





Abstract
3D electroanatomical mapping is beneficial in accessory pathway ablation for better delineation of the anatomy, less procedure and fluro time, it depends on point-by-point mapping to identify the connection sites of the accessory pathway (AP) to the atria or ventricle, or the site of the AP potential. However, this approach requires an accurate interpretation of the local electrograms. In contrast, open window mapping (OWM) doesn’t need to differentiate the signals site of origin, it is based on an automatic annotation process in which the signals with the highest -dV/dt are annotated at each obtained point irrespective of the cardiac chamber. (1) Few reports describe the additional benefit of such technique in patients with complex congenital heart diseases. (2)
To present our centre experience in using OWM technique in addition to early meets late (EML) algorism in accessory pathway ablation especially in patients with complex congenital heart disease or previous failed ablation trials.
We reviewed patients who underwent AVRT ablation at our centre from August 2022 to August 2023 with emphasis on cases mapped using OWM & EML techniques using high density mapping catheters. Demographic data, clinical presentation, resting & tachycardia ECGs, and Echo reports were examined thoroughly, additionally, we revised the 3D maps, ablation details, fluro dose, and outcomes of the procedures.
Over one year, among 74 patients underwent AVRT ablation, open window mapping was used in 4 patients with manifest preexcitation (Rt posteroseptal in 3 of them & Rt free wall in one patient). Among the four patients: 3 were pediatrics, youngest was 5 years old, 19 Kg, 2 patients had previous failed ablation trials, their Echo reports revealed severe form of Ebstein anomaly with large ASD in the first patient, case 2 had single ventricle physiology with bidirectional Glenn while the two other patients had structurally normal heart (Table). The mapping using the OW & EML techniques confirmed the site of AP breakthrough conduction at Rt posteroseptal area in 3 of them and Rt posterolateral area in the remaining one, ablation resulted in immediate loss of preexcitation with no recurrence in all patients. Average fluro dose was 0.1 Gy which is significantly lower than the average dose in the remaining AVRT cases. Over median follow up period of 9 months, there were no recurrence of the accessory pathways & no complications.
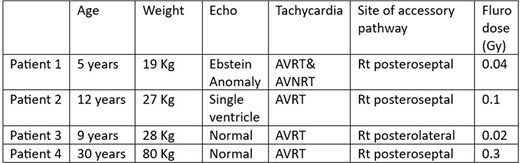
Demographic, ECG, Echo & procedure data
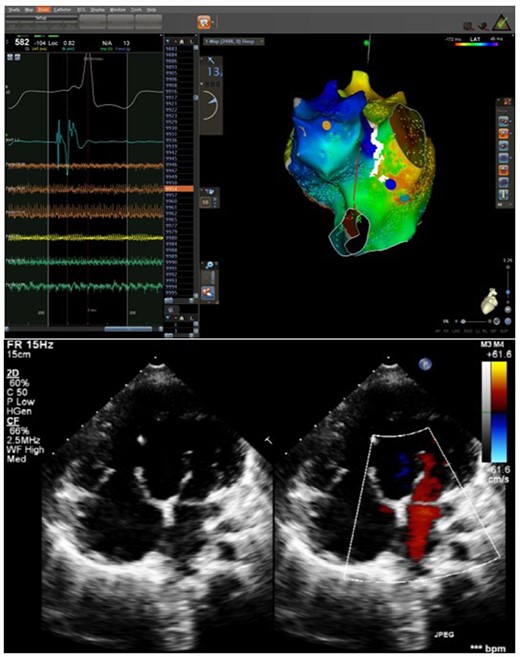
3D map & Echo in patient 2
Author notes
On behalf of AHC team
Funding Acknowledgements: Type of funding sources: None.

{kind=link}