





Abstract
To assess different aspects of the definition of valvular/non-valvular atrial fibrillation (AF) used in clinical practice by physicians who usually treat this condition.
We prospectively conducted a web-based survey including cardiologists and internists who attended continuing medical education courses on cardiovascular medicine. A questionnaire was drawn up, containing 17 questions clustered into five main topics: (A) known rheumatic aetiology; (B) site/type of valve involvement; (C) prosthetic heart valve; (D) haemodynamic relevance; (E) miscellaneous. The overall response rate was 22.4% (21.1% for cardiologists and 24% for internists). Coexistence of both medical history of rheumatic disease and clinical signs of valvular involvement were considered as essential prerequisites for the diagnosis of rheumatic AF by half of the respondents, and one-third assumed that lone aortic valve disease was sufficient for AF to be defined as valvular. A similar proportion of respondents considered that in the presence of mitral regurgitation, AF had to be defined as valvular. The majority of responding physicians considered the degree of valvular defect of lesser importance for the definition of valvular or non-valvular origin of AF.
We found important heterogeneity and uncertainties in the answers given by physicians who usually treat patients with AF, as evidence of the lack of precise and unique definitions of the origin of AF (valvular/non-valvular). It is urgent to issue clear widely accepted definitions of the origin of AF, which should improve clinical practice and research.
There is no study focusing on the definition of valvular and non-valvular atrial fibrillation (AF), except for a few international guidelines on the management of AF, which marginally address this issue. The choice of the proper anti-thrombotic regimen for stroke prevention in AF is strictly linked to the definition of the origin of AF.
The present survey shows that the meaning of the term ‘AF of valvular (or non-valvular) origin’ is far from clear to cardiologists and internists who deal with AF.
Widely accepted and shared definitions of valvular AF and non-valvular AF are needed to improve clinical practice and research.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, occurring in 1–2% of the general population, and its prevalence is estimated to double in the next 50 years as the population ages. Atrial fibrillation is associated with increased rates of death, stroke, and other thrombo-embolic events.1–3 For many years, oral anticoagulant therapy with vitamin K antagonists (VKAs) has been administered to patients affected by AF associated with mechanical prosthetic heart valves or valvular heart disease (VHD) for prevention of stroke and systemic embolism. Over the past 25 years, based on strong evidence, the prevention of stroke with VKAs has also been extended to patients with so-called non-valvular AF (NVAF).4
The referred proportion of patients with valvular AF ranges from 4 to 30% of all patients with AF.5,6 This variability is mostly due to the lack of a unique definition of what valvular or non-valvular AF is. This problem has so far been of limited relevance because VKAs represented the only available therapeutic option.
Things have changed since the introduction of novel oral anticoagulants (NOACs). Overall, NOACs are as effective as warfarin for stroke prevention in AF (SPAF) and cause less intracranial bleeding.7–10 On this basis, recent guidelines recommend NOACs as preferable to VKAs in the majority of patients with NVAF.1 Yet the evidences support their use only in patients with NVAF, such as defined in the inclusion criteria of these clinical trials. The RE-ALIGN study results advise against the use of the NOAC dabigatran in patients with mechanical heart valve prostheses.11 Definitions of valvular/non-valvular AF adopted by authoritative guidelines have changed in their different editions and sometimes they are in contradiction with each other.1–3 Studies on the definition of valvular/non-valvular AF are lacking.
We performed this prospective survey to assess different aspects of the definition of valvular/non-valvular AF, commonly used by physicians who treat this condition, and to identify eventual gaps in the current conceptual and working definitions.
Methods
Study type and sampling
We prospectively conducted a web-based survey on the opinion that a group of physicians had about the definition of NVAF. The study population was selected from a database composed of medical specialists who attended national continuing medical education (CME) courses on cardiovascular medicine, in 2011 and 2012. The questionnaire was sent to those who had provided their email address (1295 cardiologists and 998 internists). The survey was based on voluntary participation and no grant was provided to the respondents.
Questionnaire development
To build up the survey questionnaire, we first identified the main guidelines on AF with the respective definitions of valvular or non-valvular AF. AHA/ACC/ESC 2001 AF guideline stated that ‘By convention, the term non-valvular AF is restricted to cases in which the rhythm disturbance occurs in the absence of rheumatic mitral valve disease or a prosthetic heart valve’, and 2006 update adds ‘… or mitral valve repair’. The 2012 focused update of the ESC Guidelines for the management of AF stated ‘In this guideline, the term valvular AF is used to imply that AF is related to rheumatic valvular disease (predominantly mitral stenosis) or prosthetic heart valves …’.
An indirect definition of valvular/non-valvular was also provided by the most recent clinical trials on SPAF, comparing NOACs to warfarin. In the main trials, the exclusion criteria were: On these bases, we identified five main topics that are crucial in the definition of valvular or non-valvular AF: A 17 queries questionnaire (see Table 1) was built-up to assess physicians' opinion, clustering the questions as follows: 2 introductory questions (an estimate of the percentage of patients suffering from valvular AF, and about the perception of the clarity of existing definitions of NVAF); 4 questions each onTopics A, B, and D; 1 question on Topic C; and 2 questions on Topic E (see Supplementary material online, Appendix for the extended version of Table 1).
RE-LYtrial:7 ‘… history of heart valve disorders (i.e., prosthetic valve or hemodynamically relevant valve disease) … ’;
ROCKET-AFtrial:8 ‘… hemodynamically significant mitral valve stenosis. Prosthetic heart valve (annuloplasty with or without prosthetic ring, commissurotomy and/or valvuloplasty are permitted) …’;
ARISTOTLEtrial:9 ‘Key exclusion criteria were … moderate or severe mitral stenosis, conditions other than atrial fibrillation that required anticoagulation (e.g., a prosthetic heart valve) …’;
ENGAGE AFtrial:10 ‘Key exclusion criteria were … moderate-to severe mitral stenosis …’.
The presence/absence of a known rheumatic aetiology as origin of valvular disease.
Site (mitral, aortic) and type of valve involvement (stenosis, regurgitation, both).
The presence/absence of prosthetic heart valve.
Haemodynamic relevance (severe/moderate/mild stenosis or regurgitation).
Miscellaneous questions (clarity of existing definitions of NVAF, classification of AF due to reversible causes, role of left atrial enlargement).
Queries of the survey (short version)
| Q1. Make an estimate of the percentage of patients suffering from valvular AF: <5%, 5–9%, 10–19%, or >20% |
| Q2. Do you think that the existing definitions of NVAF are sufficiently clear? |
| (a) The presence/absence of a known rheumatic aetiology as origin of valvular disease |
| Q3. Are the terms NVAF and non-rheumatic AF synonyms? |
| Q4. Are medical history of rheumatic disease and clinical signs of valvular involvement both prerequisites to define AF as rheumatic? |
| Q5. In the absence of clinical history of rheumatic disease and in the presence of a documented valvular anomaly, may AF then be defined as valvular? |
| Q6. In a patient with mitral valve disease of unclear origin, may AF then be defined as valvular? |
| (b) Site (mitral, aortic) and type of valve involvement (stenosis, insufficiency, both) |
| Q7. In the presence of VHD other than mitral, may AF then be defined as valvular? |
| Q8. In a patient with rheumatic VHD, may AF then be classified as valvular if associated with mitral involvement or aortic involvement or both? |
| Q9. The term ‘AF associated to rheumatic mitral valve disease’ includes: regurgitation or stenosis or both |
| Q10. In the presence of with mitral valve regurgitation, may AF than be defined as valvular? |
| (c) The presence/absence of prosthetic heart valve |
| Q11. In the presence of a biological aortic valve prosthesis, may AF then be defined as a valvular AF? |
| (d) Haemodynamic relevance (severe/moderate/mild stenosis or insufficiency) |
| Q12. Is the degree of valvular stenosis or regurgitation relevant for the definition of valvular AF? |
| Q13. Is the degree of valvular regurgitation relevant for the definition of valvular AF? |
| Q14. Is the degree of valvular stenosis the only relevant parameter for the definition of valvular AF? |
| Q15. In case of AF and mitral stenosis, is the degree of stenosis relevant for the definition of valvular AF? |
| (e) Miscellaneous |
| Q16. Should AF during hyperthyroidism or post-surgery AF be considered as NVAF? |
| Q17. Is the degree of left atrium enlargement important to define the origin of AF (valvular vs. non-valvular)? |
| Q1. Make an estimate of the percentage of patients suffering from valvular AF: <5%, 5–9%, 10–19%, or >20% |
| Q2. Do you think that the existing definitions of NVAF are sufficiently clear? |
| (a) The presence/absence of a known rheumatic aetiology as origin of valvular disease |
| Q3. Are the terms NVAF and non-rheumatic AF synonyms? |
| Q4. Are medical history of rheumatic disease and clinical signs of valvular involvement both prerequisites to define AF as rheumatic? |
| Q5. In the absence of clinical history of rheumatic disease and in the presence of a documented valvular anomaly, may AF then be defined as valvular? |
| Q6. In a patient with mitral valve disease of unclear origin, may AF then be defined as valvular? |
| (b) Site (mitral, aortic) and type of valve involvement (stenosis, insufficiency, both) |
| Q7. In the presence of VHD other than mitral, may AF then be defined as valvular? |
| Q8. In a patient with rheumatic VHD, may AF then be classified as valvular if associated with mitral involvement or aortic involvement or both? |
| Q9. The term ‘AF associated to rheumatic mitral valve disease’ includes: regurgitation or stenosis or both |
| Q10. In the presence of with mitral valve regurgitation, may AF than be defined as valvular? |
| (c) The presence/absence of prosthetic heart valve |
| Q11. In the presence of a biological aortic valve prosthesis, may AF then be defined as a valvular AF? |
| (d) Haemodynamic relevance (severe/moderate/mild stenosis or insufficiency) |
| Q12. Is the degree of valvular stenosis or regurgitation relevant for the definition of valvular AF? |
| Q13. Is the degree of valvular regurgitation relevant for the definition of valvular AF? |
| Q14. Is the degree of valvular stenosis the only relevant parameter for the definition of valvular AF? |
| Q15. In case of AF and mitral stenosis, is the degree of stenosis relevant for the definition of valvular AF? |
| (e) Miscellaneous |
| Q16. Should AF during hyperthyroidism or post-surgery AF be considered as NVAF? |
| Q17. Is the degree of left atrium enlargement important to define the origin of AF (valvular vs. non-valvular)? |
Queries of the survey (short version)
| Q1. Make an estimate of the percentage of patients suffering from valvular AF: <5%, 5–9%, 10–19%, or >20% |
| Q2. Do you think that the existing definitions of NVAF are sufficiently clear? |
| (a) The presence/absence of a known rheumatic aetiology as origin of valvular disease |
| Q3. Are the terms NVAF and non-rheumatic AF synonyms? |
| Q4. Are medical history of rheumatic disease and clinical signs of valvular involvement both prerequisites to define AF as rheumatic? |
| Q5. In the absence of clinical history of rheumatic disease and in the presence of a documented valvular anomaly, may AF then be defined as valvular? |
| Q6. In a patient with mitral valve disease of unclear origin, may AF then be defined as valvular? |
| (b) Site (mitral, aortic) and type of valve involvement (stenosis, insufficiency, both) |
| Q7. In the presence of VHD other than mitral, may AF then be defined as valvular? |
| Q8. In a patient with rheumatic VHD, may AF then be classified as valvular if associated with mitral involvement or aortic involvement or both? |
| Q9. The term ‘AF associated to rheumatic mitral valve disease’ includes: regurgitation or stenosis or both |
| Q10. In the presence of with mitral valve regurgitation, may AF than be defined as valvular? |
| (c) The presence/absence of prosthetic heart valve |
| Q11. In the presence of a biological aortic valve prosthesis, may AF then be defined as a valvular AF? |
| (d) Haemodynamic relevance (severe/moderate/mild stenosis or insufficiency) |
| Q12. Is the degree of valvular stenosis or regurgitation relevant for the definition of valvular AF? |
| Q13. Is the degree of valvular regurgitation relevant for the definition of valvular AF? |
| Q14. Is the degree of valvular stenosis the only relevant parameter for the definition of valvular AF? |
| Q15. In case of AF and mitral stenosis, is the degree of stenosis relevant for the definition of valvular AF? |
| (e) Miscellaneous |
| Q16. Should AF during hyperthyroidism or post-surgery AF be considered as NVAF? |
| Q17. Is the degree of left atrium enlargement important to define the origin of AF (valvular vs. non-valvular)? |
| Q1. Make an estimate of the percentage of patients suffering from valvular AF: <5%, 5–9%, 10–19%, or >20% |
| Q2. Do you think that the existing definitions of NVAF are sufficiently clear? |
| (a) The presence/absence of a known rheumatic aetiology as origin of valvular disease |
| Q3. Are the terms NVAF and non-rheumatic AF synonyms? |
| Q4. Are medical history of rheumatic disease and clinical signs of valvular involvement both prerequisites to define AF as rheumatic? |
| Q5. In the absence of clinical history of rheumatic disease and in the presence of a documented valvular anomaly, may AF then be defined as valvular? |
| Q6. In a patient with mitral valve disease of unclear origin, may AF then be defined as valvular? |
| (b) Site (mitral, aortic) and type of valve involvement (stenosis, insufficiency, both) |
| Q7. In the presence of VHD other than mitral, may AF then be defined as valvular? |
| Q8. In a patient with rheumatic VHD, may AF then be classified as valvular if associated with mitral involvement or aortic involvement or both? |
| Q9. The term ‘AF associated to rheumatic mitral valve disease’ includes: regurgitation or stenosis or both |
| Q10. In the presence of with mitral valve regurgitation, may AF than be defined as valvular? |
| (c) The presence/absence of prosthetic heart valve |
| Q11. In the presence of a biological aortic valve prosthesis, may AF then be defined as a valvular AF? |
| (d) Haemodynamic relevance (severe/moderate/mild stenosis or insufficiency) |
| Q12. Is the degree of valvular stenosis or regurgitation relevant for the definition of valvular AF? |
| Q13. Is the degree of valvular regurgitation relevant for the definition of valvular AF? |
| Q14. Is the degree of valvular stenosis the only relevant parameter for the definition of valvular AF? |
| Q15. In case of AF and mitral stenosis, is the degree of stenosis relevant for the definition of valvular AF? |
| (e) Miscellaneous |
| Q16. Should AF during hyperthyroidism or post-surgery AF be considered as NVAF? |
| Q17. Is the degree of left atrium enlargement important to define the origin of AF (valvular vs. non-valvular)? |
Most of the questions were based on a multiple choice format with ‘Yes’, ‘No’, and ‘I don't know’ as possible answers. It was decided to focus the analysis on the percentage of affirmative responses, as the details of the percentages of the remaining options would not have helped in illustrating respondents' opinions. Exceptions existed in Questions 1, 8, 9, and 11, for which meaningful response formats were chosen: Q8: ‘Only mitral involvement’; Q9: ‘Mitral valvular regurgitation’; Q11: ‘Valvular AF’; for Question 1, the responses: ‘<5%’, ‘5–9%’, and ‘10–19%’ were considered as a single modality: ‘<20%’.
Data analysis
The answers to all returned questionnaires were summarized through frequency counts and percentages; frequencies of missing responses were also included in the calculations and reported for each question. A 95% confidence interval of the proportion (exact method) was reported for each response modality.
To assess the equivalence of responses between cardiologists and internists, the 95% confidence interval of the difference between proportions for each question was reported. A value Δ = 0.1 was used as equivalence criterion, thus the equivalence range has been defined as: (−0.1, 0.1). Non-equivalence was rejected when the confidence interval lie within the equivalence range. Confidence intervals were obtained according to Newcombe's method without continuity correction (Method 10).12
The statistical analysis was performed using software R13 with the Epi package14 added.
Results
Of the 2243 questionnaires sent, a total of 513 (22.4%) were returned and were available for study analysis. Responding rates were 21.1% (273 out of 1295) for cardiologists and 24% (240 out of 998) for internists (P = NS, χ2 test). Eighty-five per cent of respondents worked in a hospital setting. No differences were found between respondents and non-respondents (P = NS, χ2 test), on the years of job experience and the practice setting (hospital vs. non-hospital).
Nearly 52% of the respondents estimated that AF of valvular origin would account for <20% of the total (Q1); one-third of the respondents did not answer and <20% think that >20% of AF have a valvular origin (see Table 2).
Answers to Question 1
| (Q1) At present, NVAF can be treated with NOACs, while for valvular AF the only therapeutic resource is VKAs. Make an estimate of the percentage of patients with AF in clinical practice that will still require therapy with VKAs because suffering from valvular AF | Cardiologists | Internists | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| <5% | 21 (7.7) | (4.8–11.5) | 33 (13.8) | (9.7–18.8) |
| 5–9% | 68 (24.9) | (19.9–30.5) | 52 (21.7) | (16.6– 27.4) |
| 10–19% | 51 (18.7) | (14.2–23.8) | 40 (16.7) | (12.2–22.0) |
| >20% | 51 (18.7) | (14.2–23.8) | 33 (13.8) | (9.7–18.8) |
| No answer | 82 (30.0) | (24.7–35.9) | 82 (34.2) | (28.2–40.5) |
| Total | 273 (100.0) | 240 (100.0) | ||
| (Q1) At present, NVAF can be treated with NOACs, while for valvular AF the only therapeutic resource is VKAs. Make an estimate of the percentage of patients with AF in clinical practice that will still require therapy with VKAs because suffering from valvular AF | Cardiologists | Internists | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| <5% | 21 (7.7) | (4.8–11.5) | 33 (13.8) | (9.7–18.8) |
| 5–9% | 68 (24.9) | (19.9–30.5) | 52 (21.7) | (16.6– 27.4) |
| 10–19% | 51 (18.7) | (14.2–23.8) | 40 (16.7) | (12.2–22.0) |
| >20% | 51 (18.7) | (14.2–23.8) | 33 (13.8) | (9.7–18.8) |
| No answer | 82 (30.0) | (24.7–35.9) | 82 (34.2) | (28.2–40.5) |
| Total | 273 (100.0) | 240 (100.0) | ||
In the table, the number of subjects, the percentage, and corresponding 95% confidence interval (95% CI) are reported for each modality of response.
Answers to Question 1
| (Q1) At present, NVAF can be treated with NOACs, while for valvular AF the only therapeutic resource is VKAs. Make an estimate of the percentage of patients with AF in clinical practice that will still require therapy with VKAs because suffering from valvular AF | Cardiologists | Internists | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| <5% | 21 (7.7) | (4.8–11.5) | 33 (13.8) | (9.7–18.8) |
| 5–9% | 68 (24.9) | (19.9–30.5) | 52 (21.7) | (16.6– 27.4) |
| 10–19% | 51 (18.7) | (14.2–23.8) | 40 (16.7) | (12.2–22.0) |
| >20% | 51 (18.7) | (14.2–23.8) | 33 (13.8) | (9.7–18.8) |
| No answer | 82 (30.0) | (24.7–35.9) | 82 (34.2) | (28.2–40.5) |
| Total | 273 (100.0) | 240 (100.0) | ||
| (Q1) At present, NVAF can be treated with NOACs, while for valvular AF the only therapeutic resource is VKAs. Make an estimate of the percentage of patients with AF in clinical practice that will still require therapy with VKAs because suffering from valvular AF | Cardiologists | Internists | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| <5% | 21 (7.7) | (4.8–11.5) | 33 (13.8) | (9.7–18.8) |
| 5–9% | 68 (24.9) | (19.9–30.5) | 52 (21.7) | (16.6– 27.4) |
| 10–19% | 51 (18.7) | (14.2–23.8) | 40 (16.7) | (12.2–22.0) |
| >20% | 51 (18.7) | (14.2–23.8) | 33 (13.8) | (9.7–18.8) |
| No answer | 82 (30.0) | (24.7–35.9) | 82 (34.2) | (28.2–40.5) |
| Total | 273 (100.0) | 240 (100.0) | ||
In the table, the number of subjects, the percentage, and corresponding 95% confidence interval (95% CI) are reported for each modality of response.
To the question (Q2) if the existing definitions of NVAF (e.g. Guidelines) were sufficiently clear, cardiologists had more doubts than internists: just one half of the cardiologists answered yes compared with more than two-thirds of internists (see Table 3).
Answers to Question 2
| (Q2) Do you think that the existing definitions of NVAF are sufficiently clear? | Cardiologists | Internists | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| No | 98 (35.9) | (30.2–41.9) | 69 (28.8) | (23.1–34.9) |
| Yes | 156 (57.1) | (51.0–63.1) | 163 (67.9) | (61.6–73.8) |
| No answer | 19 (7.0) | (4.2–10.7) | 8 (3.3) | (1.4–6.5) |
| Total | 273 (100.0) | 240 (100.0) | ||
| (Q2) Do you think that the existing definitions of NVAF are sufficiently clear? | Cardiologists | Internists | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| No | 98 (35.9) | (30.2–41.9) | 69 (28.8) | (23.1–34.9) |
| Yes | 156 (57.1) | (51.0–63.1) | 163 (67.9) | (61.6–73.8) |
| No answer | 19 (7.0) | (4.2–10.7) | 8 (3.3) | (1.4–6.5) |
| Total | 273 (100.0) | 240 (100.0) | ||
In the table, the number of subjects, the percentage, and corresponding 95% confidence interval (95% CI) are reported for each modality of response.
Answers to Question 2
| (Q2) Do you think that the existing definitions of NVAF are sufficiently clear? | Cardiologists | Internists | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| No | 98 (35.9) | (30.2–41.9) | 69 (28.8) | (23.1–34.9) |
| Yes | 156 (57.1) | (51.0–63.1) | 163 (67.9) | (61.6–73.8) |
| No answer | 19 (7.0) | (4.2–10.7) | 8 (3.3) | (1.4–6.5) |
| Total | 273 (100.0) | 240 (100.0) | ||
| (Q2) Do you think that the existing definitions of NVAF are sufficiently clear? | Cardiologists | Internists | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| No | 98 (35.9) | (30.2–41.9) | 69 (28.8) | (23.1–34.9) |
| Yes | 156 (57.1) | (51.0–63.1) | 163 (67.9) | (61.6–73.8) |
| No answer | 19 (7.0) | (4.2–10.7) | 8 (3.3) | (1.4–6.5) |
| Total | 273 (100.0) | 240 (100.0) | ||
In the table, the number of subjects, the percentage, and corresponding 95% confidence interval (95% CI) are reported for each modality of response.
Figure 1 shows the 95% confidence intervals of the differences in proportions between responses given by cardiologists and internists. Non-equivalence was rejected for Questions 1, 3, 8, 12, 14, 15, and 17.
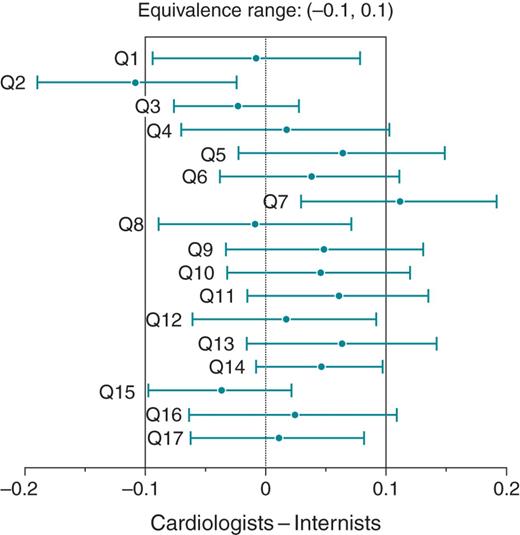
Equivalence of responses between cardiologists and internists. The figure shows estimates and respective 95% confidence intervals of the difference in proportions for selected response modalities (questions: Q1–Q17). The evidence of equivalence of the percentage of answer is shown only if the 95% confidence interval lies within the equivalence range.
The dominant answers to the questions are presented in Table 4; see the extended version of Table 4 in the Supplementary material online, for the distribution of the percentage of all the answers.
Dominant answers grouped according to the five main topics, and by physicians' specialties
| Clustering topics/questions | Cardiologists (n = 273) | Internists (n = 240) | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| (a) The presence/absence of a known rheumatic aetiology as origin of valvular disease | ||||
| Q3. Are the terms NVAF and non-rheumatic AF synonyms? | ||||
| No, n (%) | 163 (59.7) | (53.6–65.6) | 138 (57.5) | (51.0–63.8) |
| Q4. Are medical history of rheumatic disease and clinical signs of valvular involvement both prerequisites to define AF as rheumatic? | ||||
| Yes, n (%) | 133 (48.7) | (42.6–54.8) | 113 (47.1) | (40.6–53.6) |
| Q5. In the absence of clinical history of rheumatic disease and in the presence of a documented valvular anomaly, may AF then be defined as valvular? | ||||
| Yes, n (%) | 156 (57.1) | (51.0–63.1) | 122 (50.8) | (44.3–57.3) |
| Q6. In a patient with mitral valve disease of unclear origin, may AF then be defined as valvular? | ||||
| No, n (%) | 65 (23.8) | (18.9–29.3) | 67 (27.9) | (22.3–34.1) |
| (b) Site (mitral, aortic) and type of valve involvement (stenosis, insufficiency, both) | ||||
| Q7. In the presence of VHD other than mitral, may AF then be defined as valvular? | ||||
| Yes, n (%) | 110 (40.3) | (34.4–46.4) | 70 (29.2) | (23.5–35.4) |
| Q8. In a patient with rheumatic VHD, may AF then be classified as valvular if associated with mitral involvement or aortic involvement or both? | ||||
| Aortic and mitral involvement, n (%) | 129 (47.3) | (41.2–53.4) | 95 (39.6) | (33.4–46.1) |
| Q9. The term ‘AF associated to rheumatic mitral valve disease’ includes | ||||
| Both of them, n (%) | 185 (67.8) | (61.9–73.3) | 151 (62.9) | (56.5–69.0) |
| Q10. In the presence of with mitral valve regurgitation, may AF than be defined as valvular? | ||||
| Yes, n (%) | 77 (28.2) | (22.9–33.9) | 57 (23.8) | (18.5–29.6) |
| (c) The presence/absence of prosthetic heart valve | ||||
| Q11. In the presence of a biological aortic valve prosthesis, how may AF then be defined? | ||||
| NVAF, n (%) | 73 (26.7) | (21.6–32.4) | 77 (32.1) | (26.2–38.4) |
| (d) Haemodynamic relevance (severe/moderate/mild stenosis or insufficiency) | ||||
| Q12. Is the degree of valvular stenosis or regurgitation relevant for the definition of valvular AF? | ||||
| No, n (%) | 98 (35.9) | (30.2–41.9) | 69 (28.8) | (23.1–34.9) |
| Q13. Is the degree of valvular regurgitation relevant for the definition of valvular AF? | ||||
| Yes, n (%) | 89 (32.6) | (27.1–38.5) | 63 (26.2) | (20.8–32.3) |
| Q14. Is the degree of valvular stenosis the only relevant parameter for the definition of valvular AF? | ||||
| No, n (%) | 150 (54.9) | (48.8–60.9) | 116 (48.3) | (41.9–54.9) |
| Q15. In case of AF and mitral stenosis, is the degree of stenosis relevant for the definition of valvular AF? | ||||
| No, n (%) | 118 (43.2) | (37.3–49.3) | 92 (38.3) | (32.2–44.8) |
| (e) Miscellaneous | ||||
| Q16. Should AF during hyperthyroidism or post-surgery AF be considered as NVAF? | ||||
| Yes, n (%) | 144 (52.7) | (46.6–58.8) | 121 (50.4) | (43.9–56.9) |
| Q17. Is the degree of left atrium enlargement important to define the origin of AF? | ||||
| No, n (%) | 85 (31.1) | (17.5–27.8) | 78 (32.5) | (21.2–32.7) |
| Clustering topics/questions | Cardiologists (n = 273) | Internists (n = 240) | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| (a) The presence/absence of a known rheumatic aetiology as origin of valvular disease | ||||
| Q3. Are the terms NVAF and non-rheumatic AF synonyms? | ||||
| No, n (%) | 163 (59.7) | (53.6–65.6) | 138 (57.5) | (51.0–63.8) |
| Q4. Are medical history of rheumatic disease and clinical signs of valvular involvement both prerequisites to define AF as rheumatic? | ||||
| Yes, n (%) | 133 (48.7) | (42.6–54.8) | 113 (47.1) | (40.6–53.6) |
| Q5. In the absence of clinical history of rheumatic disease and in the presence of a documented valvular anomaly, may AF then be defined as valvular? | ||||
| Yes, n (%) | 156 (57.1) | (51.0–63.1) | 122 (50.8) | (44.3–57.3) |
| Q6. In a patient with mitral valve disease of unclear origin, may AF then be defined as valvular? | ||||
| No, n (%) | 65 (23.8) | (18.9–29.3) | 67 (27.9) | (22.3–34.1) |
| (b) Site (mitral, aortic) and type of valve involvement (stenosis, insufficiency, both) | ||||
| Q7. In the presence of VHD other than mitral, may AF then be defined as valvular? | ||||
| Yes, n (%) | 110 (40.3) | (34.4–46.4) | 70 (29.2) | (23.5–35.4) |
| Q8. In a patient with rheumatic VHD, may AF then be classified as valvular if associated with mitral involvement or aortic involvement or both? | ||||
| Aortic and mitral involvement, n (%) | 129 (47.3) | (41.2–53.4) | 95 (39.6) | (33.4–46.1) |
| Q9. The term ‘AF associated to rheumatic mitral valve disease’ includes | ||||
| Both of them, n (%) | 185 (67.8) | (61.9–73.3) | 151 (62.9) | (56.5–69.0) |
| Q10. In the presence of with mitral valve regurgitation, may AF than be defined as valvular? | ||||
| Yes, n (%) | 77 (28.2) | (22.9–33.9) | 57 (23.8) | (18.5–29.6) |
| (c) The presence/absence of prosthetic heart valve | ||||
| Q11. In the presence of a biological aortic valve prosthesis, how may AF then be defined? | ||||
| NVAF, n (%) | 73 (26.7) | (21.6–32.4) | 77 (32.1) | (26.2–38.4) |
| (d) Haemodynamic relevance (severe/moderate/mild stenosis or insufficiency) | ||||
| Q12. Is the degree of valvular stenosis or regurgitation relevant for the definition of valvular AF? | ||||
| No, n (%) | 98 (35.9) | (30.2–41.9) | 69 (28.8) | (23.1–34.9) |
| Q13. Is the degree of valvular regurgitation relevant for the definition of valvular AF? | ||||
| Yes, n (%) | 89 (32.6) | (27.1–38.5) | 63 (26.2) | (20.8–32.3) |
| Q14. Is the degree of valvular stenosis the only relevant parameter for the definition of valvular AF? | ||||
| No, n (%) | 150 (54.9) | (48.8–60.9) | 116 (48.3) | (41.9–54.9) |
| Q15. In case of AF and mitral stenosis, is the degree of stenosis relevant for the definition of valvular AF? | ||||
| No, n (%) | 118 (43.2) | (37.3–49.3) | 92 (38.3) | (32.2–44.8) |
| (e) Miscellaneous | ||||
| Q16. Should AF during hyperthyroidism or post-surgery AF be considered as NVAF? | ||||
| Yes, n (%) | 144 (52.7) | (46.6–58.8) | 121 (50.4) | (43.9–56.9) |
| Q17. Is the degree of left atrium enlargement important to define the origin of AF? | ||||
| No, n (%) | 85 (31.1) | (17.5–27.8) | 78 (32.5) | (21.2–32.7) |
In the table, the number of subjects, the percentage, and corresponding 95% confidence interval (95% CI) are reported of the dominant answer to the questions.
Dominant answers grouped according to the five main topics, and by physicians' specialties
| Clustering topics/questions | Cardiologists (n = 273) | Internists (n = 240) | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| (a) The presence/absence of a known rheumatic aetiology as origin of valvular disease | ||||
| Q3. Are the terms NVAF and non-rheumatic AF synonyms? | ||||
| No, n (%) | 163 (59.7) | (53.6–65.6) | 138 (57.5) | (51.0–63.8) |
| Q4. Are medical history of rheumatic disease and clinical signs of valvular involvement both prerequisites to define AF as rheumatic? | ||||
| Yes, n (%) | 133 (48.7) | (42.6–54.8) | 113 (47.1) | (40.6–53.6) |
| Q5. In the absence of clinical history of rheumatic disease and in the presence of a documented valvular anomaly, may AF then be defined as valvular? | ||||
| Yes, n (%) | 156 (57.1) | (51.0–63.1) | 122 (50.8) | (44.3–57.3) |
| Q6. In a patient with mitral valve disease of unclear origin, may AF then be defined as valvular? | ||||
| No, n (%) | 65 (23.8) | (18.9–29.3) | 67 (27.9) | (22.3–34.1) |
| (b) Site (mitral, aortic) and type of valve involvement (stenosis, insufficiency, both) | ||||
| Q7. In the presence of VHD other than mitral, may AF then be defined as valvular? | ||||
| Yes, n (%) | 110 (40.3) | (34.4–46.4) | 70 (29.2) | (23.5–35.4) |
| Q8. In a patient with rheumatic VHD, may AF then be classified as valvular if associated with mitral involvement or aortic involvement or both? | ||||
| Aortic and mitral involvement, n (%) | 129 (47.3) | (41.2–53.4) | 95 (39.6) | (33.4–46.1) |
| Q9. The term ‘AF associated to rheumatic mitral valve disease’ includes | ||||
| Both of them, n (%) | 185 (67.8) | (61.9–73.3) | 151 (62.9) | (56.5–69.0) |
| Q10. In the presence of with mitral valve regurgitation, may AF than be defined as valvular? | ||||
| Yes, n (%) | 77 (28.2) | (22.9–33.9) | 57 (23.8) | (18.5–29.6) |
| (c) The presence/absence of prosthetic heart valve | ||||
| Q11. In the presence of a biological aortic valve prosthesis, how may AF then be defined? | ||||
| NVAF, n (%) | 73 (26.7) | (21.6–32.4) | 77 (32.1) | (26.2–38.4) |
| (d) Haemodynamic relevance (severe/moderate/mild stenosis or insufficiency) | ||||
| Q12. Is the degree of valvular stenosis or regurgitation relevant for the definition of valvular AF? | ||||
| No, n (%) | 98 (35.9) | (30.2–41.9) | 69 (28.8) | (23.1–34.9) |
| Q13. Is the degree of valvular regurgitation relevant for the definition of valvular AF? | ||||
| Yes, n (%) | 89 (32.6) | (27.1–38.5) | 63 (26.2) | (20.8–32.3) |
| Q14. Is the degree of valvular stenosis the only relevant parameter for the definition of valvular AF? | ||||
| No, n (%) | 150 (54.9) | (48.8–60.9) | 116 (48.3) | (41.9–54.9) |
| Q15. In case of AF and mitral stenosis, is the degree of stenosis relevant for the definition of valvular AF? | ||||
| No, n (%) | 118 (43.2) | (37.3–49.3) | 92 (38.3) | (32.2–44.8) |
| (e) Miscellaneous | ||||
| Q16. Should AF during hyperthyroidism or post-surgery AF be considered as NVAF? | ||||
| Yes, n (%) | 144 (52.7) | (46.6–58.8) | 121 (50.4) | (43.9–56.9) |
| Q17. Is the degree of left atrium enlargement important to define the origin of AF? | ||||
| No, n (%) | 85 (31.1) | (17.5–27.8) | 78 (32.5) | (21.2–32.7) |
| Clustering topics/questions | Cardiologists (n = 273) | Internists (n = 240) | ||
|---|---|---|---|---|
| n (%) | 95% CI | n (%) | 95% CI | |
| (a) The presence/absence of a known rheumatic aetiology as origin of valvular disease | ||||
| Q3. Are the terms NVAF and non-rheumatic AF synonyms? | ||||
| No, n (%) | 163 (59.7) | (53.6–65.6) | 138 (57.5) | (51.0–63.8) |
| Q4. Are medical history of rheumatic disease and clinical signs of valvular involvement both prerequisites to define AF as rheumatic? | ||||
| Yes, n (%) | 133 (48.7) | (42.6–54.8) | 113 (47.1) | (40.6–53.6) |
| Q5. In the absence of clinical history of rheumatic disease and in the presence of a documented valvular anomaly, may AF then be defined as valvular? | ||||
| Yes, n (%) | 156 (57.1) | (51.0–63.1) | 122 (50.8) | (44.3–57.3) |
| Q6. In a patient with mitral valve disease of unclear origin, may AF then be defined as valvular? | ||||
| No, n (%) | 65 (23.8) | (18.9–29.3) | 67 (27.9) | (22.3–34.1) |
| (b) Site (mitral, aortic) and type of valve involvement (stenosis, insufficiency, both) | ||||
| Q7. In the presence of VHD other than mitral, may AF then be defined as valvular? | ||||
| Yes, n (%) | 110 (40.3) | (34.4–46.4) | 70 (29.2) | (23.5–35.4) |
| Q8. In a patient with rheumatic VHD, may AF then be classified as valvular if associated with mitral involvement or aortic involvement or both? | ||||
| Aortic and mitral involvement, n (%) | 129 (47.3) | (41.2–53.4) | 95 (39.6) | (33.4–46.1) |
| Q9. The term ‘AF associated to rheumatic mitral valve disease’ includes | ||||
| Both of them, n (%) | 185 (67.8) | (61.9–73.3) | 151 (62.9) | (56.5–69.0) |
| Q10. In the presence of with mitral valve regurgitation, may AF than be defined as valvular? | ||||
| Yes, n (%) | 77 (28.2) | (22.9–33.9) | 57 (23.8) | (18.5–29.6) |
| (c) The presence/absence of prosthetic heart valve | ||||
| Q11. In the presence of a biological aortic valve prosthesis, how may AF then be defined? | ||||
| NVAF, n (%) | 73 (26.7) | (21.6–32.4) | 77 (32.1) | (26.2–38.4) |
| (d) Haemodynamic relevance (severe/moderate/mild stenosis or insufficiency) | ||||
| Q12. Is the degree of valvular stenosis or regurgitation relevant for the definition of valvular AF? | ||||
| No, n (%) | 98 (35.9) | (30.2–41.9) | 69 (28.8) | (23.1–34.9) |
| Q13. Is the degree of valvular regurgitation relevant for the definition of valvular AF? | ||||
| Yes, n (%) | 89 (32.6) | (27.1–38.5) | 63 (26.2) | (20.8–32.3) |
| Q14. Is the degree of valvular stenosis the only relevant parameter for the definition of valvular AF? | ||||
| No, n (%) | 150 (54.9) | (48.8–60.9) | 116 (48.3) | (41.9–54.9) |
| Q15. In case of AF and mitral stenosis, is the degree of stenosis relevant for the definition of valvular AF? | ||||
| No, n (%) | 118 (43.2) | (37.3–49.3) | 92 (38.3) | (32.2–44.8) |
| (e) Miscellaneous | ||||
| Q16. Should AF during hyperthyroidism or post-surgery AF be considered as NVAF? | ||||
| Yes, n (%) | 144 (52.7) | (46.6–58.8) | 121 (50.4) | (43.9–56.9) |
| Q17. Is the degree of left atrium enlargement important to define the origin of AF? | ||||
| No, n (%) | 85 (31.1) | (17.5–27.8) | 78 (32.5) | (21.2–32.7) |
In the table, the number of subjects, the percentage, and corresponding 95% confidence interval (95% CI) are reported of the dominant answer to the questions.
Less than half of the physicians considered that history of rheumatic disease and signs of valvular involvement were essential prerequisites to define AF as rheumatic (Q4).
Nearly one-third of respondents considered the lone involvement of aortic valve as qualifying for valvular AF (Q7) though, when the same question was slightly modified, all of the responding physicians did not consider lone aortic valve disease a sufficient prerequisite for valvular AF (Q8). The majority of the physicians agreed that rheumatic mitral valve disease includes also regurgitation (Q9), but only one-third of them defined AF as valvular when associated with mitral regurgitation (Q10).
Nearly one half of the respondents were not able to define AF when associated with an aortic biological valve prosthesis and no more than 30% answered a NVAF (Q11).
Physicians think that the degree of haemodynamic compromise of valve abnormalities associated with AF is not relevant to define valvular AF (Q12–Q15).
Half of the respondents classify AF due to reversible causes as NVAF (Q16) and only one-fifth considered the degree of left atrial enlargement important to define the presence of valvular AF (Q17).
Discussion
The rate of stroke in NVAF ranges from less than 2 to more than 10 strokes per 100 patient-years15 and it is as high as 17–18% in patients with AF of valvular origin.16 Valvular heart diseases frequently coexist with AF and a recent survey found valvular abnormalities, including mild types, in 63.5% of subjects.17
The aim of this survey was to better understand physicians' perception of the definition of valvular and non-valvular AF and to assess whether the meaning of the term ‘AF of valvular origin’ is clear to physicians who use to manage AF. Although most of the surveyed physicians considered that existing definitions of valvular and non-valvular AF were clear, the heterogeneity of the answers queried this initial perception and highlighted some items, around which there are still many doubts.
The presence of a known rheumatic disease defines the valvular origin of AF, according to all main international guidelines. However, less than half of the surveyed physicians considered that rheumatic disease and signs of valvular involvement were both essential prerequisites for defining AF as rheumatic.
The involvement of mitral valve is another key point to define AF as valvular and we observed an important degree of uncertainty also around this issue. One-third of respondents considered lone aortic valve disease as sufficient for the definition of valvular AF but, in the presence of a known rheumatic disease, none of the responding physicians considered lone aortic valve disease a sufficient prerequisite for valvular AF. Furthermore, although most physicians agreed that rheumatic mitral valve disease includes also mitral regurgitation, only one-third of them assumed that mitral regurgitation could qualify for valvular AF. This could be interpreted as if physicians do not assume that mitral failure associated with AF is sufficient by itself to diagnose valvular AF.
The other item around which we found much heterogeneity was the degree of valve disease: there was a low perception that the degree of valve diseases could define valvular AF.
Considering the questionnaire as a whole, the lack of homogeneity in the answers could be interpreted as evidence of a gap in the current conceptual and working definitions of valvular/non-valvular AF, at least as perceived by physicians in clinical practice. However, the definition of the origin of AF directly influences the choice of the proper anti-thrombotic regimen for SPAF.
The most recent trials, comparing warfarin to NOACs in SPAF, enroled only patients with NVAF. In an unpublished post hoc analysis of the ARISTOTLE trial,18 26.4% of the entire trial population (e.g. 4808 patients) had concomitant VHD and some of these patients had more than one valvular abnormality. Efficacy and safety of apixaban in these subjects were no different from that observed in the overall study population, and its favourable profile compared with warfarin was preserved. In the ROCKET-AF trial, 14.1% of the enroled population had a concomitant VHD; no difference was observed, in terms of efficacy and safety of rivaroxaban, between patients with VHD and patients with no valvular abnormality.19 These data are interesting but they cannot represent the evidence that the NOACs can be used also in patients with valvular AF. This highlights the importance of a reliable definition of valvular/non-valvular AF, not only to be applied in clinical practice, but in clinical trials as well. On the basis of these definitions, prospective studies should be undertaken to evaluate the efficacy of NOACs in patients with AF of valvular origin.
Limitations
Our study has some limitations. First, the way questions were formulated may have influenced answers. However, this is true for any kind of questionnaire. For example, quoting Question 2: ‘Do you think that the existing definition of non-valvular …’. Indeed there is no unique existing definition. We have different guidelines addressing this topic and there are some differences which make them somewhat confounding. Furthermore, Question 3: ‘Are the terms non-valvular AF and non-rheumatic AF synonyms?’. We are absolutely aware that the term ‘non-rheumatic’ is unclear and rarely used, but we find patients with rheumatic VHD and AF in clinical practice and dilemmas raise about defining this form of AF. Actually, an excessive uncertainty due to the way questions were formulated could be interpreted as further evidence of the lack of clear conceptual definitions.
Secondly, even though 22% seems to be an acceptable return rate for this kind of surveys, it is a low response rate. We think that the low rate of response is strictly related to some kind of embarrassment that cardiologists and internists, who everyday deal with AF, had facing our survey and its topics.
Although we tried to identify physicians mainly involved in the management of AF (e.g. sending the questionnaire to cardiologists and internists that had participated to CME-related courses), this sampling is not necessarily representative of all Italian cardiologists and internists.
Finally, clinical practice in our country may widely differ with other nations, limiting applicability of these results.
Conclusion
In conclusion, this survey shows an important lack of homogeneity and uncertainties in the answers given by cardiologists and internists who manage SPAF. This evidence highlights a gap in the current conceptual and working definitions of valvular/non-valvular AF. Widely accepted and shared definitions of valvular and non-valvular AF are needed to improve clinical practice and research.
Supplementary material
Supplementary material is available at Europace online.
Conflicts of interest: All the authors received an unrestricted medical grant from Pfizer/Bristol-Myers Squibb (total amount 7000.00 €) for data enter, statistical analysis, and editing of the paper.
Funding
This work was supported by Pfizer/Bristol-Myers Squibb with an unrestricted medical grant.

{kind=link}