
The treatment of a symptomatic or growing giant pericardial cyst is surgical removal [1–3, 5]. The cyst in the present case also was successfully removed by video-assisted thoracic surgery. This cyst was initially thought to either be infected, hemorrhaged or to have transformed into a neoplasm. However, there was neither evidence of inflammation, hemorrhage, nor any malignancy in this cyst. Therefore, no pathological explanation could be found for the rapid growth of this cyst.
The natural history of a giant pericardial cyst is unknown in detail. Therefore, the present case is the extremely rare case with a natural history of 20 years. Although the cyst in this case had shown no change over about 18 years, a rapid growth was suddenly observed between the roentgenogram obtained in 2008 and 2009. This was not proven pathologically, however, careful observation is necessary whenever a pericardial cyst is being followed up.
In conclusion, this report presented the case of a rapidly growing giant pericardial cyst with a long natural history. General thoracic surgeons should therefore be aware of the possibility of a sudden rapid growth of such cysts without any definite reason, even if the diagnosis is a pericardial cyst.
We thank Brian Quinn for critical comments on the manuscript.

{kind=link}
{kind=link}