





Abstract
We performed a survey on current practice of ventricular tachycardia (VT) ablation in patients with implantable cardioverter-defibrillators among the European Heart Rhythm Association Research Network. The main indication for the procedure is the occurrence of multiple shocks or electrical storm, while prophylactic ablation is only rarely performed. The epicardial approach is seldom used and mostly only after failure of endocardial ablation. The main ablation strategy is targeting the clinical VT only by substrate mapping and ablation, and by targeting fractionated potentials with utilization of modern electroanatomical mapping systems. Still, a considerable number of centres frequently perform the procedure using conventional mapping catheters only.
Introduction
The use of implantable cardioverter-defibrillators (ICDs) has dramatically improved the management of patients with structural heart disease and life-threatening ventricular arrhythmias. However, despite the significant mortality benefit, recurrent arrhythmia episodes with subsequent device activation have an impact not only on life quality but also on patients' survival.1 Catheter ablation of ventricular tachycardia (VT) effectively reduces tachycardia episodes2 and is recommended for ICD patients with recurrent or incessant VT or VT storm.3 Although recent developments such as electroanatomical mapping and irrigated ablation technology have improved the results of VT ablation,4 the technique remains demanding. The aim of this survey was to gain insight into the current practice of VT ablation in ICD patients.
Results
Responses were received from 40 partners of the European Heart Rhythm Association Research Network. There was a wide geographic distribution with responses from 17 countries (6 centres from Germany, 5 each from Belgium and Spain, 4 each from Denmark and the United Kingdom, 3 from France, 2 each from Austria and the Netherlands, and 1 centre from 9 other countries). The majority of centres had a high degree of expertise: 70% of them perform >250 and 23% perform 100–250 ablations per year. Despite these high numbers of procedures, VT ablation in ICD recipients is infrequent: only 13% of the centres perform >30 such interventions per year, whereas 58% perform 10–30 and 30% perform 0–10 such interventions per year.
The main indication for the procedure is multiple ICD shocks (73%) or electrical storm (85%) (see Figure 1). Prophylactic ablation after ICD implantation aiming at reduction of future device therapies is rarely performed: 85% of the responding centres never follow this strategy. In addition, 58% never perform ablation after a first appropriate shock for VT.
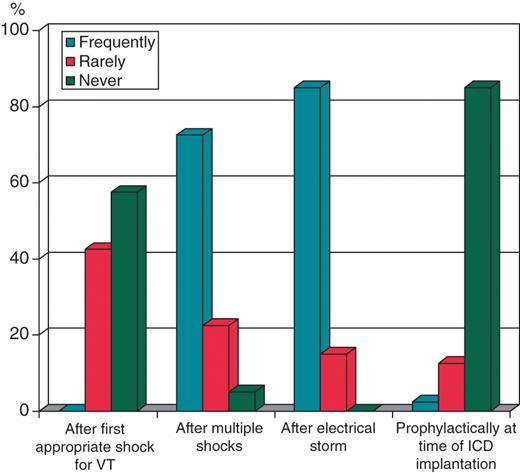
Indications for ablation of ventricular tachycardia in the different centres. Centres were asked to answer whether the listed indications were followed frequently, rarely, or never. ICD, implantable cardioverter-defibrillator; VT, ventricular tachycardia.
General anaesthesia with assisted ventilation is used by 63% of the centres: either routinely (25%) or in unstable patients or if an epicardial approach is chosen (38%). The most frequent approach to the left ventricle is retrogradely through the aortic valve (88%), whereas the transseptal approach is frequently used by only 28%.
The standard approach is endocardial. Fifty-five per cent of the responding centres had performed none and another 30% <5 epicardial VT ablations in the 12 months preceding the survey. In addition, only 21% of the centres apply an initial epicardial approach if an epicardial origin is suspected, whereas 62% use it only after failure of an endocardial approach and 36% reported to never use an epicardial approach.
Modern electroanatomical tools such as the CARTO (Biosense Webster) or NavX (St. Jude Medical) systems are frequently used by 90% of the centres, whereas other modern systems such as non-contact mapping, remote navigation, or contact force evaluation are only used by a minority. However, 25% of the centres reported that they frequently perform the ablation with conventional mapping catheters only.
The most common ablation strategy is substrate mapping and ablation (frequently used by 63%). Substrate ablation is mostly performed by creation of connecting lines, for instance from scar to anatomical boundaries, between scars or within a scar (75% of the centres), and also by targeting late and fractionated potentials around and within scars (70%). Most frequent target of the procedure is ablation of the clinical VT only (63%) and, more rarely, ablation of all inducible VTs (40%).
Discussion
The findings of the survey can be summarized as follows: It has to be noted that, as a voluntary survey, the present analysis does not necessarily reflect in an accurate way clinical practice in the different regions of the Research Network.
The main indication for VT ablation in ICD patients remains the occurrence of multiple shocks or electrical storm, which is in line with current recommendations.3 Although recent studies have shown a usefulness of prophylactic ablation with the aim to reduce subsequent device activation,5,6 the complex character of the procedure obviously limits a wider application.
The epicardial approach is only rarely applied and more than half of the responding centres had performed no epicardial ablation in the 12 months preceding the survey. It is well documented that a portion of VTs can be targeted successfully only from the epicardium. However, this approach is challenging, requires a high degree of expertise, and may be associated with severe complications.7 Thus, it is not surprising that the use of the technique remains limited even among centres with a considerable procedural volume such as the ones that participated in the survey.
The main strategy during the procedure is substrate mapping and ablation by creation of connecting lines and by targeting of fractionated potentials. Electroanatomical mapping systems significantly facilitate VT ablation offering a three-dimensional reconstruction of the ventricle and have expectedly become standard in the majority of the responding centres. However, it is noteworthy that a considerable number of centres still perform VT ablation using only conventional mapping catheters.
Conclusions
The main indication for VT ablation in ICD recipients in centres responding to the survey is the occurrence of multiple shocks or electrical storm. In contrast, prophylactic ablation is only rarely performed. The epicardial approach is seldom used and mostly only after failure of endocardial ablation. Main ablation strategy is targeting of the clinical VT only by substrate mapping and ablation and by targeting of fractionated potentials with utilization of modern electroanatomical mapping systems. However, a considerable number of centres frequently perform the procedure using conventional mapping catheters only.
Conflict of interest: none declared.
Acknowledgements
The production of this EP wire document is under the responsibility of the ‘Scientific Initiatives Committee’ of the European Heart Rhythm Association: C. Blomström-Lundqvist, P. Mabo, N. Dagres, D. Dobreanu, I. van Gelder, M. Grazia Bongiorni, T. Lewalter, G.Y.H. Lip, G. Marinskis, L. Pison, A. Proclemer, J. Hastrup Svendsen.
The previous members of the ‘Scientific Initiatives Committee’: A. Goette, F. Halimi, G. Marinskis, J. Morgan, J.H. Svendsen, L. van Erven, and the EHRA Research Network centres; F. Anselme, F. Atienza, A. Brandes, C.D. Dicandia, K. Etsadashili, A. Grace, A. Lubinski, J. Paisey, who all contributed with the construction of this survey, are acknowledged.
References
Author notes
The survey was conducted by the Scientific Initiatives Committee of the European Heart Rhythm Association.

{kind=link}