





Abstract
Electrical cardioversion is commonly used to restore sinus rhythm in patients with atrial fibrillation (AF), but procedural technique and clinical success vary. We sought to identify techniques associated with electrical cardioversion success for AF patients.
We searched MEDLINE, EMBASE, CENTRAL, and the grey literature from inception to October 2022. We abstracted data on initial and cumulative cardioversion success. We pooled data using random-effects models. From 15 207 citations, we identified 45 randomized trials and 16 observational studies. In randomized trials, biphasic when compared with monophasic waveforms resulted in higher rates of initial [16 trials, risk ratio (RR) 1.71, 95% CI 1.29–2.28] and cumulative success (18 trials, RR 1.10, 95% CI 1.04–1.16). Fixed, high-energy (≥200 J) shocks when compared with escalating energy resulted in a higher rate of initial success (four trials, RR 1.62, 95% CI 1.33–1.98). Manual pressure when compared with no pressure resulted in higher rates of initial (two trials, RR 2.19, 95% CI 1.21–3.95) and cumulative success (two trials, RR 1.19, 95% CI 1.06–1.34). Cardioversion success did not differ significantly for other interventions, including: antero-apical/lateral vs. antero-posterior positioned pads (initial: 11 trials, RR 1.16, 95% CI 0.97–1.39; cumulative: 14 trials, RR 1.01, 95% CI 0.96–1.06); rectilinear/pulsed biphasic vs. biphasic truncated exponential waveform (initial: four trials, RR 1.11, 95% CI 0.91–1.34; cumulative: four trials, RR 0.98, 95% CI 0.89–1.08) and cathodal vs. anodal configuration (cumulative: two trials, RR 0.99, 95% CI 0.92–1.07).
Biphasic waveforms, high-energy shocks, and manual pressure increase the success of electrical cardioversion for AF. Other interventions, especially pad positioning, require further study.
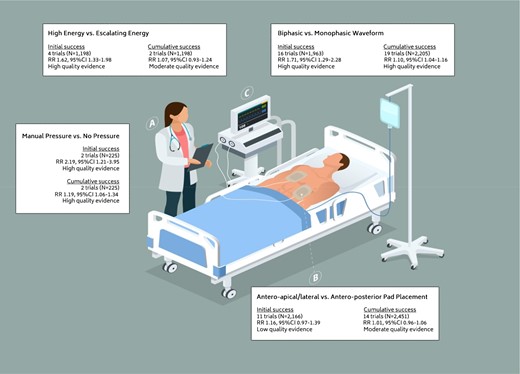
Current guidelines provide limited guidance on how to perform electrical cardioversion, but our systematic review shows that clinicians can apply biphasic waveforms, high-energy (≥ 200J) shocks, and manual pressure to increase the likelihood of sinus rhythm conversion following atrial fibrillation.
The effect of pad positioning on electrical cardioversion success is currently indeterminate. Pad placement should be studied in conjunction with two other techniques known to be effective (i.e. maximal energy and biphasic shocks) for cardioversion success.
Introduction
Atrial fibrillation (AF) is the most common arrhythmia and is associated with increased morbidity, mortality, and healthcare costs.1–3 The prevalence and incidence of AF are increasing. An estimated 6–16 million people will have AF in the USA by 2050 and around 14 million people in Europe will have AF by 2060.4 Electrical cardioversion is a common procedure for patients with AF to restore sinus rhythm, alleviate symptoms, and delay disease progression.5–8 Reported acute success rates of electrical cardioversion range from 50 to 90%.9–15 Electrical cardioversion has multiple modifiable components, including waveform phases, shock energy, pad positioning, manual pressure, and the use of adjunct medications.14 Differences in technique may explain some of the variability in procedural success. Clinical practice guidelines provide limited guidance on how to perform electrical cardioversion.5–8 The available evidence on interventions needs to be collated, appraised, and summarized to inform clinical practice and identify directions for future research.
This systematic review and meta-analysis aimed to compare rates of successful electrical cardioversion of AF using different techniques.
Methods
We pre-registered the protocol with Open Science Framework (DOI:10.17605/OSF.IO/FTU57).16 We list the differences between the registered and final protocol in see Supplementary material online, Appendix S1.
Search strategy
We searched CENTRAL, MEDLINE, and EMBASE from inception to October 2022 and searched the grey literature.16 An academic librarian reviewed the search strategies (see Supplementary material online, Appendix S2).
Eligibility criteria
We included randomized controlled trials and comparative observational studies evaluating the efficacy of a non-pharmacological intervention in patients with AF undergoing electrical cardioversion. We excluded studies where AF was induced and studies focused on atrial flutter. We did not pose restrictions on language or publication status.
Outcomes
The primary outcomes were initial and cumulative cardioversion success, defined as sinus rhythm following administration of the first and last shock, respectively. For ‘cross-over’ protocols, we only considered shocks delivered with the first allocated intervention. We included adverse events as secondary outcomes. We used individual studies’ definitions for all outcomes.
Data collection and analysis
We selected studies using Covidence (Veritas Health Innovation, Melbourne, Australia). Two reviewers independently screened studies based on titles and abstracts. Two reviewers then independently screened full texts and recorded the main reason for exclusion. We resolved disagreements through discussion with the supervising author.
Data extraction and management
For each study, two reviewers independently collected data, resolving disagreements by discussion with the supervising author. We collected data on bibliographic information, AF duration, study protocol, anticoagulant, and anti-arrhythmic drug use, description of the intervention and comparator, electrical cardioversion success, and adverse events. We contacted authors for further information as needed.
Data synthesis and subgroup analyses
We used Review Manager 5.4 (Cochrane Collaboration) to perform meta-analysis using the Mantel–Haenszel method. Results are presented as risk ratios (RRs) with 95% confidence intervals (CI) using random-effects models. A two-sided P-value <0.05 was considered statistically significant. We assessed heterogeneity with the I2 statistic and considered an I2 value of > 50% to represent substantial heterogeneity.17 We conducted pre-specified subgroup analyses based on waveform phases, energy dose, and electrode positioning.
Assessment of the quality of evidence
We assessed risk of bias in individual studies using the Cochrane Risk of Bias 1.0 tool for randomized trials and the CLARITY tool for observational studies.18–20 Reviewers evaluated randomized trials as having low, high, or unclear risk of bias across the domains of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias (e.g. premature study termination). We judged detection bias to be low in all studies due to the objective nature of the outcome and the short time from intervention to occurrence. We judged the risk of performance bias to be low if study protocols clearly outlined co-interventions; otherwise, we judged it to be high. We dichotomized the overall risk of bias as either low (all domains rated at a low risk of bias) or high (at least one domain rated at a high risk of bias). Reviewers assessed observational studies as having low, probably low, probably high, or high risk of bias.
We appraised the overall quality of the evidence for each comparison using the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) framework.21 Within the GRADE framework, randomized trials begin with a high-quality rating and observational studies begin with a low-quality rating. The quality of the evidence can be rated up or down based on five factors: risk of bias, directness of the evidence, heterogeneity of data, precision of results, and publication bias.
Results
Search results and study selection
Our search strategy identified a total of 15 207 unique citations, of which 258 met criteria for full-text screening. From this, 45 randomized trials (7110 participants) and 16 observational studies (4718 participants) met criteria for inclusion in the quantitative synthesis (see Supplementary material online, Appendix S3). Interventions studied in randomized trials included: shock waveforms (18 studies), energy dose (4 studies), pad positioning (14 studies), manual pressure (2 studies), biphasic waveform properties (5 studies), and electrode polarity (2 studies). The characteristics of the included randomized trials are summarized in Table 1 and detailed further in Supplementary material online, Appendix S4. The interventions compared in the 16 observational studies included: biphasic vs. monophasic shock waveform (six studies), energy dose (two studies), pad positioning (four studies), manual pressure (two studies), and biphasic waveform properties (two studies). Supplementary material online, Appendix S5 summarizes the characteristics of the included observational studies. Supplementary material online, Appendix S6 summarizes the characteristics of ongoing and important excluded studies.
Characteristics of included studies
| Author | Study arms | n | Electrode placement or waveform | Shock protocol (Joules) | Success rate (%) by attempt | Risk of bias | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| SHOCK WAVEFORM | ||||||||||
| Ambler 200622 | Monophasic | 68 | AA | 100, 200, 300, 360, 360 | 19 | 47 | 66 | 79 | 87 | High |
| Biphasic | 60 | AA | 70, 100, 150, 200, 300 | 33 | 70 | 84 | 92 | 93 | ||
| Kawabata 200723 | MDS | 77 | AA | 100, 200, 300, up to 360 | 54.6 | 81.8 | 90.9 | 92.2 | – | Low |
| BTE | 77 | AA | 50, 100, 150, up to 175 | 57.1 | 80.5 | 87.0 | 89.6 | – | ||
| Khaykin 200324 | MDS | 28 | AP | 360 | – | – | 21 | – | – | Low |
| BTE | 28 | AP | 150, 200, 360 | 22 | 43 | 69 | – | – | ||
| Kirchhof 200525 | MDS | 97 | AP | 50, 100, 200, 300, 360 | 8.3 | 16 | 48 | 68 | 80 | High |
| BTE | 104 | AP | 50, 100, 200, 300, 360 | 25 | 55 | 82 | 89 | 95 | ||
| Kmec 200626 | MDS | 100 | AL | 200, 300, 360, 360 | 27 | 60 | 80 | 83 | – | Low |
| BTE | 100 | AL | 100, 120, 270, 270 | 50 | 86 | 93 | 93 | – | ||
| Kosior 200527 | MDS | 22 | AL | 2 J/kg BW, then up to 2 shocks of 360 J | N/A | N/A | 88 | – | – | Low |
| BR | 26 | AL | 2 J/kg BW, then up to 2 shocks of 360 J | N/A | N/A | 100 | – | – | ||
| Koster 200428 | MDS | 37 | AL | 70, 100, 200, 360 | 5.4 | 19 | 38 | 86 | – | Low |
| BTE | 35 | AL | 70, 100, 200, 360 | 60 | 80 | 97 | 97 | – | ||
| Krasteva 200129 | MDS | 80 | N/A | 160 | 90 | – | – | – | – | Low |
| BTE | 31 | N/A | 80, 100, 120, 160, 180 | N/A | N/A | N/A | N/A | 87 | ||
| Manegold 200730 | MDS | 21 | AP | 200, 300, 360, 360 | 71% | N/A | N/A | 95 | – | Low |
| BR | 23 | AP | 100, 150, 200, 200 | 74% | N/A | N/A | 96 | – | ||
| Marinsek 200331 | MDS | 40 | AL | 100, 200, 300, 360 | N/A | N/A | N/A | 90 | – | High |
| BTE | 43 | AL | 70, 100, 150, 200 | N/A | N/A | N/A | 88.3 | – | ||
| Mittal 200032 | MDS | 77 | AP | 100, 200, 300, 360 | 21 | 44 | 68 | 79 | – | High |
| BR | 88 | AP | 70, 120, 150, 170 | 68 | 85 | 91 | 94 | – | ||
| Neumann 200433 | MDS | 57 | AP | 100, 200, 360 | 15.8 | 42.1 | 73.7 | – | – | Low |
| BTE | 61 | AP | 100, 200, 360 | 57.4 | 95.1 | 100 | – | – | ||
| Page 200234 | MDS | 107 | AP | 100, 150, 200, 360 | 22.4 | 43.9 | 53.3 | 85.1 | – | Low |
| BTE | 96 | AP | 100, 150, 200, 360 | 60.4 | 77.1 | 89.6 | 90.6 | – | ||
| Ricard 200135 | MDS | 27 | AL | 150, 360 | 59.3 | 88.9 | – | – | – | Low |
| BTE | 30 | AL | 150, 360 | 86.7 | 93.3 | – | – | – | ||
| Santomauro 200436 | MDS | 18 | AP | 100, 200, 300, 360, 360 | 5 | 27 | 50 | 72 | 78 | Low |
| BTE | 24 | AP | 70, 100, 150, 200, 200 | 15 | 55 | 80 | 95 | 100 | ||
| Santomauro 200436 | MDS | 18 | AP | 100, 200, 300, 360, 360 | 5 | 27 | 50 | 72 | 78 | Low |
| BR | 22 | AP | 75, 100, 150, 200, 200 | 9 | 45 | 72 | 90 | 95 | ||
| Siaplaouras 200437 | MDS | 108 | AP | 200, 300, 360, 360 | 67.7 | N/A | N/A | 96.8 | – | Low |
| RBW | 108 | AP | 120, 150, 200, 200 | 76.4 | N/A | N/A | 94.3 | – | ||
| Stanaitiene 200838 | MDS | 112 | AA, AP | 100, 200, 300, 360 | 37.5 | 63.4 | 77.7 | 79.5 | – | High |
| BTE | 112 | AA, AP | 100, 150, 200, 300, 360 | 67 | 88.4 | 94.6 | 97.3 | – | ||
| Vaisman 200539 | Monophasic | 22 | N/A | 200, 300, 360 | 95.5 | N/A | 95.5 | – | – | Low |
| Biphasic | 21 | N/A | 120, 150, 200 | 57.1 | N/A | 85.5 | – | – | ||
| ENERGY DOSE | ||||||||||
| Boodhoo 200740 | Escalating | 125 | AA-AA-AP MDS | 200 AA, 360AA, 360AP | 41.6 | 72.0 | 83.2 | – | – | Low |
| High energy | 136 | AA-AP-PA MDS | 360AA, 360AP, 360PA | 68.4 | 86.0 | 91.9 | – | – | ||
| Glover 200841 | Escalating | 193 | AA | 100, 150, 200, 200 | 47.7 | 76.7 | 87.6 | 90.2 | – | Low |
| BTE | ||||||||||
| High energy | 187 | AA | 200, 200, 200 | 70.6 | 82.9 | 88.2 | – | – | ||
| BTE | ||||||||||
| aGotcheva 201542 | Escalating | 112 | AL | 120, 200, 200, 360 | 54.5 | N/A | N/A | 95.5 | Low | |
| Biphasic | ||||||||||
| High energy | 169 | AL | 200, 200, 200, 360 | 72.9 | N/A | N/A | 88.8 | |||
| Biphasic | ||||||||||
| Schmidt 202043 | Escalating | 147 | AP | 120, 150, 200 | 34.0 | 53.1 | 66 | – | – | Low |
| BTE | ||||||||||
| High energy | 129 | AP | 360, 360, 360 | 75.2 | 85.3 | 88.4 | – | – | ||
| BTE | ||||||||||
| PAD PLACEMENT | ||||||||||
| Alp 200044 | AL | 30 | MDS | 360 | 60 | – | – | – | – | High |
| AP | 29 | MDS | 360 | 34.5 | – | – | – | – | ||
| Botto 199945 | AA | 151 | MDS | 3 J/kg BW then 4 J/kg (max. 360 J) | 58 | 76 | – | – | – | High |
| AP | 150 | MDS | 3 J/kg BW then 4 J/kg (max. 360 J) | 67 | 87 | – | – | – | ||
| Brazdzionyte 200646 | AL | 55 | BTE | 100, 150, 200, 300 | 72.7 | 94.5 | 96.3 | 98.2 | – | Low |
| AP | 48 | BTE | 100, 150, 200, 300 | 60.4 | 85.4 | 95.8 | 97.9 | – | ||
| Chen 200347 | AA | 31 | MDS | 100, 150, 200, 300, 360 | 19.4 | 45.2 | 74.2 | 77.4 | 83.9 | Low |
| AP | 39 | MDS | 100, 150, 200, 300, 360 | 23 | 41.0 | 66.7 | 79.5 | 84.6 | ||
| Kirchhof 200248 | AA | 56 | MDS | Preselected shock energies, starting at 50 J | 5.4 | 19.7 | 50.1 | 68 | 78.7 | High |
| AP | 52 | MDS | Preselected shock energies, starting at 50 J | 9.6 | 28.8 | 59.6 | 76.9 | 96.1 | ||
| Mathew 199949 | AA | 45 | N/A | 100, 200, 300, 360 | N/A | N/A | N/A | 84 | – | Low |
| AP | 45 | N/A | 100, 200, 300, 360 | N/A | N/A | N/A | 78 | – | ||
| Munoz-Martinez 201050 | AA | 46 | BTE | 150, 200, 200 | 70 | N/A | 96 | – | – | Low |
| AP | 45 | BTE | 150, 200, 200 | 40 | N/A | 94 | – | – | ||
| Schmidt 202151 | AL | 233 | BTE | 100, 150, 200, 360 | 54 | 75 | 86 | 93 | – | Low |
| AP | 234 | BTE | 100, 150, 200, 360 | 33 | 53 | 69 | 85 | – | ||
| Siaplaouras 200552 | AA | 63 | Biphasic | 120, 150, 200, 200 Watts | 74.6 | 87.3 | 93.6 | 95.2 | – | Low |
| AP | 60 | Biphasic | 120, 150, 200, 200 Watts | 78.3 | 89.9 | 94.9 | 94.9 | – | ||
| Steill 202053 | AL | 82 | Biphasic | ≥ 200 (3 shocks maximum) | 91.4 | N/A | 93.9 | – | – | Low |
| AP | 78 | Biphasic | ≥ 200 (3 shocks maximum) | 76.9 | N/A | 91.0 | – | – | ||
| Tuinenburg 199754 | AL | 35 | MDS | 100, 200, 360 | N/A | N/A | 85.7 | – | – | Low |
| AP | 35 | MDS | 100, 200, 360 | N/A | N/A | 82.9 | ||||
| Vogiatzis 200955 | AA | 32 | MDS | 200, 300, 360 | 43.8 | 62.5 | 96.9 | – | – | Low |
| AP | 30 | MDS | 200, 300, 360 | 50.0 | 93.3 | 100.0 | – | – | ||
| Voskoboinik 201956 | AL | 64 | Biphasic | 100, 200 | N/A | 76.5 | – | – | – | Low |
| AP | 61 | Biphasic | 100, 200 | N/A | 82 | – | – | – | ||
| Walsh 200557 | AA | 150 | BTE | 70, 100, 150, 200 | 36 | 66.0 | 82 | 95.3 | – | Low |
| AP | 144 | BTE | 70, 100, 150, 200 | 31 | 51.4 | 75.7 | 88.2 | – | ||
| MANUAL PRESSURE OR NO PRESSURE | ||||||||||
| Squara 202158 | Active compression | 50 | AP | 50, 100, 150, 200 | 10 | 46 | 72 | 84 | – | Low |
| Control | 50 | AP | 50, 100, 150, 200 | 34 | 66 | 86 | 96 | – | ||
| bVoskoboinik, 201956 | Hand-held paddles | 62 | AA or AP | 100, 200 | 50 | 90 | – | – | – | Low |
| adhesive patch | 63 | AA or AP | 100, 200 | 27 | 68 | – | – | – | ||
| BIPHASIC WAVEFORM PROPERTIES | ||||||||||
| Alatawi 200559 | BTE | 70 | AP | 50, 70, 100, 125, 150, 200, 300, 360 | 30 | N/A | N/A | N/A | N/A | High |
| BR | 71 | AP | 50, 75, 100, 120, 150, 200 | 21 | N/A | N/A | N/A | N/A | ||
| Deakin 201260 | BTE | 99 | N/A | 50, 100, 150, 200, 200 | 15.2 | 47.5 | 68.7 | 87.9 | 90.9 | High |
| BR | 101 | N/A | 50, 100, 150, 200, 200 | 18.8 | 58.4 | 82.2 | 91.1 | 95.1 | ||
| Kim 200461 | BTE | 74 | AP | 50, 100, 150, 200, 360 | 54 | 84 | 92 | 97 | 97 | Low |
| BR | 71 | AP | 50, 100, 150, 200 | 61 | 79 | 93 | 97 | – | ||
| Neal 200362 | BTE | 48 | AP | 50, 100, 200, 200 | 52.1 | 83.3 | 95.8 | 97.9 | – | Low |
| BR | 53 | AP | 50, 100, 200, 200 | 64.2 | 94.3 | 100.00 | 100.00 | – | ||
| Schmidt 201763 | BTE | 65 | AP | 100, 150, 200, 250 | N/A | N/A | N/A | 86 | – | High |
| PB | 69 | AP | 90, 120, 150, 200 | N/A | N/A | N/A | 62 | – | ||
| ELECTRODE POLARITY | ||||||||||
| Oral 199964 | Anterior cathodal configuration | 100 | MDS, AA | 50, 100, 200, 300, 360 | N/A | N/A | 85 | N/A | 94 | Low |
| Anterior anodal configuration | 100 | MDS, AA | 50, 100, 200, 300, 360 | N/A | N/A | 72 | N/A | 96 | ||
| Rashba 200265 | Anterior cathodal configuration | 55 | AP | 50, 100, 200, 300, 360 | N/A | N/A | N/A | N/A | 83.4 | Low |
| Anterior anodal configuration | 55 | AP | 50, 100, 200, 300, 360 | N/A | N/A | N/A | N/A | 78.1 | ||
| Author | Study arms | n | Electrode placement or waveform | Shock protocol (Joules) | Success rate (%) by attempt | Risk of bias | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| SHOCK WAVEFORM | ||||||||||
| Ambler 200622 | Monophasic | 68 | AA | 100, 200, 300, 360, 360 | 19 | 47 | 66 | 79 | 87 | High |
| Biphasic | 60 | AA | 70, 100, 150, 200, 300 | 33 | 70 | 84 | 92 | 93 | ||
| Kawabata 200723 | MDS | 77 | AA | 100, 200, 300, up to 360 | 54.6 | 81.8 | 90.9 | 92.2 | – | Low |
| BTE | 77 | AA | 50, 100, 150, up to 175 | 57.1 | 80.5 | 87.0 | 89.6 | – | ||
| Khaykin 200324 | MDS | 28 | AP | 360 | – | – | 21 | – | – | Low |
| BTE | 28 | AP | 150, 200, 360 | 22 | 43 | 69 | – | – | ||
| Kirchhof 200525 | MDS | 97 | AP | 50, 100, 200, 300, 360 | 8.3 | 16 | 48 | 68 | 80 | High |
| BTE | 104 | AP | 50, 100, 200, 300, 360 | 25 | 55 | 82 | 89 | 95 | ||
| Kmec 200626 | MDS | 100 | AL | 200, 300, 360, 360 | 27 | 60 | 80 | 83 | – | Low |
| BTE | 100 | AL | 100, 120, 270, 270 | 50 | 86 | 93 | 93 | – | ||
| Kosior 200527 | MDS | 22 | AL | 2 J/kg BW, then up to 2 shocks of 360 J | N/A | N/A | 88 | – | – | Low |
| BR | 26 | AL | 2 J/kg BW, then up to 2 shocks of 360 J | N/A | N/A | 100 | – | – | ||
| Koster 200428 | MDS | 37 | AL | 70, 100, 200, 360 | 5.4 | 19 | 38 | 86 | – | Low |
| BTE | 35 | AL | 70, 100, 200, 360 | 60 | 80 | 97 | 97 | – | ||
| Krasteva 200129 | MDS | 80 | N/A | 160 | 90 | – | – | – | – | Low |
| BTE | 31 | N/A | 80, 100, 120, 160, 180 | N/A | N/A | N/A | N/A | 87 | ||
| Manegold 200730 | MDS | 21 | AP | 200, 300, 360, 360 | 71% | N/A | N/A | 95 | – | Low |
| BR | 23 | AP | 100, 150, 200, 200 | 74% | N/A | N/A | 96 | – | ||
| Marinsek 200331 | MDS | 40 | AL | 100, 200, 300, 360 | N/A | N/A | N/A | 90 | – | High |
| BTE | 43 | AL | 70, 100, 150, 200 | N/A | N/A | N/A | 88.3 | – | ||
| Mittal 200032 | MDS | 77 | AP | 100, 200, 300, 360 | 21 | 44 | 68 | 79 | – | High |
| BR | 88 | AP | 70, 120, 150, 170 | 68 | 85 | 91 | 94 | – | ||
| Neumann 200433 | MDS | 57 | AP | 100, 200, 360 | 15.8 | 42.1 | 73.7 | – | – | Low |
| BTE | 61 | AP | 100, 200, 360 | 57.4 | 95.1 | 100 | – | – | ||
| Page 200234 | MDS | 107 | AP | 100, 150, 200, 360 | 22.4 | 43.9 | 53.3 | 85.1 | – | Low |
| BTE | 96 | AP | 100, 150, 200, 360 | 60.4 | 77.1 | 89.6 | 90.6 | – | ||
| Ricard 200135 | MDS | 27 | AL | 150, 360 | 59.3 | 88.9 | – | – | – | Low |
| BTE | 30 | AL | 150, 360 | 86.7 | 93.3 | – | – | – | ||
| Santomauro 200436 | MDS | 18 | AP | 100, 200, 300, 360, 360 | 5 | 27 | 50 | 72 | 78 | Low |
| BTE | 24 | AP | 70, 100, 150, 200, 200 | 15 | 55 | 80 | 95 | 100 | ||
| Santomauro 200436 | MDS | 18 | AP | 100, 200, 300, 360, 360 | 5 | 27 | 50 | 72 | 78 | Low |
| BR | 22 | AP | 75, 100, 150, 200, 200 | 9 | 45 | 72 | 90 | 95 | ||
| Siaplaouras 200437 | MDS | 108 | AP | 200, 300, 360, 360 | 67.7 | N/A | N/A | 96.8 | – | Low |
| RBW | 108 | AP | 120, 150, 200, 200 | 76.4 | N/A | N/A | 94.3 | – | ||
| Stanaitiene 200838 | MDS | 112 | AA, AP | 100, 200, 300, 360 | 37.5 | 63.4 | 77.7 | 79.5 | – | High |
| BTE | 112 | AA, AP | 100, 150, 200, 300, 360 | 67 | 88.4 | 94.6 | 97.3 | – | ||
| Vaisman 200539 | Monophasic | 22 | N/A | 200, 300, 360 | 95.5 | N/A | 95.5 | – | – | Low |
| Biphasic | 21 | N/A | 120, 150, 200 | 57.1 | N/A | 85.5 | – | – | ||
| ENERGY DOSE | ||||||||||
| Boodhoo 200740 | Escalating | 125 | AA-AA-AP MDS | 200 AA, 360AA, 360AP | 41.6 | 72.0 | 83.2 | – | – | Low |
| High energy | 136 | AA-AP-PA MDS | 360AA, 360AP, 360PA | 68.4 | 86.0 | 91.9 | – | – | ||
| Glover 200841 | Escalating | 193 | AA | 100, 150, 200, 200 | 47.7 | 76.7 | 87.6 | 90.2 | – | Low |
| BTE | ||||||||||
| High energy | 187 | AA | 200, 200, 200 | 70.6 | 82.9 | 88.2 | – | – | ||
| BTE | ||||||||||
| aGotcheva 201542 | Escalating | 112 | AL | 120, 200, 200, 360 | 54.5 | N/A | N/A | 95.5 | Low | |
| Biphasic | ||||||||||
| High energy | 169 | AL | 200, 200, 200, 360 | 72.9 | N/A | N/A | 88.8 | |||
| Biphasic | ||||||||||
| Schmidt 202043 | Escalating | 147 | AP | 120, 150, 200 | 34.0 | 53.1 | 66 | – | – | Low |
| BTE | ||||||||||
| High energy | 129 | AP | 360, 360, 360 | 75.2 | 85.3 | 88.4 | – | – | ||
| BTE | ||||||||||
| PAD PLACEMENT | ||||||||||
| Alp 200044 | AL | 30 | MDS | 360 | 60 | – | – | – | – | High |
| AP | 29 | MDS | 360 | 34.5 | – | – | – | – | ||
| Botto 199945 | AA | 151 | MDS | 3 J/kg BW then 4 J/kg (max. 360 J) | 58 | 76 | – | – | – | High |
| AP | 150 | MDS | 3 J/kg BW then 4 J/kg (max. 360 J) | 67 | 87 | – | – | – | ||
| Brazdzionyte 200646 | AL | 55 | BTE | 100, 150, 200, 300 | 72.7 | 94.5 | 96.3 | 98.2 | – | Low |
| AP | 48 | BTE | 100, 150, 200, 300 | 60.4 | 85.4 | 95.8 | 97.9 | – | ||
| Chen 200347 | AA | 31 | MDS | 100, 150, 200, 300, 360 | 19.4 | 45.2 | 74.2 | 77.4 | 83.9 | Low |
| AP | 39 | MDS | 100, 150, 200, 300, 360 | 23 | 41.0 | 66.7 | 79.5 | 84.6 | ||
| Kirchhof 200248 | AA | 56 | MDS | Preselected shock energies, starting at 50 J | 5.4 | 19.7 | 50.1 | 68 | 78.7 | High |
| AP | 52 | MDS | Preselected shock energies, starting at 50 J | 9.6 | 28.8 | 59.6 | 76.9 | 96.1 | ||
| Mathew 199949 | AA | 45 | N/A | 100, 200, 300, 360 | N/A | N/A | N/A | 84 | – | Low |
| AP | 45 | N/A | 100, 200, 300, 360 | N/A | N/A | N/A | 78 | – | ||
| Munoz-Martinez 201050 | AA | 46 | BTE | 150, 200, 200 | 70 | N/A | 96 | – | – | Low |
| AP | 45 | BTE | 150, 200, 200 | 40 | N/A | 94 | – | – | ||
| Schmidt 202151 | AL | 233 | BTE | 100, 150, 200, 360 | 54 | 75 | 86 | 93 | – | Low |
| AP | 234 | BTE | 100, 150, 200, 360 | 33 | 53 | 69 | 85 | – | ||
| Siaplaouras 200552 | AA | 63 | Biphasic | 120, 150, 200, 200 Watts | 74.6 | 87.3 | 93.6 | 95.2 | – | Low |
| AP | 60 | Biphasic | 120, 150, 200, 200 Watts | 78.3 | 89.9 | 94.9 | 94.9 | – | ||
| Steill 202053 | AL | 82 | Biphasic | ≥ 200 (3 shocks maximum) | 91.4 | N/A | 93.9 | – | – | Low |
| AP | 78 | Biphasic | ≥ 200 (3 shocks maximum) | 76.9 | N/A | 91.0 | – | – | ||
| Tuinenburg 199754 | AL | 35 | MDS | 100, 200, 360 | N/A | N/A | 85.7 | – | – | Low |
| AP | 35 | MDS | 100, 200, 360 | N/A | N/A | 82.9 | ||||
| Vogiatzis 200955 | AA | 32 | MDS | 200, 300, 360 | 43.8 | 62.5 | 96.9 | – | – | Low |
| AP | 30 | MDS | 200, 300, 360 | 50.0 | 93.3 | 100.0 | – | – | ||
| Voskoboinik 201956 | AL | 64 | Biphasic | 100, 200 | N/A | 76.5 | – | – | – | Low |
| AP | 61 | Biphasic | 100, 200 | N/A | 82 | – | – | – | ||
| Walsh 200557 | AA | 150 | BTE | 70, 100, 150, 200 | 36 | 66.0 | 82 | 95.3 | – | Low |
| AP | 144 | BTE | 70, 100, 150, 200 | 31 | 51.4 | 75.7 | 88.2 | – | ||
| MANUAL PRESSURE OR NO PRESSURE | ||||||||||
| Squara 202158 | Active compression | 50 | AP | 50, 100, 150, 200 | 10 | 46 | 72 | 84 | – | Low |
| Control | 50 | AP | 50, 100, 150, 200 | 34 | 66 | 86 | 96 | – | ||
| bVoskoboinik, 201956 | Hand-held paddles | 62 | AA or AP | 100, 200 | 50 | 90 | – | – | – | Low |
| adhesive patch | 63 | AA or AP | 100, 200 | 27 | 68 | – | – | – | ||
| BIPHASIC WAVEFORM PROPERTIES | ||||||||||
| Alatawi 200559 | BTE | 70 | AP | 50, 70, 100, 125, 150, 200, 300, 360 | 30 | N/A | N/A | N/A | N/A | High |
| BR | 71 | AP | 50, 75, 100, 120, 150, 200 | 21 | N/A | N/A | N/A | N/A | ||
| Deakin 201260 | BTE | 99 | N/A | 50, 100, 150, 200, 200 | 15.2 | 47.5 | 68.7 | 87.9 | 90.9 | High |
| BR | 101 | N/A | 50, 100, 150, 200, 200 | 18.8 | 58.4 | 82.2 | 91.1 | 95.1 | ||
| Kim 200461 | BTE | 74 | AP | 50, 100, 150, 200, 360 | 54 | 84 | 92 | 97 | 97 | Low |
| BR | 71 | AP | 50, 100, 150, 200 | 61 | 79 | 93 | 97 | – | ||
| Neal 200362 | BTE | 48 | AP | 50, 100, 200, 200 | 52.1 | 83.3 | 95.8 | 97.9 | – | Low |
| BR | 53 | AP | 50, 100, 200, 200 | 64.2 | 94.3 | 100.00 | 100.00 | – | ||
| Schmidt 201763 | BTE | 65 | AP | 100, 150, 200, 250 | N/A | N/A | N/A | 86 | – | High |
| PB | 69 | AP | 90, 120, 150, 200 | N/A | N/A | N/A | 62 | – | ||
| ELECTRODE POLARITY | ||||||||||
| Oral 199964 | Anterior cathodal configuration | 100 | MDS, AA | 50, 100, 200, 300, 360 | N/A | N/A | 85 | N/A | 94 | Low |
| Anterior anodal configuration | 100 | MDS, AA | 50, 100, 200, 300, 360 | N/A | N/A | 72 | N/A | 96 | ||
| Rashba 200265 | Anterior cathodal configuration | 55 | AP | 50, 100, 200, 300, 360 | N/A | N/A | N/A | N/A | 83.4 | Low |
| Anterior anodal configuration | 55 | AP | 50, 100, 200, 300, 360 | N/A | N/A | N/A | N/A | 78.1 | ||
Separate group involving escalating protocol based on body surface area not included.
Special inclusion criterion of body mass index of 30 or greater.
Abbreviations: AA, antero-apical pad positioning; AL, antero-lateral pad positioning; AP, antero-posterior pad positioning; BR, biphasic rectilinear waveform; BTE, biphasic truncated exponential waveform; MDS, monophasic dampened sinusoidal waveform; N/A, not applicable (not reported); SR, sinus rhythm.
Characteristics of included studies
| Author | Study arms | n | Electrode placement or waveform | Shock protocol (Joules) | Success rate (%) by attempt | Risk of bias | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| SHOCK WAVEFORM | ||||||||||
| Ambler 200622 | Monophasic | 68 | AA | 100, 200, 300, 360, 360 | 19 | 47 | 66 | 79 | 87 | High |
| Biphasic | 60 | AA | 70, 100, 150, 200, 300 | 33 | 70 | 84 | 92 | 93 | ||
| Kawabata 200723 | MDS | 77 | AA | 100, 200, 300, up to 360 | 54.6 | 81.8 | 90.9 | 92.2 | – | Low |
| BTE | 77 | AA | 50, 100, 150, up to 175 | 57.1 | 80.5 | 87.0 | 89.6 | – | ||
| Khaykin 200324 | MDS | 28 | AP | 360 | – | – | 21 | – | – | Low |
| BTE | 28 | AP | 150, 200, 360 | 22 | 43 | 69 | – | – | ||
| Kirchhof 200525 | MDS | 97 | AP | 50, 100, 200, 300, 360 | 8.3 | 16 | 48 | 68 | 80 | High |
| BTE | 104 | AP | 50, 100, 200, 300, 360 | 25 | 55 | 82 | 89 | 95 | ||
| Kmec 200626 | MDS | 100 | AL | 200, 300, 360, 360 | 27 | 60 | 80 | 83 | – | Low |
| BTE | 100 | AL | 100, 120, 270, 270 | 50 | 86 | 93 | 93 | – | ||
| Kosior 200527 | MDS | 22 | AL | 2 J/kg BW, then up to 2 shocks of 360 J | N/A | N/A | 88 | – | – | Low |
| BR | 26 | AL | 2 J/kg BW, then up to 2 shocks of 360 J | N/A | N/A | 100 | – | – | ||
| Koster 200428 | MDS | 37 | AL | 70, 100, 200, 360 | 5.4 | 19 | 38 | 86 | – | Low |
| BTE | 35 | AL | 70, 100, 200, 360 | 60 | 80 | 97 | 97 | – | ||
| Krasteva 200129 | MDS | 80 | N/A | 160 | 90 | – | – | – | – | Low |
| BTE | 31 | N/A | 80, 100, 120, 160, 180 | N/A | N/A | N/A | N/A | 87 | ||
| Manegold 200730 | MDS | 21 | AP | 200, 300, 360, 360 | 71% | N/A | N/A | 95 | – | Low |
| BR | 23 | AP | 100, 150, 200, 200 | 74% | N/A | N/A | 96 | – | ||
| Marinsek 200331 | MDS | 40 | AL | 100, 200, 300, 360 | N/A | N/A | N/A | 90 | – | High |
| BTE | 43 | AL | 70, 100, 150, 200 | N/A | N/A | N/A | 88.3 | – | ||
| Mittal 200032 | MDS | 77 | AP | 100, 200, 300, 360 | 21 | 44 | 68 | 79 | – | High |
| BR | 88 | AP | 70, 120, 150, 170 | 68 | 85 | 91 | 94 | – | ||
| Neumann 200433 | MDS | 57 | AP | 100, 200, 360 | 15.8 | 42.1 | 73.7 | – | – | Low |
| BTE | 61 | AP | 100, 200, 360 | 57.4 | 95.1 | 100 | – | – | ||
| Page 200234 | MDS | 107 | AP | 100, 150, 200, 360 | 22.4 | 43.9 | 53.3 | 85.1 | – | Low |
| BTE | 96 | AP | 100, 150, 200, 360 | 60.4 | 77.1 | 89.6 | 90.6 | – | ||
| Ricard 200135 | MDS | 27 | AL | 150, 360 | 59.3 | 88.9 | – | – | – | Low |
| BTE | 30 | AL | 150, 360 | 86.7 | 93.3 | – | – | – | ||
| Santomauro 200436 | MDS | 18 | AP | 100, 200, 300, 360, 360 | 5 | 27 | 50 | 72 | 78 | Low |
| BTE | 24 | AP | 70, 100, 150, 200, 200 | 15 | 55 | 80 | 95 | 100 | ||
| Santomauro 200436 | MDS | 18 | AP | 100, 200, 300, 360, 360 | 5 | 27 | 50 | 72 | 78 | Low |
| BR | 22 | AP | 75, 100, 150, 200, 200 | 9 | 45 | 72 | 90 | 95 | ||
| Siaplaouras 200437 | MDS | 108 | AP | 200, 300, 360, 360 | 67.7 | N/A | N/A | 96.8 | – | Low |
| RBW | 108 | AP | 120, 150, 200, 200 | 76.4 | N/A | N/A | 94.3 | – | ||
| Stanaitiene 200838 | MDS | 112 | AA, AP | 100, 200, 300, 360 | 37.5 | 63.4 | 77.7 | 79.5 | – | High |
| BTE | 112 | AA, AP | 100, 150, 200, 300, 360 | 67 | 88.4 | 94.6 | 97.3 | – | ||
| Vaisman 200539 | Monophasic | 22 | N/A | 200, 300, 360 | 95.5 | N/A | 95.5 | – | – | Low |
| Biphasic | 21 | N/A | 120, 150, 200 | 57.1 | N/A | 85.5 | – | – | ||
| ENERGY DOSE | ||||||||||
| Boodhoo 200740 | Escalating | 125 | AA-AA-AP MDS | 200 AA, 360AA, 360AP | 41.6 | 72.0 | 83.2 | – | – | Low |
| High energy | 136 | AA-AP-PA MDS | 360AA, 360AP, 360PA | 68.4 | 86.0 | 91.9 | – | – | ||
| Glover 200841 | Escalating | 193 | AA | 100, 150, 200, 200 | 47.7 | 76.7 | 87.6 | 90.2 | – | Low |
| BTE | ||||||||||
| High energy | 187 | AA | 200, 200, 200 | 70.6 | 82.9 | 88.2 | – | – | ||
| BTE | ||||||||||
| aGotcheva 201542 | Escalating | 112 | AL | 120, 200, 200, 360 | 54.5 | N/A | N/A | 95.5 | Low | |
| Biphasic | ||||||||||
| High energy | 169 | AL | 200, 200, 200, 360 | 72.9 | N/A | N/A | 88.8 | |||
| Biphasic | ||||||||||
| Schmidt 202043 | Escalating | 147 | AP | 120, 150, 200 | 34.0 | 53.1 | 66 | – | – | Low |
| BTE | ||||||||||
| High energy | 129 | AP | 360, 360, 360 | 75.2 | 85.3 | 88.4 | – | – | ||
| BTE | ||||||||||
| PAD PLACEMENT | ||||||||||
| Alp 200044 | AL | 30 | MDS | 360 | 60 | – | – | – | – | High |
| AP | 29 | MDS | 360 | 34.5 | – | – | – | – | ||
| Botto 199945 | AA | 151 | MDS | 3 J/kg BW then 4 J/kg (max. 360 J) | 58 | 76 | – | – | – | High |
| AP | 150 | MDS | 3 J/kg BW then 4 J/kg (max. 360 J) | 67 | 87 | – | – | – | ||
| Brazdzionyte 200646 | AL | 55 | BTE | 100, 150, 200, 300 | 72.7 | 94.5 | 96.3 | 98.2 | – | Low |
| AP | 48 | BTE | 100, 150, 200, 300 | 60.4 | 85.4 | 95.8 | 97.9 | – | ||
| Chen 200347 | AA | 31 | MDS | 100, 150, 200, 300, 360 | 19.4 | 45.2 | 74.2 | 77.4 | 83.9 | Low |
| AP | 39 | MDS | 100, 150, 200, 300, 360 | 23 | 41.0 | 66.7 | 79.5 | 84.6 | ||
| Kirchhof 200248 | AA | 56 | MDS | Preselected shock energies, starting at 50 J | 5.4 | 19.7 | 50.1 | 68 | 78.7 | High |
| AP | 52 | MDS | Preselected shock energies, starting at 50 J | 9.6 | 28.8 | 59.6 | 76.9 | 96.1 | ||
| Mathew 199949 | AA | 45 | N/A | 100, 200, 300, 360 | N/A | N/A | N/A | 84 | – | Low |
| AP | 45 | N/A | 100, 200, 300, 360 | N/A | N/A | N/A | 78 | – | ||
| Munoz-Martinez 201050 | AA | 46 | BTE | 150, 200, 200 | 70 | N/A | 96 | – | – | Low |
| AP | 45 | BTE | 150, 200, 200 | 40 | N/A | 94 | – | – | ||
| Schmidt 202151 | AL | 233 | BTE | 100, 150, 200, 360 | 54 | 75 | 86 | 93 | – | Low |
| AP | 234 | BTE | 100, 150, 200, 360 | 33 | 53 | 69 | 85 | – | ||
| Siaplaouras 200552 | AA | 63 | Biphasic | 120, 150, 200, 200 Watts | 74.6 | 87.3 | 93.6 | 95.2 | – | Low |
| AP | 60 | Biphasic | 120, 150, 200, 200 Watts | 78.3 | 89.9 | 94.9 | 94.9 | – | ||
| Steill 202053 | AL | 82 | Biphasic | ≥ 200 (3 shocks maximum) | 91.4 | N/A | 93.9 | – | – | Low |
| AP | 78 | Biphasic | ≥ 200 (3 shocks maximum) | 76.9 | N/A | 91.0 | – | – | ||
| Tuinenburg 199754 | AL | 35 | MDS | 100, 200, 360 | N/A | N/A | 85.7 | – | – | Low |
| AP | 35 | MDS | 100, 200, 360 | N/A | N/A | 82.9 | ||||
| Vogiatzis 200955 | AA | 32 | MDS | 200, 300, 360 | 43.8 | 62.5 | 96.9 | – | – | Low |
| AP | 30 | MDS | 200, 300, 360 | 50.0 | 93.3 | 100.0 | – | – | ||
| Voskoboinik 201956 | AL | 64 | Biphasic | 100, 200 | N/A | 76.5 | – | – | – | Low |
| AP | 61 | Biphasic | 100, 200 | N/A | 82 | – | – | – | ||
| Walsh 200557 | AA | 150 | BTE | 70, 100, 150, 200 | 36 | 66.0 | 82 | 95.3 | – | Low |
| AP | 144 | BTE | 70, 100, 150, 200 | 31 | 51.4 | 75.7 | 88.2 | – | ||
| MANUAL PRESSURE OR NO PRESSURE | ||||||||||
| Squara 202158 | Active compression | 50 | AP | 50, 100, 150, 200 | 10 | 46 | 72 | 84 | – | Low |
| Control | 50 | AP | 50, 100, 150, 200 | 34 | 66 | 86 | 96 | – | ||
| bVoskoboinik, 201956 | Hand-held paddles | 62 | AA or AP | 100, 200 | 50 | 90 | – | – | – | Low |
| adhesive patch | 63 | AA or AP | 100, 200 | 27 | 68 | – | – | – | ||
| BIPHASIC WAVEFORM PROPERTIES | ||||||||||
| Alatawi 200559 | BTE | 70 | AP | 50, 70, 100, 125, 150, 200, 300, 360 | 30 | N/A | N/A | N/A | N/A | High |
| BR | 71 | AP | 50, 75, 100, 120, 150, 200 | 21 | N/A | N/A | N/A | N/A | ||
| Deakin 201260 | BTE | 99 | N/A | 50, 100, 150, 200, 200 | 15.2 | 47.5 | 68.7 | 87.9 | 90.9 | High |
| BR | 101 | N/A | 50, 100, 150, 200, 200 | 18.8 | 58.4 | 82.2 | 91.1 | 95.1 | ||
| Kim 200461 | BTE | 74 | AP | 50, 100, 150, 200, 360 | 54 | 84 | 92 | 97 | 97 | Low |
| BR | 71 | AP | 50, 100, 150, 200 | 61 | 79 | 93 | 97 | – | ||
| Neal 200362 | BTE | 48 | AP | 50, 100, 200, 200 | 52.1 | 83.3 | 95.8 | 97.9 | – | Low |
| BR | 53 | AP | 50, 100, 200, 200 | 64.2 | 94.3 | 100.00 | 100.00 | – | ||
| Schmidt 201763 | BTE | 65 | AP | 100, 150, 200, 250 | N/A | N/A | N/A | 86 | – | High |
| PB | 69 | AP | 90, 120, 150, 200 | N/A | N/A | N/A | 62 | – | ||
| ELECTRODE POLARITY | ||||||||||
| Oral 199964 | Anterior cathodal configuration | 100 | MDS, AA | 50, 100, 200, 300, 360 | N/A | N/A | 85 | N/A | 94 | Low |
| Anterior anodal configuration | 100 | MDS, AA | 50, 100, 200, 300, 360 | N/A | N/A | 72 | N/A | 96 | ||
| Rashba 200265 | Anterior cathodal configuration | 55 | AP | 50, 100, 200, 300, 360 | N/A | N/A | N/A | N/A | 83.4 | Low |
| Anterior anodal configuration | 55 | AP | 50, 100, 200, 300, 360 | N/A | N/A | N/A | N/A | 78.1 | ||
| Author | Study arms | n | Electrode placement or waveform | Shock protocol (Joules) | Success rate (%) by attempt | Risk of bias | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| SHOCK WAVEFORM | ||||||||||
| Ambler 200622 | Monophasic | 68 | AA | 100, 200, 300, 360, 360 | 19 | 47 | 66 | 79 | 87 | High |
| Biphasic | 60 | AA | 70, 100, 150, 200, 300 | 33 | 70 | 84 | 92 | 93 | ||
| Kawabata 200723 | MDS | 77 | AA | 100, 200, 300, up to 360 | 54.6 | 81.8 | 90.9 | 92.2 | – | Low |
| BTE | 77 | AA | 50, 100, 150, up to 175 | 57.1 | 80.5 | 87.0 | 89.6 | – | ||
| Khaykin 200324 | MDS | 28 | AP | 360 | – | – | 21 | – | – | Low |
| BTE | 28 | AP | 150, 200, 360 | 22 | 43 | 69 | – | – | ||
| Kirchhof 200525 | MDS | 97 | AP | 50, 100, 200, 300, 360 | 8.3 | 16 | 48 | 68 | 80 | High |
| BTE | 104 | AP | 50, 100, 200, 300, 360 | 25 | 55 | 82 | 89 | 95 | ||
| Kmec 200626 | MDS | 100 | AL | 200, 300, 360, 360 | 27 | 60 | 80 | 83 | – | Low |
| BTE | 100 | AL | 100, 120, 270, 270 | 50 | 86 | 93 | 93 | – | ||
| Kosior 200527 | MDS | 22 | AL | 2 J/kg BW, then up to 2 shocks of 360 J | N/A | N/A | 88 | – | – | Low |
| BR | 26 | AL | 2 J/kg BW, then up to 2 shocks of 360 J | N/A | N/A | 100 | – | – | ||
| Koster 200428 | MDS | 37 | AL | 70, 100, 200, 360 | 5.4 | 19 | 38 | 86 | – | Low |
| BTE | 35 | AL | 70, 100, 200, 360 | 60 | 80 | 97 | 97 | – | ||
| Krasteva 200129 | MDS | 80 | N/A | 160 | 90 | – | – | – | – | Low |
| BTE | 31 | N/A | 80, 100, 120, 160, 180 | N/A | N/A | N/A | N/A | 87 | ||
| Manegold 200730 | MDS | 21 | AP | 200, 300, 360, 360 | 71% | N/A | N/A | 95 | – | Low |
| BR | 23 | AP | 100, 150, 200, 200 | 74% | N/A | N/A | 96 | – | ||
| Marinsek 200331 | MDS | 40 | AL | 100, 200, 300, 360 | N/A | N/A | N/A | 90 | – | High |
| BTE | 43 | AL | 70, 100, 150, 200 | N/A | N/A | N/A | 88.3 | – | ||
| Mittal 200032 | MDS | 77 | AP | 100, 200, 300, 360 | 21 | 44 | 68 | 79 | – | High |
| BR | 88 | AP | 70, 120, 150, 170 | 68 | 85 | 91 | 94 | – | ||
| Neumann 200433 | MDS | 57 | AP | 100, 200, 360 | 15.8 | 42.1 | 73.7 | – | – | Low |
| BTE | 61 | AP | 100, 200, 360 | 57.4 | 95.1 | 100 | – | – | ||
| Page 200234 | MDS | 107 | AP | 100, 150, 200, 360 | 22.4 | 43.9 | 53.3 | 85.1 | – | Low |
| BTE | 96 | AP | 100, 150, 200, 360 | 60.4 | 77.1 | 89.6 | 90.6 | – | ||
| Ricard 200135 | MDS | 27 | AL | 150, 360 | 59.3 | 88.9 | – | – | – | Low |
| BTE | 30 | AL | 150, 360 | 86.7 | 93.3 | – | – | – | ||
| Santomauro 200436 | MDS | 18 | AP | 100, 200, 300, 360, 360 | 5 | 27 | 50 | 72 | 78 | Low |
| BTE | 24 | AP | 70, 100, 150, 200, 200 | 15 | 55 | 80 | 95 | 100 | ||
| Santomauro 200436 | MDS | 18 | AP | 100, 200, 300, 360, 360 | 5 | 27 | 50 | 72 | 78 | Low |
| BR | 22 | AP | 75, 100, 150, 200, 200 | 9 | 45 | 72 | 90 | 95 | ||
| Siaplaouras 200437 | MDS | 108 | AP | 200, 300, 360, 360 | 67.7 | N/A | N/A | 96.8 | – | Low |
| RBW | 108 | AP | 120, 150, 200, 200 | 76.4 | N/A | N/A | 94.3 | – | ||
| Stanaitiene 200838 | MDS | 112 | AA, AP | 100, 200, 300, 360 | 37.5 | 63.4 | 77.7 | 79.5 | – | High |
| BTE | 112 | AA, AP | 100, 150, 200, 300, 360 | 67 | 88.4 | 94.6 | 97.3 | – | ||
| Vaisman 200539 | Monophasic | 22 | N/A | 200, 300, 360 | 95.5 | N/A | 95.5 | – | – | Low |
| Biphasic | 21 | N/A | 120, 150, 200 | 57.1 | N/A | 85.5 | – | – | ||
| ENERGY DOSE | ||||||||||
| Boodhoo 200740 | Escalating | 125 | AA-AA-AP MDS | 200 AA, 360AA, 360AP | 41.6 | 72.0 | 83.2 | – | – | Low |
| High energy | 136 | AA-AP-PA MDS | 360AA, 360AP, 360PA | 68.4 | 86.0 | 91.9 | – | – | ||
| Glover 200841 | Escalating | 193 | AA | 100, 150, 200, 200 | 47.7 | 76.7 | 87.6 | 90.2 | – | Low |
| BTE | ||||||||||
| High energy | 187 | AA | 200, 200, 200 | 70.6 | 82.9 | 88.2 | – | – | ||
| BTE | ||||||||||
| aGotcheva 201542 | Escalating | 112 | AL | 120, 200, 200, 360 | 54.5 | N/A | N/A | 95.5 | Low | |
| Biphasic | ||||||||||
| High energy | 169 | AL | 200, 200, 200, 360 | 72.9 | N/A | N/A | 88.8 | |||
| Biphasic | ||||||||||
| Schmidt 202043 | Escalating | 147 | AP | 120, 150, 200 | 34.0 | 53.1 | 66 | – | – | Low |
| BTE | ||||||||||
| High energy | 129 | AP | 360, 360, 360 | 75.2 | 85.3 | 88.4 | – | – | ||
| BTE | ||||||||||
| PAD PLACEMENT | ||||||||||
| Alp 200044 | AL | 30 | MDS | 360 | 60 | – | – | – | – | High |
| AP | 29 | MDS | 360 | 34.5 | – | – | – | – | ||
| Botto 199945 | AA | 151 | MDS | 3 J/kg BW then 4 J/kg (max. 360 J) | 58 | 76 | – | – | – | High |
| AP | 150 | MDS | 3 J/kg BW then 4 J/kg (max. 360 J) | 67 | 87 | – | – | – | ||
| Brazdzionyte 200646 | AL | 55 | BTE | 100, 150, 200, 300 | 72.7 | 94.5 | 96.3 | 98.2 | – | Low |
| AP | 48 | BTE | 100, 150, 200, 300 | 60.4 | 85.4 | 95.8 | 97.9 | – | ||
| Chen 200347 | AA | 31 | MDS | 100, 150, 200, 300, 360 | 19.4 | 45.2 | 74.2 | 77.4 | 83.9 | Low |
| AP | 39 | MDS | 100, 150, 200, 300, 360 | 23 | 41.0 | 66.7 | 79.5 | 84.6 | ||
| Kirchhof 200248 | AA | 56 | MDS | Preselected shock energies, starting at 50 J | 5.4 | 19.7 | 50.1 | 68 | 78.7 | High |
| AP | 52 | MDS | Preselected shock energies, starting at 50 J | 9.6 | 28.8 | 59.6 | 76.9 | 96.1 | ||
| Mathew 199949 | AA | 45 | N/A | 100, 200, 300, 360 | N/A | N/A | N/A | 84 | – | Low |
| AP | 45 | N/A | 100, 200, 300, 360 | N/A | N/A | N/A | 78 | – | ||
| Munoz-Martinez 201050 | AA | 46 | BTE | 150, 200, 200 | 70 | N/A | 96 | – | – | Low |
| AP | 45 | BTE | 150, 200, 200 | 40 | N/A | 94 | – | – | ||
| Schmidt 202151 | AL | 233 | BTE | 100, 150, 200, 360 | 54 | 75 | 86 | 93 | – | Low |
| AP | 234 | BTE | 100, 150, 200, 360 | 33 | 53 | 69 | 85 | – | ||
| Siaplaouras 200552 | AA | 63 | Biphasic | 120, 150, 200, 200 Watts | 74.6 | 87.3 | 93.6 | 95.2 | – | Low |
| AP | 60 | Biphasic | 120, 150, 200, 200 Watts | 78.3 | 89.9 | 94.9 | 94.9 | – | ||
| Steill 202053 | AL | 82 | Biphasic | ≥ 200 (3 shocks maximum) | 91.4 | N/A | 93.9 | – | – | Low |
| AP | 78 | Biphasic | ≥ 200 (3 shocks maximum) | 76.9 | N/A | 91.0 | – | – | ||
| Tuinenburg 199754 | AL | 35 | MDS | 100, 200, 360 | N/A | N/A | 85.7 | – | – | Low |
| AP | 35 | MDS | 100, 200, 360 | N/A | N/A | 82.9 | ||||
| Vogiatzis 200955 | AA | 32 | MDS | 200, 300, 360 | 43.8 | 62.5 | 96.9 | – | – | Low |
| AP | 30 | MDS | 200, 300, 360 | 50.0 | 93.3 | 100.0 | – | – | ||
| Voskoboinik 201956 | AL | 64 | Biphasic | 100, 200 | N/A | 76.5 | – | – | – | Low |
| AP | 61 | Biphasic | 100, 200 | N/A | 82 | – | – | – | ||
| Walsh 200557 | AA | 150 | BTE | 70, 100, 150, 200 | 36 | 66.0 | 82 | 95.3 | – | Low |
| AP | 144 | BTE | 70, 100, 150, 200 | 31 | 51.4 | 75.7 | 88.2 | – | ||
| MANUAL PRESSURE OR NO PRESSURE | ||||||||||
| Squara 202158 | Active compression | 50 | AP | 50, 100, 150, 200 | 10 | 46 | 72 | 84 | – | Low |
| Control | 50 | AP | 50, 100, 150, 200 | 34 | 66 | 86 | 96 | – | ||
| bVoskoboinik, 201956 | Hand-held paddles | 62 | AA or AP | 100, 200 | 50 | 90 | – | – | – | Low |
| adhesive patch | 63 | AA or AP | 100, 200 | 27 | 68 | – | – | – | ||
| BIPHASIC WAVEFORM PROPERTIES | ||||||||||
| Alatawi 200559 | BTE | 70 | AP | 50, 70, 100, 125, 150, 200, 300, 360 | 30 | N/A | N/A | N/A | N/A | High |
| BR | 71 | AP | 50, 75, 100, 120, 150, 200 | 21 | N/A | N/A | N/A | N/A | ||
| Deakin 201260 | BTE | 99 | N/A | 50, 100, 150, 200, 200 | 15.2 | 47.5 | 68.7 | 87.9 | 90.9 | High |
| BR | 101 | N/A | 50, 100, 150, 200, 200 | 18.8 | 58.4 | 82.2 | 91.1 | 95.1 | ||
| Kim 200461 | BTE | 74 | AP | 50, 100, 150, 200, 360 | 54 | 84 | 92 | 97 | 97 | Low |
| BR | 71 | AP | 50, 100, 150, 200 | 61 | 79 | 93 | 97 | – | ||
| Neal 200362 | BTE | 48 | AP | 50, 100, 200, 200 | 52.1 | 83.3 | 95.8 | 97.9 | – | Low |
| BR | 53 | AP | 50, 100, 200, 200 | 64.2 | 94.3 | 100.00 | 100.00 | – | ||
| Schmidt 201763 | BTE | 65 | AP | 100, 150, 200, 250 | N/A | N/A | N/A | 86 | – | High |
| PB | 69 | AP | 90, 120, 150, 200 | N/A | N/A | N/A | 62 | – | ||
| ELECTRODE POLARITY | ||||||||||
| Oral 199964 | Anterior cathodal configuration | 100 | MDS, AA | 50, 100, 200, 300, 360 | N/A | N/A | 85 | N/A | 94 | Low |
| Anterior anodal configuration | 100 | MDS, AA | 50, 100, 200, 300, 360 | N/A | N/A | 72 | N/A | 96 | ||
| Rashba 200265 | Anterior cathodal configuration | 55 | AP | 50, 100, 200, 300, 360 | N/A | N/A | N/A | N/A | 83.4 | Low |
| Anterior anodal configuration | 55 | AP | 50, 100, 200, 300, 360 | N/A | N/A | N/A | N/A | 78.1 | ||
Separate group involving escalating protocol based on body surface area not included.
Special inclusion criterion of body mass index of 30 or greater.
Abbreviations: AA, antero-apical pad positioning; AL, antero-lateral pad positioning; AP, antero-posterior pad positioning; BR, biphasic rectilinear waveform; BTE, biphasic truncated exponential waveform; MDS, monophasic dampened sinusoidal waveform; N/A, not applicable (not reported); SR, sinus rhythm.
Assessment of risk of bias
We judged 28 trials as having an unclear risk of bias for randomization and 31 studies as having an unclear risk of bias for allocation concealment; no studies were rated high risk in these two domains. We judged all 46 trials to be at low risk of detection bias. We judged one trial to be at high risk for performance bias due to participants receiving unequal co-interventions.45 No studies had risk of attrition or reporting bias that we judged to have an important effect on outcomes. Three trials were terminated early for benefit44,48,63; this is known to potentially overestimate the true effect size.66Supplementary material online, Appendix S7 summarizes our judgments about each risk of bias item presented as percentages across all randomized trials. Supplementary material online, Appendix S8 summarizes our judgements about risk of bias across included randomized trials. Supplementary material online, Appendix S9 summarizes the risk of bias in observational studies.
Initial and cumulative cardioversion success
Table 2 summarizes the study’s overall findings.
Association of different interventions with initial and cumulative cardioversion success in patients with atrial fibrillation
| Intervention | Initial success | Cumulative success | ||||||
|---|---|---|---|---|---|---|---|---|
| Events/total (no. of patients) | Effect risk ratio (95% CI) | I2% | Quality of evidence | Events/total (no. of patients) | Effect risk ratio (95% CI) | I2% | Quality of evidence | |
| Shock waveform | ||||||||
| Monophasic | 316/974 | 1.71 (1.29–2.28) | 85 | Moderate | 936/1116 | 1.10 (1.04–1.16) | 70 | High |
| Biphasic | 538/989 | 1016/1089 | ||||||
| Energy dose | ||||||||
| High energy | 445/621 | 1.62 (1.33–1.98) | 72 | High | 553/621 | 1.07 (0.93–1.24) | 91 | Low |
| Escalating energy | 255/577 | 477/577 | ||||||
| Pad placement | ||||||||
| Antero-apical/lateral | 540/1091 | 1.16 (0.97–1.39) | 70 | Low | 984/1235 | 1.01 (0.96–1.06) | 62 | Moderate |
| Antero-posterior | 451/1075 | 939/1216 | ||||||
| Pressure | ||||||||
| No pressure | 22/112 | 2.19 (1.21–3.95) | 34 | High | 85/112 | 1.19 (1.06–1.34) | 9 | High |
| Manual pressure | 48/113 | 104/113 | ||||||
| Biphasic waveform properties | ||||||||
| Rectilinear/pulsed biphasic | 111/296 | 1.11 (0.91–1.34) | 0 | Moderate | 261/294 | 0.98 (0.89–1.08) | 84 | Moderate |
| Biphasic truncated exponential | 101/291 | 265/286 | ||||||
| Polarity | ||||||||
| Cathodal configuration | N/A | 140/155 | 0.99 (0.92–1.07) | 15 | High | |||
| Anodal configuration | 139/155 | |||||||
| Intervention | Initial success | Cumulative success | ||||||
|---|---|---|---|---|---|---|---|---|
| Events/total (no. of patients) | Effect risk ratio (95% CI) | I2% | Quality of evidence | Events/total (no. of patients) | Effect risk ratio (95% CI) | I2% | Quality of evidence | |
| Shock waveform | ||||||||
| Monophasic | 316/974 | 1.71 (1.29–2.28) | 85 | Moderate | 936/1116 | 1.10 (1.04–1.16) | 70 | High |
| Biphasic | 538/989 | 1016/1089 | ||||||
| Energy dose | ||||||||
| High energy | 445/621 | 1.62 (1.33–1.98) | 72 | High | 553/621 | 1.07 (0.93–1.24) | 91 | Low |
| Escalating energy | 255/577 | 477/577 | ||||||
| Pad placement | ||||||||
| Antero-apical/lateral | 540/1091 | 1.16 (0.97–1.39) | 70 | Low | 984/1235 | 1.01 (0.96–1.06) | 62 | Moderate |
| Antero-posterior | 451/1075 | 939/1216 | ||||||
| Pressure | ||||||||
| No pressure | 22/112 | 2.19 (1.21–3.95) | 34 | High | 85/112 | 1.19 (1.06–1.34) | 9 | High |
| Manual pressure | 48/113 | 104/113 | ||||||
| Biphasic waveform properties | ||||||||
| Rectilinear/pulsed biphasic | 111/296 | 1.11 (0.91–1.34) | 0 | Moderate | 261/294 | 0.98 (0.89–1.08) | 84 | Moderate |
| Biphasic truncated exponential | 101/291 | 265/286 | ||||||
| Polarity | ||||||||
| Cathodal configuration | N/A | 140/155 | 0.99 (0.92–1.07) | 15 | High | |||
| Anodal configuration | 139/155 | |||||||
Association of different interventions with initial and cumulative cardioversion success in patients with atrial fibrillation
| Intervention | Initial success | Cumulative success | ||||||
|---|---|---|---|---|---|---|---|---|
| Events/total (no. of patients) | Effect risk ratio (95% CI) | I2% | Quality of evidence | Events/total (no. of patients) | Effect risk ratio (95% CI) | I2% | Quality of evidence | |
| Shock waveform | ||||||||
| Monophasic | 316/974 | 1.71 (1.29–2.28) | 85 | Moderate | 936/1116 | 1.10 (1.04–1.16) | 70 | High |
| Biphasic | 538/989 | 1016/1089 | ||||||
| Energy dose | ||||||||
| High energy | 445/621 | 1.62 (1.33–1.98) | 72 | High | 553/621 | 1.07 (0.93–1.24) | 91 | Low |
| Escalating energy | 255/577 | 477/577 | ||||||
| Pad placement | ||||||||
| Antero-apical/lateral | 540/1091 | 1.16 (0.97–1.39) | 70 | Low | 984/1235 | 1.01 (0.96–1.06) | 62 | Moderate |
| Antero-posterior | 451/1075 | 939/1216 | ||||||
| Pressure | ||||||||
| No pressure | 22/112 | 2.19 (1.21–3.95) | 34 | High | 85/112 | 1.19 (1.06–1.34) | 9 | High |
| Manual pressure | 48/113 | 104/113 | ||||||
| Biphasic waveform properties | ||||||||
| Rectilinear/pulsed biphasic | 111/296 | 1.11 (0.91–1.34) | 0 | Moderate | 261/294 | 0.98 (0.89–1.08) | 84 | Moderate |
| Biphasic truncated exponential | 101/291 | 265/286 | ||||||
| Polarity | ||||||||
| Cathodal configuration | N/A | 140/155 | 0.99 (0.92–1.07) | 15 | High | |||
| Anodal configuration | 139/155 | |||||||
| Intervention | Initial success | Cumulative success | ||||||
|---|---|---|---|---|---|---|---|---|
| Events/total (no. of patients) | Effect risk ratio (95% CI) | I2% | Quality of evidence | Events/total (no. of patients) | Effect risk ratio (95% CI) | I2% | Quality of evidence | |
| Shock waveform | ||||||||
| Monophasic | 316/974 | 1.71 (1.29–2.28) | 85 | Moderate | 936/1116 | 1.10 (1.04–1.16) | 70 | High |
| Biphasic | 538/989 | 1016/1089 | ||||||
| Energy dose | ||||||||
| High energy | 445/621 | 1.62 (1.33–1.98) | 72 | High | 553/621 | 1.07 (0.93–1.24) | 91 | Low |
| Escalating energy | 255/577 | 477/577 | ||||||
| Pad placement | ||||||||
| Antero-apical/lateral | 540/1091 | 1.16 (0.97–1.39) | 70 | Low | 984/1235 | 1.01 (0.96–1.06) | 62 | Moderate |
| Antero-posterior | 451/1075 | 939/1216 | ||||||
| Pressure | ||||||||
| No pressure | 22/112 | 2.19 (1.21–3.95) | 34 | High | 85/112 | 1.19 (1.06–1.34) | 9 | High |
| Manual pressure | 48/113 | 104/113 | ||||||
| Biphasic waveform properties | ||||||||
| Rectilinear/pulsed biphasic | 111/296 | 1.11 (0.91–1.34) | 0 | Moderate | 261/294 | 0.98 (0.89–1.08) | 84 | Moderate |
| Biphasic truncated exponential | 101/291 | 265/286 | ||||||
| Polarity | ||||||||
| Cathodal configuration | N/A | 140/155 | 0.99 (0.92–1.07) | 15 | High | |||
| Anodal configuration | 139/155 | |||||||
Biphasic and monophasic waveforms
Sixteen randomized trials (1963 participants) compared initial cardioversion success between biphasic and monophasic waveforms.22–26,28,30,32–39 Biphasic waveforms resulted in an overall higher rate of cardioversion success (54 vs. 32%, RR 1.71, 95% CI 1.29–2.28, I2 = 85%, Figure 1A). Neither subgroup analyses comparing the two variations of the biphasic waveform (truncated exponential and rectilinear) nor subgroup analyses comparing pad positioning showed significant differences (all P > 0.05) (see Supplementary material online, Appendix S10). We judged the overall quality of evidence for initial cardioversion success to be high (see Supplementary material online, Appendix S13).
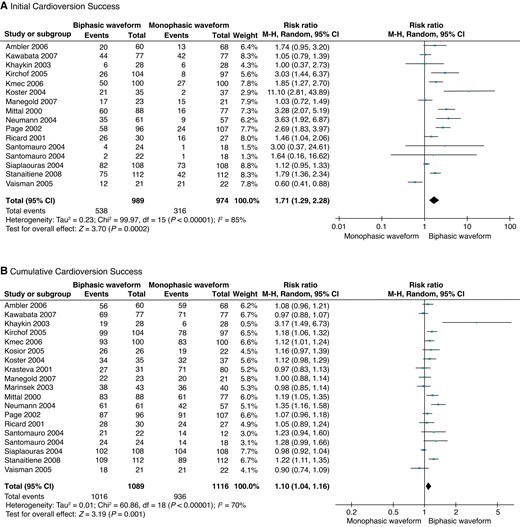
Forest plots for RCTs comparing biphasic and monophasic waveforms. (A) Initial cardioversion success. (B) Cumulative cardioversion success.
Nineteen randomized trials (2205 participants) compared cumulative cardioversion success between biphasic and monophasic waveforms.22–39 Biphasic waveforms resulted in an overall higher rate of cardioversion success (93 vs. 84%, RR 1.10, 95% CI 1.04–1.16, I2 = 70%, Figure 1B). All trials used low-dose escalating energy shock protocols. Subgroup analyses comparing the two variations of the biphasic waveform (truncated exponential and rectilinear) did not show any significant differences (P = 0.33) (see Supplementary material online, Appendix S10). Subgroup analyses comparing pad positioning also did not show significant differences (P = 0.32) (see Supplementary material online, Appendix S10). We judged the overall quality of evidence for cumulative cardioversion success to be high (see Supplementary material online, Appendix S13).
Energy dose
Four randomized trials (1198 participants) compared initial cardioversion success between high-energy shocks with a minimum of 200 J and shock protocols that started with low energy and escalated in the event of an unsuccessful shock.40–43 High-energy shocks resulted in a significant improvement in overall initial cardioversion success (72 vs. 44%, RR 1.62, 95% CI 1.33–1.98, I2 = 72%, Figure 2). Subgroup analyses based on electrode positioning showed a significant subgroup effect for initial cardioversion success in favour of a larger effect with antero-posterior pad positioning when compared with antero-apical or antero-lateral positioning (P = 0.003) (see Supplementary material online, Appendix S10). Neither biphasic when compared with monophasic waveforms (P = 0.93) nor a fixed energy protocol of 200 J compared with a fixed energy protocol of 360 J (P = 0.07) were effect modifiers for energy dose (see Supplementary material online, Appendix S10). We judged the overall quality of evidence for initial cardioversion success to be high (see Supplementary material online, Appendix S13).
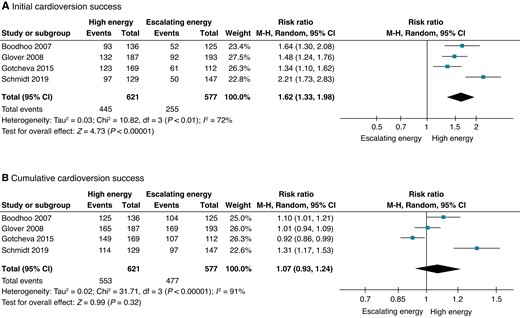
Forest plots of RCTs comparing fixed, high energy and low-dose, escalating energy. (A) Initial cardioversion success. (B) Cumulative cardioversion success.
The same four trials (1198 participants) compared cumulative cardioversion success between high-energy shocks and escalating energy protocols.40–43 High-energy shocks did not significantly improve overall cumulative cardioversion success (89 vs. 83%, RR 1.07, 95% CI 0.93–1.24, I2 = 91%, see Supplementary material online, Appendix S10). Subgroup analyses showed significant subgroup effects in favour of antero-posterior pad positioning (P = 0.04) and a fixed energy protocol using 360 J (P = 0.04) (see Supplementary material online, Appendix S10). There was no significant subgroup difference when comparing monophasic waveforms to biphasic waveforms (P = 0.75) (see Supplementary material online, Appendix S10). Quality of evidence for cumulative cardioversion success was moderate due to inconsistency (see Supplementary material online, Appendix S13).
Pad positioning
Eleven trials (2166 participants) compared initial cardioversion success between the antero-apical/lateral and antero-posterior pad positioning.44–48,50–53,55,57 The overall rate of initial cardioversion success was 49% for antero-apical/lateral and 42% for antero-posterior (RR 1.16, 95% CI 0.97–1.39, I2 = 70%, Figure 3A). A subgroup analysis comparing trials that used biphasic waveforms (six trials, RR 1.26, 95% CI 1.04–1.53, I2 = 71%) and those that used monophasic waveforms (five trials, RR 0.96, 95% CI 0.73–1.26, I2 = 29%) did not find a significant subgroup effect (P = 0.11) (see Supplementary material online, Appendix S10). A subgroup comparison of the one trial that applied fixed, high-energy shocks (RR 1.74, 95% CI 0.97–3.11) and 10 trials that applied escalating energy shocks (RR 1.14, 95% CI 0.95–1.36, I2 = 71%) did not find a significant subgroup effect for cumulative success (P = 0.17) (see Supplementary material online, Appendix S10). Quality of evidence for initial cardioversion success was low based on inconsistency and imprecision (see Supplementary material online, Appendix S13).

Forest plots for RCTs comparing antero-apical/lateral and antero-posterior pad placement. (A) Initial cardioversion success. (B) Cumulative cardioversion success.
Fourteen trials (2451 participants) compared cumulative cardioversion success between antero-apical/lateral and antero-posterior positioning.44–53,55–57 Overall cardioversion success was 80% for the antero-apical/lateral and 77% for the antero-posterior configuration (RR 1.01, 95% CI 0.96–1.06, I2 = 62%, Figure 3B). A subgroup analysis comparing trials that used biphasic waveforms (seven trials, RR 1.05, 95% CI 1.00–1.10, I2 = 52%) and trials that used monophasic waveforms (seven trials, RR 0.96, 95% CI 0.87–1.05, I2 = 55%) did not find a significant subgroup effect (P = 0.09). A subgroup comparison of the one trial that applied fixed, high-energy shocks (RR 1.74, 95% CI 0.97–3.11) and 10 trials that applied escalating energy shocks (RR 1.01, 95% CI 0.96–1.06, I2 = 61%) did not find a significant subgroup effect for cumulative success (P = 0.07) (see Supplementary material online, Appendix S10). In the third trials that reported the average number of shocks required to cardiovert, participants randomized to antero-posterior configuration and those randomized to the antero-apical/lateral configuration converted after a mean of 2 ± 1 shocks.46,52,55 Quality of evidence for cumulative cardioversion success was moderate due to inconsistency (see Supplementary material online, Appendix S13).
Manual pressure
Two trials (225 participants) compared initial cardioversion success with and without manual pressure.56,58 One trial used paddle electrodes,58 the other trial used manual pressure on top of adhesive electrodes.56 One trial enrolled patients with a body mass index of 30 kg/m2 or greater.56 Both trials applied escalating shocks. Antero-posterior pad positioning was used in one trial and there was an equal distribution of antero-posterior and antero-apical pad positioning in the other. Manual pressure increased initial cardioversion success (42 vs. 20%, RR 2.19, 95% CI 1.21–3.95, I2 = 34%, Figure 4A). Quality of evidence for initial cardioversion success was high (see Supplementary material online, Appendix S13).
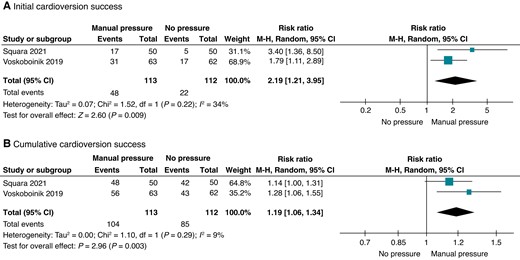
Forest plots for RCTs comparing manual pressure and no manual pressure. (A) Initial cardioversion success. (B) Cumulative cardioversion success.
The same two trials (225 participants) compared cumulative cardioversion success with and without manual pressure.56,58 Manual pressure application increased cumulative cardioversion success (92 vs. 76%, RR 1.19, 95% CI 1.06–1.34, I2 = 9%, Figure 4B). Quality of evidence for cumulative cardioversion success was high (see Supplementary material online, Appendix S13).
Other interventions
Nine trials (1031 participants) assessed cardioversion success with other techniques.59,60,62–65 None of these techniques impacted initial nor cumulative cardioversion success (see Supplementary material online, Appendix S10). These techniques included rectilinear/pulsed biphasic compared with biphasic truncated exponential waveform (initial: four trials, RR 1.11, 95% CI 0.91–1.34, I2 = 0%; cumulative: four trials, RR 0.98, 95% CI 0.89–1.08, I2 = 84%); and anterior pad as cathode compared with anterior pad as anode (cumulative success: two trials, RR 0.99, 95% CI 0.92–1.07, I2 = 15%). Supplementary material online, Appendix S13 summarizes the quality of evidence for these pooled estimates.
Adverse events
Reporting of adverse events varied between trials. Serious adverse events such as stroke (reported in one trial), pacemaker implantation (reported in one trial), and ventricular arrhythmia (reported in one trial) were rare (see Supplementary material online, Appendix S11).
Outcomes from observational studies
Biphasic and monophasic shock waveforms were compared in six observational studies (2081 participants). When compared with monophasic waveforms, biphasic waveforms were not associated with significant differences in initial (RR 1.03, 95% CI 0.97–1.09, I2= 68%) or cumulative (RR 1.12, 95% CI 0.97–1.29, I2 = 76%) cardioversion success. Fixed, high-energy protocols and escalating energy protocols were compared in two observational studies (779 participants). When compared with fixed, high-energy protocols, escalating energy protocols were associated with higher rates of final cardioversion success (RR 1.06, 95% CI 1.01–1.11, I2 = 0%). Antero-apical/lateral and antero-posterior pad positioning were compared in four observational studies (533 participants). When compared with antero-posterior pads, antero-apical/lateral pads were not associated with significant differences in initial (RR 1.07, 95% CI 0.89–1.29, I2= 55%) or cumulative cardioversion success (RR 1.04, 95% CI 0.98–1.10, I2= 0%). Manual pressure was assessed in two observational studies (915 participants). When compared with no pressure, manual pressure was not associated with significant differences in initial cardioversion success (RR 0.78, 95% CI 0.33–1.86, I2= 79%). However, manual pressure was associated with a higher rate of cumulative cardioversion success (RR 1.08, 95% CI 1.04–1.11, I2 = 4%). Studies that compared waveform properties found similar success with biphasic pulsed energy when compared with biphasic low energy waveform with pulsed biphasic and biphasic truncated exponential waveforms. Forest plots and data for these comparisons appear in Supplementary material online, Appendix S12.
Discussion
This systematic review and meta-analysis of randomized trials and observational studies identified three techniques that improve cardioversion success for patients with AF. Biphasic shock waveforms nearly doubled initial cardioversion success and increased cumulative success by about 10%. High-energy shocks using at least 200 J increased initial success by approximately 60%. Biphasic, high-energy shocks can increase efficacy and minimize the number of shocks needed for restoration of sinus rhythm. Manual pressure, which was studied primarily in obese patients, resulted in a two-fold increase in success and may be considered in these patients. The optimal electrode position remains unclear. No randomized trial has compared antero-posterior and antero-apical/lateral pad configurations while using biphasic, high-energy shocks.
Biphasic waveforms result in higher initial and cumulative shock success; we rated this evidence as high quality. These findings were consistent when tested across subgroups of biphasic waveform properties and pad position. The superiority of biphasic waveforms is hypothesized to stem from their ability to compensate for transthoracic impedance.32
Fixed, high-energy shocks result in higher initial cardioversion success; we rated this evidence as high quality. Escalating-energy protocols increase until reaching high energy; and as expected, have similar cumulative success as high-energy protocols. Observational series have suggested that this effect may be even more pronounced in patients with longer AF durations.67 Experimental studies on animals have suggested that lower energy settings may reduce skin burns, patient discomfort, and myocardial damage.68 However, such adverse events are rare in clinical practice.40–43 In contrast, minimizing the number of shocks is desirable because it requires less sedation, shortens the overall procedure time, and minimizes patient discomfort.14
Manual pressure with handheld paddles or active compression increases the efficacy of both initial and cumulative cardioversion; we rated this evidence as high quality. These interventions are hypothesized to lower thoracic impedance.69 Although we judged this evidence as high-quality based on the GRADE framework, it has limitations. These studies included only 225 patients, and one study was limited to obese patients.56,58 Clinicians may consider manual pressure using gloved hands on the first attempt in obese patients and during repeated attempts in others.
We found no difference in cardioversion success when comparing antero-posterior to antero-apical/lateral pad position. We rated this evidence as low quality for initial cardioversion success and moderate quality for cumulative success. Importantly, evidence for pad position is limited because it has not been studied in conjunction with the other two techniques known to be effective (i.e. maximal energy and biphasic shocks). Biological arguments support both configurations of pad placement. Antero-posterior placement may result in a more direct shock vector to the atria, resulting in reduced transthoracic impedance, except in patients with larger chests.57,70,71 In contrast, antero-apical/lateral pads may capture more myocardial cells overall.72 Because the effect could differ based on patient anatomy, clinicians may consider the opposite configuration when the first fails.
This review found no significant differences between the biphasic waveform subtypes or differing electrode polarity. These interventions seem unlikely to impact cardioversion success.
Clinical practice guidelines make a number of statements related to cardioversion techniques, but these have not been based on systematic reviews.5–8,73 The 2014 American Heart Association/American College of Cardiology Guidelines discuss high energy, biphasic waveforms, changing shock vectors, and applying pressure to improve energy delivery, but do not make practice recommendations.8,73 The 2020 Canadian Cardiovascular Society Guidelines recommend (strong recommendation; low-quality evidence) at least a 150 J biphasic waveform for electrical cardioversion.5 These guidelines discuss that pad positioning does not seem to impact efficacy and that manual pressure may facilitate cardioversion in obese patients. The 2020 European Society of Cardiology Guidelines discuss the superiority of biphasic waveforms, but do not make a practice recommendation.7 These guidelines also discuss that anterior–posterior pads are more effective, but offer the caveat that some studies have shown no difference. A practical guidance document that was published by the European Heart Rhythm Association in 2020 states that antero-posterior pad placement is more effective than antero-apical.6 The evidence provided by this systematic review will inform practice recommendations.
Strengths
This is the first systematic review to comprehensively summarize and appraise the evidence on techniques impacting cardioversion success.6,14,74–76 Our protocol was preregistered and our review assessed the methodological quality of individual studies. We used the GRADE approach to assess the quality of evidence. We performed subgroup analyses to assess interventions in the context of other co-interventions.
Limitations
The limitations of this review are inherent to the included studies. The main limitation was the heterogeneous combinations of interventions used in different studies. Although we attempted to assess this using subgroup analyses, these findings should be considered exploratory. Pre-treatment with anti-arrhythmic drugs also varied; it is established to improve acute and long-term success of cardioversion.15 Although included studies did not provide data on long-term maintenance of sinus rhythm, it seems unlikely that these interventions would affect this outcome. Finally, adverse effects were not consistently reported or were not specified across studies.
Conclusions
Biphasic shock waveforms, high-energy shocks, and manual pressure using paddle electrodes or applied on top of adhesive electrodes increase the efficacy of cardioversion of AF. Other interventions, particularly pad placement, require further study. Considering the variability in AF cardioversion success, these findings will help guide future research.
Supplementary material
Supplementary material is available at Europace online.
Acknowledgements
We would like to thank Jo-Anne Petropoulos (McMaster Health Sciences Library) for reviewing our search strategy, Anders Granholm for assessing articles written in Danish, Gera Kisselman for assessing articles written in Russian, Kevin Gu for assessing articles written in Chinese, Meliha Horzum for assessing articles written in Turkish, Omri Nachmani for assessing articles written in Hebrew, and Sergio Conti for assessing articles written in Italian.
Funding
None.
References
Author notes
Conflict of interest: None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}