





Background: Non-ambulatory heart failure (HF) patients have been traditionally excluded from major cardiac resynchronization therapy (CRT) clinical trials, and thus lie outside guideline recommendations. Nevertheless, in clinical practice, CRT implantation is occasionally considered for patients during an unscheduled admission for decompensated heart failure.
Purpose: To compare one-year outcomes in advanced heart failure patients implanted with CRT during an unscheduled heart failure admission with outcomes in ambulatory HF patients.
Methods: We retrospectively reviewed baseline data and first year outcomes of all patients undergoing CRT implantation, between 2006 and 2014, at two Spanish referral hospitals. CRT echocardiographic responders were defined as patients who were alive at 1 year and had experienced a reduction of at least 15 % in left ventricular end-systolic volume. Outcomes were compared between patients undergoing implantation during an unscheduled HF admission and ambulatory patients.
Results: Of 254 patients undergoing CRT implantation, 37 (14.6 %) were advanced HF patients implanted during an unplanned HF admission. Baseline characteristics and one-year outcomes are summarized in the table. Regarding non-ambulatory patients, the device was succesfully implanted in 31 patients (83.8 %) with 10 patients experiencing procedure-related complications (27 %). One patient died during the index admission. Amongst non-ambulatory patients, total one-year mortality and re-admission rates were 24.3 % and 51.4 %, and 32.4 % of patients were considered echo responders at 12 months. The corresponding rates for ambulatory patients were 1.1%, 14 % and 61.1 %, respectively (p < 0.05 for all comparisons).
Conclusions: Despite high survival to discharge rates, advanced heart failure patients undergoing CRT implantation during an unscheduled heart failure admission present significantly worse one-year outcomes compared to ambulatory patients.
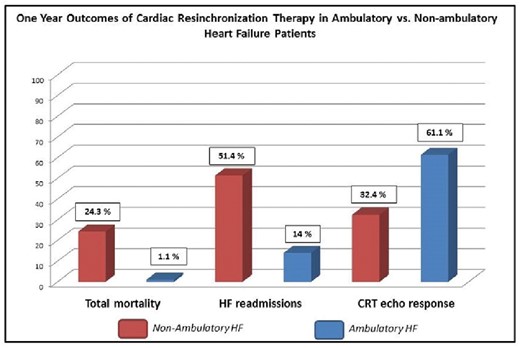
Abstract P440 Figure.

{kind=link}