





Abstract
Little is known about the optimal number of antitachycardia pacing (ATP) attempts to programme in the fast ventricular tachycardia (FVT) zone. We sought to analyse the long-term efficacy and safety of programming a high number of ATP attempts for FVTs.
All patients receiving an implantable cardioverter/defibrillator (ICD) for coronary artery disease or dilated cardiomyopathy for primary and secondary prevention between 2000 and 2009 were prospectively included. Implantable cardioverter/defibrillators were programmed to deliver 10 ATP attempts for FVT cycle lengths (CLs) of 250–300 ms (200–240 b.p.m.) before shock delivery (5 bursts, then 5 ramps; 8–10 extrastimuli at 81–88% FVT CL; minimal pacing CL 180 ms). Among 770 patients included and followed for 40.6 ± 25.6 months, 137 (17.8%) experienced a total of 1839 FVTs, 1713 of which were ATP-terminated (unadjusted efficacy = 93.1%, adjusted = 81.7%), 106 ATP-accelerated (5.8%), and 20 ATP-resistant (1.1%). The majority of FVT episodes were successfully treated by one or two attempts (98.3%). However, patient-based analysis showed that 17 (12.4%), 8 (5.8%), and 5 patients (2.1%) had at least one episode treated by three or more, four or more, and five or more ATP attempts. The benefit of this strategy was reduced after five attempts. The majority of FVT episodes was asymptomatic and diagnosed at device interrogation during follow-up: syncope and pre-syncope occurred in only 0.2 and 0.4% of episodes, respectively.
Programming a high number of ATP attempts (up to five ATP attempts) in the FVT zone is both safe and efficient and could prevent shocks in numerous ICD recipients.
Introduction
Implantable cardioverter/defibrillator (ICD) is a cornerstone therapy used in the primary or secondary prevention of sudden cardiac death.1 The usefulness of antitachycardia pacing (ATP) has been demonstrated in large studies: offering a painless opportunity of terminating ventricular arrhythmias, reducing the occurrence of defibrillation shocks and hospitalizations, improving patients’ quality of life2 and acceptance of the device, and improving battery life.
Programming ATP for fast ventricular tachycardia (FVT) was initially limited for safety concerns until pioneer studies such as PainFREE Rx3 and PainFREE Rx II4 were published. These studies demonstrated both the safety and the efficacy of ATP for FVTs. Further trials confirmed these initial results in patients implanted for primary and secondary prevention for coronary artery disease (CAD) or dilated cardiomyopathy (DCM).5–10 However, in all published trials, the use of ATP was limited to mainly one unique or rarely two ATP attempts before shock delivery. This was explained by both the fact that most of FVTs are interrupted by the first ATP attempt and by concerns of delaying successful therapy in the case of ATP failure. The efficacy and safety of programming more ATP attempts and the optimal number of attempts to programme in the FVT zone remain unknown.
The objective of this study was to analyse if empiric ICD programming with a high number of ATP attempts is both useful and safe in patients with CAD or DCM, implanted for primary or secondary prevention.
Methods
Patient population
Consecutive patients with CAD and primary DCM scheduled for ICD implantation in our institution from January 2000 to June 2009 were included. Patients were selected for ICD implantation for primary or secondary prevention according to the European Society of Cardiology guidelines at the time of implantation.1,11 Each patient provided written informed consent before enrolment.
Device implantation and programming
Market-released single-chamber, dual–chamber, and cardiac resynchronization therapy-defibrillator (CRT-D) devices capable of delivering ATP for FVTs were implanted (from Biotronik, Boston Scientific, Medtronic, St Jude Medical and Sorin Group companies). Devices were programmed to deliver 10 ATP attempts from the right ventricular lead (including for CRT-D recipients) for ventricular arrhythmias up to 240 b.p.m. before high-energy shock delivery (Figure 1). Consequently, FVT cycle lengths (CLs) of 250–300 ms (i.e. 200–240 b.p.m.) were included in this zone and could benefit from ATP therapy.
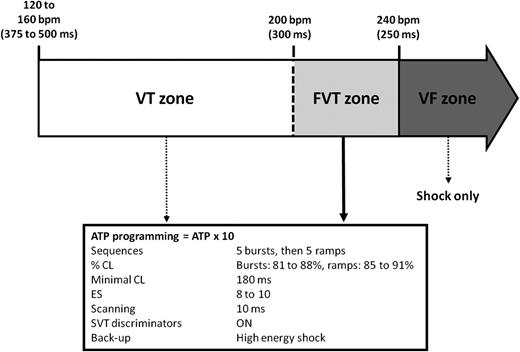
Implantable cardioverter/defibrillator programming parameters. Devices were programmed to deliver 10 ATP attempts for FVT cycle lengths (CL) of 250–300 ms. For CL <250 ms (i.e.>240 b.p.m.), high-energy shocks alone were delivered. Supra-ventricular tachycardia (SVT) discriminators, were programmed up to 240 b.p.m. ATP, antitachycardia pacing; b.p.m. beats per minute; CL, cycle length; ES, extrastimuli; FVT, fast ventricular tachycardia; SVT, supraventricular tachycardia; VF, ventricular fibrillation; VT, ventricular tachycardia.
Antitachycardia pacing consisted of five bursts (8–10 pulse bursts pacing trains at 81–88% of the FVT CL), followed by five ramps (8–10 pulse ramp pacing trains at 85–91% of the FVT CL). The minimal basic CL was programmed at 180 ms. For patients implanted with a market-released ICD able to deliver only bursts or ramps ATP therapies in the same zone (former models from St Jude Medical, St Paul, Minnesota, USA), 10 bursts attempts were programmed. Detection and redetection intervals were programmed to nominal settings. For CL < 250 ms (i.e. >240 b.p.m.), high-energy shocks alone were delivered.
Supra-ventricular tachycardia (SVT) discriminators, defined as stability (40 ms), sudden onset (100 ms or 12–15%), and morphology (when available) algorithms, and AV relationship for dual chambers and CRT-D devices were programmed up to 240 b.p.m.
Data collection and follow-up
Stored far-field electrograms were classified as SVT or FVT by reviewers based on the spontaneous rhythm preceding the onset and following the end of each episode. Only episodes with detailed electrograms were included in the analysis. Acceleration was defined as >10% decrease in tachycardia CL.
Two types of ventricular tachycardia (VT) terminations with ATP have been described: the type-1 and the type-2 breaks. Type-1 breaks are characterized by a termination of VT immediately after the last ATP pulse and are considered as ATP success. Conversely, in the type-2 breaks, the same or a different VT persists for few beats before spontaneous restoration of the underlying rhythm. There is no agreement on the definition of FVT termination for type-2 breaks. Based on the results published by Wathen's group,12 we considered the therapy as successful if FVT lasted <5 beats after the last ATP pulse.
Patients were followed every 6 months as recommended by the French health authorities13 or sooner if clinically indicated. The characteristics of FVT episodes (rate, therapy delivered, and number of ATP attempts necessary for the reduction or the acceleration of FVT) occurring during follow-up were recorded for analysis. Symptoms data were obtained by patients’ interrogation at this time. For patients who died during the follow-up, post-mortem ICD removal and interrogation were performed when possible.
Statistical analysis
Statistical analyses were performed using SPSS for Windows release 16.0 (SPSS Inc., Chicago, IL, USA). Continuous variables with normal distributions were expressed as mean ± SD. Categorical variables were expressed as frequency (percentage). Exact confidence intervals were estimated using binomial distribution. Comparison of categorical measures was performed using the χ2 tests. Survival curves were performed using Kaplan–Meier analysis with log-rank test. To adjust for multiple episodes per patient, the generalized estimating equations (GEE) method was used. A value of P < 0.05 was considered statistically significant.
Results
Patient characteristics
From January 2000 to June 2009, 807 patients met the inclusion criteria and were enrolled in the study. Twelve months of follow-up could not be obtained in 37 patients (4.6%) implanted in our centre but followed in other institutions. These patients were not included in the analysis. Clinical characteristics of the remaining 770 patients are summarized in Table 1. Most patients were on optimal medical therapy at enrolment with 83.1% on β-blocker and 91.2% on angiotensin-converting enzyme inhibitor or angiotensin receptor blocker therapies. Amiodarone was prescribed in 26.0% of patients and up to one-third of patients were on spironolactone or eplerenone.
Baseline patient demographics
| N | 770 |
|---|---|
| Age (years) | 63.2 ± 11.4 |
| Male | 646 (83.9%) |
| Left ventricular ejection fraction (%) | 30.3 ± 9.1 |
| Cardiomyopathy | |
| CAD | 581 (75.5%) |
| DCM | 189 (24.5%) |
| Device type | |
| Single chamber | 465 (60.4%) |
| Dual chamber | 137 (17.8%) |
| CRT-D | 168 (21.8%) |
| Indication for implant | |
| Primary | 349 (45.3%) |
| Secondary | 421 (54.7%) |
| Medication at enrolment | |
| β-Blocker | 640 (83.1%) |
| Angiotensin-converting enzyme inhibitor | 635 (82.5%) |
| Angiotensin receptor blocker | 67 (8.7%) |
| Amiodarone | 200 (26.0%) |
| Digitalis | 37 (4.8%) |
| Aspirin | 504 (65.5%) |
| Clopidogrel | 182 (23.6%) |
| Vitamin K antagonist | 214 (27.8%) |
| Class I antiarrhythmic drugs | 0 (0%) |
| Class IV antiarrhythmic drugs | 15 (1.9%) |
| Dihydropyridine calcium channel blockers | 43 (5.6%) |
| Spironolactone/eplerenone | 242 (31.4%) |
| Diuretics | 521 (67.7%) |
| Statin | 535 (69.5%) |
| Omega-3 acids | 13 (1.7%) |
| Ivabradine | 6 (0.8%) |
| Follow-up (months) | 40.6 ± 28.6 |
| N | 770 |
|---|---|
| Age (years) | 63.2 ± 11.4 |
| Male | 646 (83.9%) |
| Left ventricular ejection fraction (%) | 30.3 ± 9.1 |
| Cardiomyopathy | |
| CAD | 581 (75.5%) |
| DCM | 189 (24.5%) |
| Device type | |
| Single chamber | 465 (60.4%) |
| Dual chamber | 137 (17.8%) |
| CRT-D | 168 (21.8%) |
| Indication for implant | |
| Primary | 349 (45.3%) |
| Secondary | 421 (54.7%) |
| Medication at enrolment | |
| β-Blocker | 640 (83.1%) |
| Angiotensin-converting enzyme inhibitor | 635 (82.5%) |
| Angiotensin receptor blocker | 67 (8.7%) |
| Amiodarone | 200 (26.0%) |
| Digitalis | 37 (4.8%) |
| Aspirin | 504 (65.5%) |
| Clopidogrel | 182 (23.6%) |
| Vitamin K antagonist | 214 (27.8%) |
| Class I antiarrhythmic drugs | 0 (0%) |
| Class IV antiarrhythmic drugs | 15 (1.9%) |
| Dihydropyridine calcium channel blockers | 43 (5.6%) |
| Spironolactone/eplerenone | 242 (31.4%) |
| Diuretics | 521 (67.7%) |
| Statin | 535 (69.5%) |
| Omega-3 acids | 13 (1.7%) |
| Ivabradine | 6 (0.8%) |
| Follow-up (months) | 40.6 ± 28.6 |
Values are mean ± SD or percentages.
CAD, coronary artery disease; CRT-D, cardiac resynchronization therapy; DCM, dilated cardiomyopathy.
Baseline patient demographics
| N | 770 |
|---|---|
| Age (years) | 63.2 ± 11.4 |
| Male | 646 (83.9%) |
| Left ventricular ejection fraction (%) | 30.3 ± 9.1 |
| Cardiomyopathy | |
| CAD | 581 (75.5%) |
| DCM | 189 (24.5%) |
| Device type | |
| Single chamber | 465 (60.4%) |
| Dual chamber | 137 (17.8%) |
| CRT-D | 168 (21.8%) |
| Indication for implant | |
| Primary | 349 (45.3%) |
| Secondary | 421 (54.7%) |
| Medication at enrolment | |
| β-Blocker | 640 (83.1%) |
| Angiotensin-converting enzyme inhibitor | 635 (82.5%) |
| Angiotensin receptor blocker | 67 (8.7%) |
| Amiodarone | 200 (26.0%) |
| Digitalis | 37 (4.8%) |
| Aspirin | 504 (65.5%) |
| Clopidogrel | 182 (23.6%) |
| Vitamin K antagonist | 214 (27.8%) |
| Class I antiarrhythmic drugs | 0 (0%) |
| Class IV antiarrhythmic drugs | 15 (1.9%) |
| Dihydropyridine calcium channel blockers | 43 (5.6%) |
| Spironolactone/eplerenone | 242 (31.4%) |
| Diuretics | 521 (67.7%) |
| Statin | 535 (69.5%) |
| Omega-3 acids | 13 (1.7%) |
| Ivabradine | 6 (0.8%) |
| Follow-up (months) | 40.6 ± 28.6 |
| N | 770 |
|---|---|
| Age (years) | 63.2 ± 11.4 |
| Male | 646 (83.9%) |
| Left ventricular ejection fraction (%) | 30.3 ± 9.1 |
| Cardiomyopathy | |
| CAD | 581 (75.5%) |
| DCM | 189 (24.5%) |
| Device type | |
| Single chamber | 465 (60.4%) |
| Dual chamber | 137 (17.8%) |
| CRT-D | 168 (21.8%) |
| Indication for implant | |
| Primary | 349 (45.3%) |
| Secondary | 421 (54.7%) |
| Medication at enrolment | |
| β-Blocker | 640 (83.1%) |
| Angiotensin-converting enzyme inhibitor | 635 (82.5%) |
| Angiotensin receptor blocker | 67 (8.7%) |
| Amiodarone | 200 (26.0%) |
| Digitalis | 37 (4.8%) |
| Aspirin | 504 (65.5%) |
| Clopidogrel | 182 (23.6%) |
| Vitamin K antagonist | 214 (27.8%) |
| Class I antiarrhythmic drugs | 0 (0%) |
| Class IV antiarrhythmic drugs | 15 (1.9%) |
| Dihydropyridine calcium channel blockers | 43 (5.6%) |
| Spironolactone/eplerenone | 242 (31.4%) |
| Diuretics | 521 (67.7%) |
| Statin | 535 (69.5%) |
| Omega-3 acids | 13 (1.7%) |
| Ivabradine | 6 (0.8%) |
| Follow-up (months) | 40.6 ± 28.6 |
Values are mean ± SD or percentages.
CAD, coronary artery disease; CRT-D, cardiac resynchronization therapy; DCM, dilated cardiomyopathy.
Episodes of fast ventricular tachycardias detected
During a mean follow-up of 40.6 ± 25.6 months (range = 12–125 months), 137 patients (17.8%) experienced a total of 1839 episodes of FVTs (i.e. from 200 and 240 b.p.m.) treated by ATP (1–516 episodes/patient, median = 3 episodes/patient). The mean rate of FVT episodes was 209.2 ± 9.2 b.p.m. (range = 200–240 b.p.m.). The majority of patients (96.4%) experienced from 1–20 episodes, but five patients (3.6%) experienced a total of 1179 episodes (516, 238, 166, 130, and 129 episodes each, respectively) accounting for 64.1% of all the episodes.
Antitachycardia pacing efficacy
Out of the 1839 episodes of FVTs detected, 1713 were successfully terminated by ATP [unadjusted efficacy = 93.1%, GEE-adjusted efficacy = 81.7%; 95% confidence interval (CI), 76.2–86.3%]. The five patients who experienced the majority of episodes had a high ATP efficacy (94.0–100%). Excluding these five patients from the analysis led to a reduction in the unadjusted efficacy to 83.8% with no change in the GEE-adjusted efficacy (81.5%; 95% CI, 75.9–86.1%). Acceleration occurred in 106 episodes (5.8%) in 44 patients and the 10 ATP attempts were unsuccessful in 20 episodes (1.1%) in 10 patients. All unsuccessfully treated or ATP-accelerated FVTs were successfully terminated by back-up programmed high-energy shocks. Antitachycardia pacing efficacy in the different subsets of patients is given in Table 2.
Subgroup analysis of antitachycardia pacing efficacy
| Non-adjusted efficacy (%) | GEE-adjusted efficacy (%) | P | |
|---|---|---|---|
| Sex | 93.6 | 83.4 | 0.075 |
| Male | 74.4 | 66.1 | |
| Female | |||
| Cardiomyopathy | |||
| CAD | 91.3 | 84.3 | 0.371 |
| DCM | 94.3 | 77.9 | |
| LVEF | |||
| ≤30% | 93.5 | 76.5 | 0.093 |
| >30% | 92.7 | 89.0 | |
| β-Blockers | |||
| Yes | 93.8 | 83.6 | 0.230 |
| No | 89.2 | 75.3 | |
| Amiodarone | |||
| Yes | 85.1 | 77.6 | 0.376 |
| No | 94.0 | 83.1 | |
| Indication of implantation | |||
| Primary | 84.7 | 78.3 | 0.449 |
| Secondary | 93.9 | 82.9 |
| Non-adjusted efficacy (%) | GEE-adjusted efficacy (%) | P | |
|---|---|---|---|
| Sex | 93.6 | 83.4 | 0.075 |
| Male | 74.4 | 66.1 | |
| Female | |||
| Cardiomyopathy | |||
| CAD | 91.3 | 84.3 | 0.371 |
| DCM | 94.3 | 77.9 | |
| LVEF | |||
| ≤30% | 93.5 | 76.5 | 0.093 |
| >30% | 92.7 | 89.0 | |
| β-Blockers | |||
| Yes | 93.8 | 83.6 | 0.230 |
| No | 89.2 | 75.3 | |
| Amiodarone | |||
| Yes | 85.1 | 77.6 | 0.376 |
| No | 94.0 | 83.1 | |
| Indication of implantation | |||
| Primary | 84.7 | 78.3 | 0.449 |
| Secondary | 93.9 | 82.9 |
CAD, coronary artery disease; CRT-D, cardiac resynchronization therapy; DCM, dilated cardiomyopathy; LVEF, left ventricular ejection fraction.
Subgroup analysis of antitachycardia pacing efficacy
| Non-adjusted efficacy (%) | GEE-adjusted efficacy (%) | P | |
|---|---|---|---|
| Sex | 93.6 | 83.4 | 0.075 |
| Male | 74.4 | 66.1 | |
| Female | |||
| Cardiomyopathy | |||
| CAD | 91.3 | 84.3 | 0.371 |
| DCM | 94.3 | 77.9 | |
| LVEF | |||
| ≤30% | 93.5 | 76.5 | 0.093 |
| >30% | 92.7 | 89.0 | |
| β-Blockers | |||
| Yes | 93.8 | 83.6 | 0.230 |
| No | 89.2 | 75.3 | |
| Amiodarone | |||
| Yes | 85.1 | 77.6 | 0.376 |
| No | 94.0 | 83.1 | |
| Indication of implantation | |||
| Primary | 84.7 | 78.3 | 0.449 |
| Secondary | 93.9 | 82.9 |
| Non-adjusted efficacy (%) | GEE-adjusted efficacy (%) | P | |
|---|---|---|---|
| Sex | 93.6 | 83.4 | 0.075 |
| Male | 74.4 | 66.1 | |
| Female | |||
| Cardiomyopathy | |||
| CAD | 91.3 | 84.3 | 0.371 |
| DCM | 94.3 | 77.9 | |
| LVEF | |||
| ≤30% | 93.5 | 76.5 | 0.093 |
| >30% | 92.7 | 89.0 | |
| β-Blockers | |||
| Yes | 93.8 | 83.6 | 0.230 |
| No | 89.2 | 75.3 | |
| Amiodarone | |||
| Yes | 85.1 | 77.6 | 0.376 |
| No | 94.0 | 83.1 | |
| Indication of implantation | |||
| Primary | 84.7 | 78.3 | 0.449 |
| Secondary | 93.9 | 82.9 |
CAD, coronary artery disease; CRT-D, cardiac resynchronization therapy; DCM, dilated cardiomyopathy; LVEF, left ventricular ejection fraction.
Successfully treated episodes had a slower rate compared with ATP-accelerated episodes (209.1 ± 8.8 vs. 212.3 ± 13.5 b.p.m., P = 0.02). Antitachycardia pacing efficacy was similar for FVT rates ranging from 200 to 230 b.p.m. and significantly lower for FVT rates between 230 and 240 b.p.m. (Figure 2).
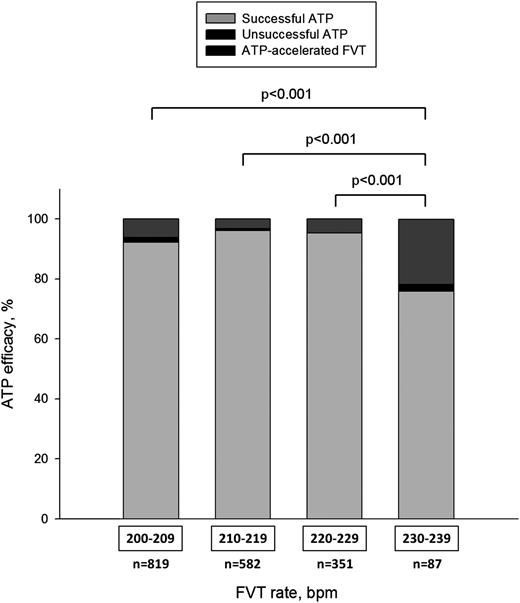
Antitachycardia pacing efficacy according to FVT rate. Antitachycardia pacing efficacy was identical for FVT rates ranging from 200 to 230 b.p.m. and significantly lower for FVT rates between 230 and 240 b.p.m. ATP, antitachycardia pacing; FVT, fast ventricular tachycardia.
Number of antitachycardia pacing attempts required to interrupt fast ventricular tachycardias
The vast majority of ATP-interrupted FVT episodes (1629 out of 1713 FVTs = 95.1%) required one ATP attempt for termination. Only 54 (3.2%) and 30 (1.7%) episodes needed two and from three to nine ATP attempts for termination, respectively (Figure 3). None of the terminated episodes required the delivery of the 10 ATP attempts. The efficacies of the first and second ATP attempts were 88.5 and 40.9%, respectively. The global efficacies of the 3rd to 5th and 6th to 10th attempts were 35.9 and 22.6%, respectively. The average number of ATP attempts required to successfully terminate FVTs was 1.1 ± 0.6 (Figure 3). For the five patients who experienced the majority of FVT episodes (n = 1179), FVTs were successfully interrupted by only one (n = 1173) or two attempts (n = 6).
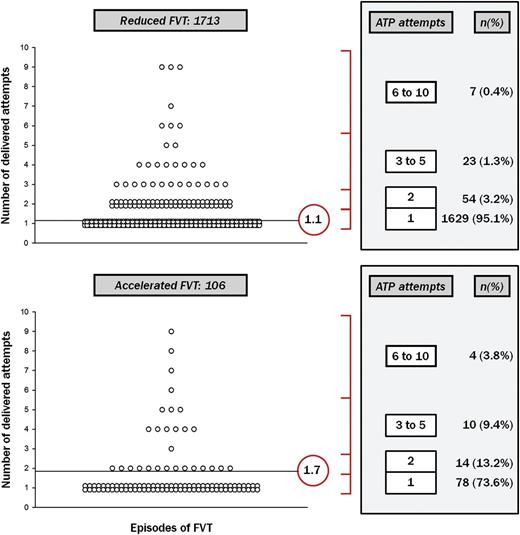
Number of ATP attempts delivered for each FVT episode successfully treated (top) or accelerated (bottom). Each circle represents one FVT episode. The vast majority of FVT episodes were interrupted by the first ATP attempt and few needed two and from three to nine ATP attempts for termination. None of the reduced episodes required the delivery of the 10 ATP attempts. The average number of ATP attempts required to successfully terminate FVTs was 1.1. Fast ventricular tachycardias were mainly accelerated by the first or the second ATP attempt. An average of 1.7 attempts was delivered for accelerated FVT episodes. ATP, antitachycardia pacing; FVT, fast ventricular tachycardia.
Accelerated episodes occurred mainly after the first (67.9%) or the second ATP attempt (18.9%) whereas subsequent ATP attempts (3–10) were less responsible for FVT acceleration (13.2%). An average of 1.7 ± 1.5 ATP attempts were delivered for accelerated FVT episodes (Figure 3).
Although the vast majority of FVT episodes were successfully interrupted by the first or the second ATP attempts, a large number of patients had at least one episode treated by three or more ATP attempts. In a patient-based analysis, 43 (31.4% of patients; 95% CI, 23.7–39.9%), 17 (12.4% of patients; 95% CI, 7.4–19.1%), 8 (5.8% of patients; 95% CI, 2.6–11.2%), and 5 patients (3.6% of patients; 95% CI, 1.2–8.3%) had at least one FVT episode treated by two or more, three or more, four or more, and five or more ATP attempts, respectively. These patients would have received at least one shock with a conventional ICD programming. Thus, during follow-up, 84 shocks were avoided in 43 patients as compared with programming using one ATP attempt for FVTs and 30 shocks were avoided in 17 patients as compared with programming using two ATP attempts, respectively. The benefit of programming numerous ATP attempts was lower above five attempts.
Characteristics of patients with three or more antitachycardia pacing attempts
Seventeen patients (12.4% of FVT patients) had at least one episode treated by three to nine ATP attempts. A comparison of baseline characteristics between patients always treated by 1–2 ATP attempts and those treated at least once by three or more ATP attempts showed no differences in terms of age at implantation (62.8 ± 11.7 vs. 67.4 ± 13.3, P = 0.147), indication for implantation (secondary: 73.3 vs. 88.2%, P = 0.153), heart disease aetiology (CAD, 69.5 vs. 70.5%, P = 0.588), left ventricular ejection fraction (LVEF, 32.1 ± 9.6 vs. 34.5 ± 8.7%, P = 0.335), and mean FVT rates (209.3 ± 9.0 vs. 208.6 ± 10.1 b.p.m., P = 0.390).
Safety of antitachycardia pacing programming
The vast majority of FVT episodes was asymptomatic and diagnosed at device interrogation during routine follow-up. Twelve of the 1839 episodes (0.6%, eight patients) were symptomatic. Four patients experienced lightheadedness or pre-syncope (eight episodes, 0.4%) whereas four other patients experienced syncope (four episodes, 0.2%). All but three symptomatic episodes were treated by only one ATP attempt: two symptomatic episodes were treated by the two ATP attempts whereas the last symptomatic episode was treated by six ATP attempts.
The mortality rate during follow-up was 26.5%, mainly due to non-arrhythmic cardiac deaths (Table 3). The arrhythmic mortality accounted for 11.8% of all the deaths, which were related to electrical storms due to incessant ventricular fibrillation (VF). No death could be reported due to ATP failure since all unsuccessfully paced FVTs were successfully interrupted by shock (see the paragraph on ATP efficacy). Only five patients (2.4%) died from an unknown cause. The mortality assessed by Kaplan–Meier analysis (Figure 4) was similar in patients receiving one or two ATP attempts and those treated at least once by more than two ATP attempts (log-rank P = 0.211).
Causes of death in the study population
| Mortality | 204 (26.5%) |
| Arrhythmic death | 24 (11.8%) |
| Cardiac, non-arrhythmic death | 102 (50.0%) |
| Non cardiac death | 73 (35.8%) |
| Unknown | 5 (2.4%) |
| Mortality | 204 (26.5%) |
| Arrhythmic death | 24 (11.8%) |
| Cardiac, non-arrhythmic death | 102 (50.0%) |
| Non cardiac death | 73 (35.8%) |
| Unknown | 5 (2.4%) |
Causes of death in the study population
| Mortality | 204 (26.5%) |
| Arrhythmic death | 24 (11.8%) |
| Cardiac, non-arrhythmic death | 102 (50.0%) |
| Non cardiac death | 73 (35.8%) |
| Unknown | 5 (2.4%) |
| Mortality | 204 (26.5%) |
| Arrhythmic death | 24 (11.8%) |
| Cardiac, non-arrhythmic death | 102 (50.0%) |
| Non cardiac death | 73 (35.8%) |
| Unknown | 5 (2.4%) |
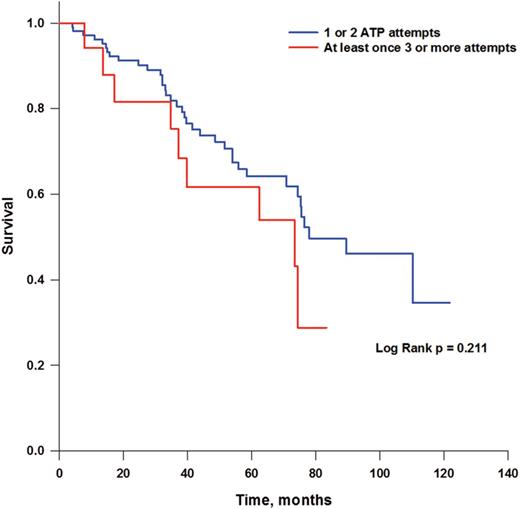
Survival curves in patients treated by only one or two antitachycardia pacing attempts or at least once by three antitachycardia pacing attempts. The mortality assessed by Kaplan–Meier analysis was similar between patients using only one or two antitachycardia pacing attempts and those using at least once three or more attempts (log-rank P= 0211).
Discussion
To our knowledge, this is the first prospective study to demonstrate that empirical programming of a large number of ATP attempts is both safe and effective in terminating FVT episodes in a large unselected population with CAD and DCM implanted for primary and secondary prevention of sudden cardiac death. The adjusted efficacy of ATP was 81.7%, with a very low incidence of pre-syncope or syncope. One interesting finding in this study was that programming more than the usual one or two ATP attempts in the FVT zone avoided the occurrence of 84 shocks in 43 patients (31.4%) and 30 shocks in 17 patients (12.4%), respectively.
Antitachycardia pacing programming for the fast ventricular tachycardia zone
It is well established that ATP has a negligible battery drain, reduces shocks delivery, and improves quality of life and hence acceptance of the device.4,14 Since the publication of the pilots studies PainFREE Rx3 and PainFREE Rx II,4 several trials have analysed the safety and efficacy of ATP for FVTs,5–10 with a maximal unadjusted efficacy up to 89%.7 However, ATP was used carefully in these studies. Only one ATP attempt was used in the FVT zone in PainFREE Rx II,4 PITAGORA ICD,6 AVANCE-D,9 and ADVANCE CRT-D10 trials. Two attempts were used in PainFREE Rx,3 PROVE,8 Jimenez-Candil et al.,7 and Grimm et al.5 studies. This attitude was related to concerns regarding (i) the haemodynamic tolerance of FVT episodes and (ii) the risk of delaying the lifesaving shock in the case of ATP failure. These concerns led to incorporate in recent ICDs the capability to deliver ATP before or during charging in order to prevent shock delay.15,16 However, this new feature allows the delivery of only one or sometimes two ATP attempts. There are no guidelines about optimal ICD programming, but based on previously reported trials and some authors recommendations,15,17–19 physicians empirically programme up to a maximum of two ATP attempts in the FVT zone or high-energy shock with ATP during capacitor charging.
Thus, the benefits and potential risks of programming many ATP attempts are unknown. Only a retrospective small-size study including 24 patients reported the efficacy of six ATP attempts in a zone ranging from 140 to 220 b.p.m. One to three ATP attempts reduced the majority of FVTs, and very few patients had episodes requiring four or more ATP attempts. However, mean rate was low (168 ± 22 b.p.m.) and these results cannot be extrapolated to FVTs.20
How many attempts to programme?
In this study, the majority of episodes were interrupted by the first or the second ATP attempt. Since only 1.8% of episodes were interrupted by 3–9 attempts, one can argue that programming more than two ATP attempts is not necessary. This is true in an episode-based analysis, but not in a patient-based analysis. Indeed, a high proportion of patients had at least one episode treated by three or more ATP attempts, and would have experienced painful shocks even with modern ICD programming. In comparison with PainFREE Rx,3 Jimenez-Candil et al.,7 and PROVE8 trials which programmed two ATP attempts, our programming parameters avoided 30 shocks in 17 patients (12.4%) during overall follow-up (Figure 5). The benefit of this strategy appeared to be less in the case of more than five attempts.
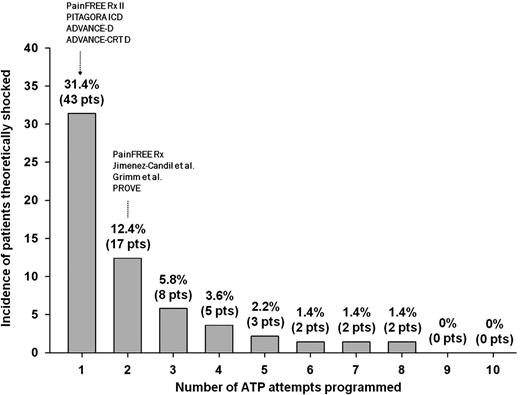
Number of patients in the study who would have experienced at least one shock for ATP failure during the follow-up, according to the number of ATP attempts programmed. Seventeen patients had at least one episode treated by three ATP attempts or more. Then, these patients would have been shocked if only two ATP attempts were programmed (PainFREE Rx, Jimenez-Candil et al., Grimm et al., and PROVE trials-like programming). ATP, antitachycardia pacing; pts, patients.
The benefit of programming more than two ATP attempts may be related to (i) pacing at faster CL (since after each failed ATP attempt, pacing CL decreased by 10 ms) which can improve circuit penetration both anterogradely and retrogradely, and FVT termination;14 and (ii) programming a high number of ATP attempts delays back-up high-energy shock in the case of ATP failure; thus, some long-lasting non-sustained FVT episodes may spontaneously terminate before shock delivery.
Safety considerations
In this study, there was a very low incidence of symptoms (0.6%). This incidence is similar to those reported in previously published studies, i.e. 2 and 0.7% in PainFree Rx I3 and II,4 respectively, 1.7 and 1.1% in ADVANCE-D9 and ADVANCE CRT-D10 trials, respectively, or 0.97% in PITAGORA ICD trial.6 Programming a high number of ATP attempts does not seem to increase the risk of symptoms since all, but one, symptomatic episodes were treated by the first or the second ATP attempt. All ATP-resistant or -accelerated episodes were terminated by ICD shock.
The 26.5% mortality rate during the follow-up was similar to other clinical studies.21,22 No deaths were related to the study programming and only five patients (2.4%) died from unknown cause. Although one can argue that these deaths could be related to the large number of ATP attempts programmed, one should keep in mind that this rate is similar to those reported in clinical trials in ICD recipients for secondary23 or primary indications.8
Study limitations
This study is a single-centre evaluation of ATP for FVTs. However, our population is similar, in age, sex, and LVEF, to the other populations of the main studies that evaluated ATP for the treatment of FVTs.3
Another limitation is the lack of control group with the usual one or two ATP attempts programmed.
We also used a variable ATP scheme in the FVT zone: each attempt was composed by 8–10 pulse bursts pacing trains at 81–88% of the FVT CL, or 8–10 pulse ramp pacing trains at 85–91% of the FVT CL. This is related to the enrolment of patients implanted with any market-released ICDs, each having specific ATP parameters. This limitation can be conversely considered as a strong point, as this represents ATP programming in ‘real life’. Furthermore, only a limited number of episodes were treated or accelerated by 6–10 ATP attempts (11 among 1839 episodes, 0.59% of episodes), limiting the bias of using ramp pacing trains from the 6th to the 10th attempt. Furthermore, as described in Figure 1, only two zones were programmed, i.e. one VT zone and one VF zone (FVTs were detected in the VT zone programmed up to 240 b.p.m. and not in a ‘FVT via VF’ zone). Thus, detection and redetection settings were different from those programmed in PainFREE Rx studies.
As reported in the PREPARE study, some FVT episodes could have been non-sustained and self-terminated if not treated by ATP, possibly overestimating the ATP success rate.
The majority of FVT episodes (1179 out of 1839 episodes) occurred in only five patients. This affects the unadjusted efficacy but not the GEE-adjusted efficacy of ATP, as demonstrated by the similar adjusted efficacy (81.5 vs. 81.7%) found in our study when these five patients are not included in the analysis.
In this study, a low incidence of symptomatic FVT episodes was found (0.6%). Symptoms data were obtained by patients’ interrogation during routine ICD follow-up every 6 months. Although patients were systematically asked about syncopal or pre-syncopal episodes, the real incidence of symptomatic FVT episodes is probably underestimated.
Clinical implications
To our knowledge, this is the first large-scale study evaluating the long-term follow-up safety and efficacy of programming a high number of ATP attempts. The main implication of this study is that in CAD or DCM patients implanted with an ICD for primary or secondary prevention, programming more than one or two ATP attempts is both safe and efficient in terminating a large number of life-threatening FVT episodes thus avoiding painful shocks. Since only few patients did benefit from 6 to 10 attempts, programming 10 attempts is probably not necessary. However, programming up to five attempts could be a reasonable compromise between ATP efficacy and therapy safety. One of the main benefits of this strategy is that this easy programming can be used in all market-released ICDs.
This strategy, in addition to lessons learned from the PREPARE study24 (associating increased tachycardia detection rate and increased number of intervals to detect, SVT discriminators, and high-energy first shock) and from computer modelling,25 could reduce shock incidence and ICD-associated co-morbidities.
The impact of programming a high number of ATP attempts in the case of erroneous SVT detection leading to inappropriate therapy is unknown and has not been evaluated in this study. Programming a high number of ATP attempts could probably allow SVT to terminate spontaneously but also SVT detection algorithm to operate in fast rate since SVT discriminators were programmed up to 240 b.p.m.
Conclusion
This study suggests that programming a high number of ATP attempts (up to five ATP attempts) is useful and prevents numerous painful shocks for FVTs in ICD recipients implanted in primary and secondary prevention of sudden cardiac death in CAD and DCM. This strategy is also safe with a very low incidence of rhythm accelerations, pre-syncope, or syncope.
Conflict of interest: None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}