





Abstract
Type of funding sources: None.
Leadless pacing has evolved as a safe and effective treatment option in selected patients. With the updated generation that allows sensing of atrial contraction, atrioventricular synchronized pacing is now possible in a VDD mode. Previous retrospective analyses have demonstrated that echocardiographic parameters may be helpful in selecting patients with a higher chance of good atrioventricular synchronous pacing behaviour.
Analysis of the early experience with the second generation of leadless pacemaker and the role of ECG parameters to predict a good atrial contraction signal (so-called A4 amplitude) in patients who underwent leadless pacemaker implantation in four tertiary centres.
In this retrospective analysis, a total of 136 patients were included. Mean age was 78.0 (64.7 - 84.2 years) years with 48.9 % being male. Coronary artery disease was the leading underlying heart disease with 27.1 % affected patients. 61.7 % of the population suffered from sinus rhythm with complete or intermittent atrioventricular block. The majority of devices were implanted at the mid-septal (61.2 %) or high-septal (25.6 %) right ventricle, respectively. Electrical parameters were optimal at implant (Table 1) and remained stable over time (Table 1). In addition, A4 signal amplitude remained stable too during follow-up compared to the value early after implantation (Table 1). From this entire cohort, patients with an ECG available at implant and those in which the device was working predominantly in the VDD mode were selected for further analyses (62 patients). PR interval measured from the ECG prior to implantation did not correlate with the A4 signal amplitude (Figure 1A; P = NS). Next, P wave amplitudes were measured in all 12 ECG leads. There was a correlation between P wave amplitude from lead V2 with the A4 amplitude (Figure 1B; P = 0.034, R2 = 0.09), whereas the other right-sided ECG leads (V1/aVR), either alone or in combination, did not correlate with the A4 signal amplitude (P = NS).
In our cohort of patients with the second generation of leadless pacemakers, offering VDD pacing, good electrical parameters can be achieved as it has been observed with the first generation. Also the A4 signal amplitude as a marker for atrial contraction remains stable over time. In regard to ECG parameters measured prior to device implantation, only the P wave amplitude in lead V2 correlated with a amplitude of the A4 signal.

Table 1
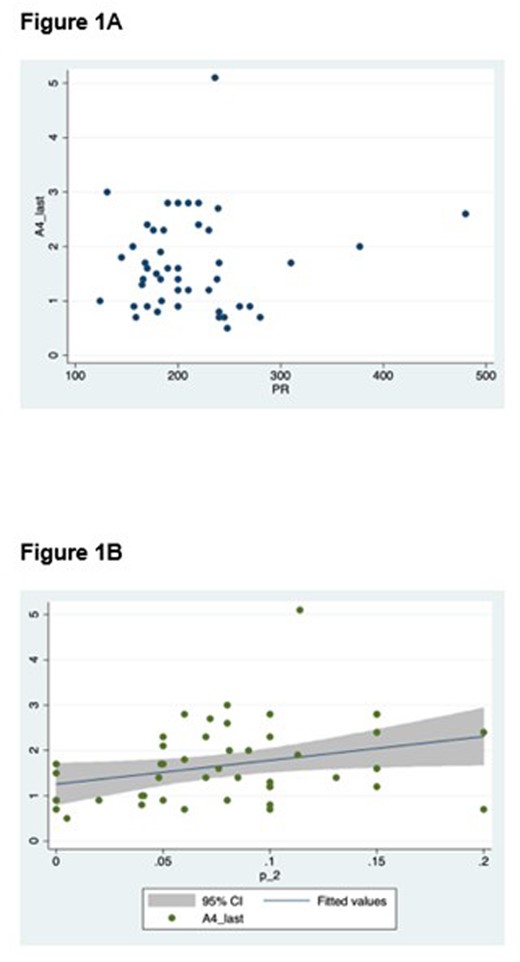
Figure 1

{kind=link}