





Abstract
Type of funding sources: Public hospital(s). Main funding source(s): Hospital Universitari Vall d"Hebron - Vall d"Hebron Institut de Recerca. CIBERCV
Patients with structural heart disease (SHD) or bundle branch block (BBB) are at high risk of having an arrhythmic syncope (AS). In patients with recurrent syncope episodes (RSE) complete work-up including electrophysiological study (EPS) and/or implantation of a loop recorder (ILR) is recommended, however patients with their first episode may also be at risk of an AS.
To determinate if the patients with SHD or BBB with a single syncope episode (SSE) are at high risk of having an AS and compare it with patients with recurrent episodes (RSE).
METHODS Cohort study carried out in a tertiary hospital that is a reference centre for syncope. From January 2008 to August 2020 patients with SHD or BBB with syncope of unknown origin after the initial evaluation and without direct indication of an ICD were included. They were managed according the current ESC guidelines.
417patients were included (74 ±11 y. o; 39% female). Mean follow up was 2.5 ±1 y. 223 patients were diagnosed from an AS [113 (53%) in SSE group and 110 (54%) in RSE group, p = 0.9], 210 were due to bradyarrhythmia (AV block or sinus arrest). No differences in baseline characteristics where found comparing both groups, except that BBB was slightly more prevalent in patients with RSE (81% vs 90%, p = 0.01) (FIGURE- PANEL A). Risk of AS was 53% in patients with SE and 54% (p = 0.9). RSE were not associated with an increased risk of AS in univariate analyses (OR 1.01 IC95% 0.7-1.5) neither in the multivariate (FIGURE- PANEL B). EPS and ILR diagnostic yield was 45% / 32% respectively in SSE group and 44% / 33% in RSE group (p = 0.8) (FIGURE - PANEL C). After appropriate treatment, recurrence syncope rate was 10% in SSE group and 9% in RSE group (p = 0.8). No significant differences in mortality rate were found.
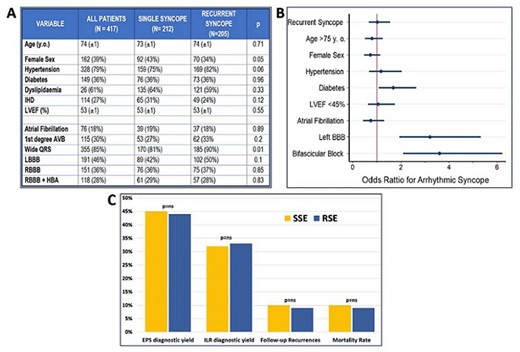
Abstract Figure

{kind=link}