





Abstract
We report a case of a patient with long-standing persistent atrial fibrillation (AF) who had rapid formation of spontaneous echo-contrast in the left atrium during pulmonary vein antrum isolation set off by a vagally mediated pause despite standard anticoagulation protocol. Spontaneous echo contrast resolved with ventricular pacing, representing visual evidence for dependence of some AF patients with poor atrial transport function on ventricular emptying with potential greater risk of thromboembolism related to a long ventricular pause.
Case Report
We report a case of a 57-year-old man with long-standing persistent atrial fibrillation (AF) for 12 years who failed three trials of antiarrhythmic drugs including amiodarone as well as multiple cardioversion attempts, presenting for pulmonary vein antrum isolation (PVAI).1 His CHADS-2 score was 1 based on history of hypertension. He had moderate mitral insufficiency by surface echocardiography. His left atrium was dilated at 60 mm in long-axis parasternal view. The patient was chronically anticoagulated with therapeutic weekly international normalized ratio for ≥ 4 weeks prior to PVAI. He was bridged with full-dose enoxaparin and had a trans-oesophageal echo the day of ablation ruling out left atrial thrombus. Once transseptal access to the left atrium was obtained, the patient was anticoagulated with activated clotting time maintained >350 s throughout the case. Ablation took place under general anaesthetic with the patient instrumented with an intracardiac echocardiography probe (ICE, Acunav, Mountain View, California) placed in the right atrium, a decapolar 2 cm circular mapping catheter (Lasso, Biosense Webster, Diamond Bar, California), and an irrigated tip ablation catheter (Celcius Thermocool, Biosense Webster). The patient was in AF at the outset of ablation with mild spontaneous echo contrast in the left atrium (Figure 1A). He experienced an episode of acute vagal stimulation during ablation at the antrum of the left upper pulmonary vein with a 10 s ventricular pause. During the pause (Figure 2), the left atrium immediately filled with very dense spontaneous echo contrast as seen by ICE—‘sludge’ (Figure 1B). As the ventricular rhythm returned, ‘sludge’ dissipated. The patient was then instrumented with a quadripolar catheter placed at the right ventricular apex with programmed stimulation in VVI mode at 60 bpm. During the next radiofrequency application in the same region, atrioventricular conduction slowed down enough for right ventricle apical stimulation to take over. No further ‘sludge’ formation was seen during ventricular pacing (Figure 1C). The patient remained haemodynamically stable and the procedure was ultimately successful with no further clinical recurrences of AF in >1 year. When the patient recovered from anaesthesia, it became apparent that he had suffered a stroke manifesting with expressive aphasia, which resolved over the following 6 months. Post-operative magnetic resonance imaging of the brain confirmed that the event was compatible with multiple small emboli to a small cortical area rather than a single large embolus. The images represent visual evidence for dependence of some AF patients with poor atrial transport function on ventricular emptying with potential greater risk of thromboembolism related to a long ventricular pause. Immediate ventricular pacing is advisable in patients demonstrating vagally mediated pauses during AF ablation, particularly if the patient is actually in AF during the procedure. A movie detailing these observations is available online as supplementary material.

Left atrial imaging using intracardiac echocardiography during Lasso-guided pulmonary vein antrum isolation. (A) Mild spontaneous echo contrast at the beginning of ablation, (B) dense echocontrast—‘sludge’—in the left atrium during a ventricular pause, and (C) microbubbles typically seen during ongoing irrigated ablation of the left atrium while supporting ventricular rhythm with right ventricular apical stimulation.
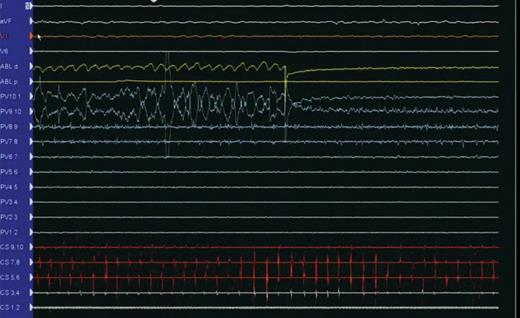
Pause during ablation. Listed from top down are leads I, aVF, V1, and V6 followed by ablation distal and proximal electrograms and Lasso electrograms from proximal to distal (pulmonary vein). Note ablation artefact on Lasso poles 7–8 and 8–9. These are followed by coronary sinus electrograms from proximal to distal.
Supplementary material
Supplementary material is available at Europace online.
Conflict of interest: none declared.

{kind=link}
{kind=link}