





Abstract
A 50-year-old man with a history of renal cell carcinoma was admitted with ventricular tachycardia. Echocardiography showed a mass in the apex of the left ventricle. Cardiac magnetic resonance confirmed a mass infiltrating the anterior–apical wall of the left ventricle. This is the first case describing an association between ventricular tachycardia and renal cell carcinoma metastatic to the left ventricle.
Case report
A 50-year-old man with a past medical history of renal cell carcinoma (RCC), treated with radical nephrectomy and chemotherapy, was admitted to our hospital with symptoms of palpitations and dyspnoea. Electrocardiogram revealed sustained ventricular tachycardia (SVT) with a rate of 260 bpm, QS from V1 to V6 and frontal right axis deviation (Figure 1B). Restoration of normal sinus rhythm was achieved by electrical cardioversion with biphasic DC shocks of 200 J. Transthoracic echocardiography showed a mass in the apex of the left ventricle (LV) without vena caval or right atrial involvement. Coronary angiography did not show significant epicardial coronary stenosis. Cardiac magnetic resonance confirmed a mass of 36×27×48 mm, infiltrating the anterior–apical wall of the LV (Figure 1A). The mass biopsied was consistent with metastatic RCC. A single-chamber implantable cardioverter-defibrillator was implanted and chemotherapy with gemcitabine continued. He was discharged on therapy with amiodarone after 7 days. At 6-month follow-up, the patient was alive and no SVT episodes were detected.
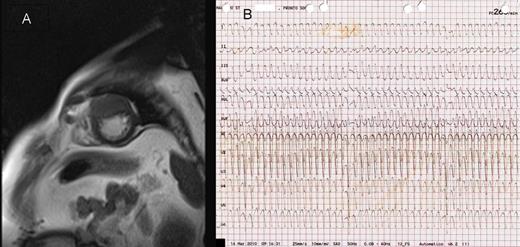
(A) Cardiac magnetic resonance showing a mass infiltrating the anterior−apical wall of the left ventricle. (B) Electrocardiogram showing sustained ventricular tachycardia with a rate of 260 bpm, QS from V1 to V6 and frontal right axis deviation.
Discussion
In our patient, the only documented disease that could be related to SVT was the cardiac metastasis and the morphology of the ventricular tachycardia can be compatible with an origin of the arrhythmia from the apex of the heart.
Malignant tumours affecting the heart are more likely to represent metastatic disease than primary cancer.1 Cardiac metastases from RCC are extremely infrequent but LV involvement is even more Infrequent.2 To the best of our knowledge, this is the first case describing an association between SVT and RCC metastatic to the LV.
In patients with malignant tumours and arrhythmias, the possibility of cardiac metastasis should be considered.
Conflict of interest: none declared.

{kind=link}