





Abstract
Atrial fibrillation (AF) is the most common cardiac arrhythmia, its prevalence increasing markedly with age. Atrial fibrillation is strongly associated with increased risk of morbidity, including stroke and thromboembolism. There is growing awareness of the economic burden of AF due to ageing populations and constrained public finances. A systematic review was performed (1990–2009). Cost studies for AF or atrial flutter were included; acute-onset and post-operative AF were excluded. Total, direct, and indirect costs were extracted. Of 875 records retrieved, 37 studies were included. The cost of managing individual AF patients is high. Direct-cost estimates ranged from $2000 to 14 200 per patient-year in the USA and from €450 to 3000 in Europe. This is comparable with other chronic conditions such as diabetes. The direct cost of AF represented 0.9–2.4% of the UK health-care budget in 2000 and had almost doubled over the previous 5 years. Inpatient care accounted for 50–70% of annual direct costs. In the USA, AF hospitalizations alone cost ∼$6.65 billion in 2005. In this first systematic review of the economic burden of AF, hospitalizations consistently represented the major cost driver. Costs and hospitalizations attributable to AF have increased markedly over recent decades and are expected to increase in future due to ageing populations.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia and is strongly associated with increased risk of morbidity, such as stroke and thromboembolism.1 Atrial fibrillation is considered an epidemic, affecting 1–1.5% of the population in the developed world.2 The risk increases with age,3 and the prevalence is projected to grow at least three-fold by 2050.2 Hospitalization rates for AF have been increasing steadily over the last two decades4 and almost tripled in 2000 compared with the previous two decades.5 In many countries, there is a growing awareness of the economic burden associated with AF due to ageing populations and constrained public finances.
A number of published studies have described the cost of illness associated with AF; these have varied widely in methodologies and the costs that have been included. However, no systematic review has been performed to assemble and interpret the available data. The objective of this study was to provide the first systematic review of this area; to describe the cost of illness associated with AF, including that associated with stroke and bleeding complications; and to identify the main cost drivers. The resources directly involved in providing health care (direct costs) and other costs associated with AF, such as lost work productivity (indirect costs), were also reviewed.
Methods
A systematic review was performed in accordance with a pre-specified protocol. Searches were performed from 1 January 1990 to 21 April 2009. No limitations on publication language or geographic perspective were applied. Studies reporting cost of illness, resource utilization, or length of hospital stay for AF (paroxysmal, persistent, or permanent) or atrial flutter were included. Studies also were included if they focused on specific subgroups of patients within the AF population, on specific interventions, or on treatment settings—with the exception of acute-onset or post-operative AF and cost-effectiveness analyses, which were excluded.
The following electronic databases were searched: MEDLINE, EMBASE, and The Cochrane Library, which included the National Health Service Economic Evaluation, Health Technology Assessment, and Database of Abstracts of Reviews of Effectiveness databases. Search terms included ‘atrial fibrillation [medical subject heading (MeSH)]', atrial flutter (MeSH)', ‘cost of illness (MeSH)', ‘burden of illness', ‘economic burden', ‘resource use', ‘resource utilization', ‘direct cost', ‘indirect cost', and ‘annual cost'. Separate searches were performed for studies reporting costs or resource use associated with stroke or bleeding in AF patients. Conference abstracts from the American Heart Association, European Heart Rhythm Association, European Society of Cardiology, International Society for Pharmacoeconomics and Outcomes Research, and American College of Cardiology were searched for the period from January 2005 to April 2009.
Study inclusion was performed in parallel by two researchers; disagreements were resolved by consensus. The range of direct annual and hospital costs estimates for the USA and Western Europe was summarized. Disaggregated costs within annual direct costs of AF were reviewed to identify the main cost drivers.
Results
Search results and study characteristics
The search strategy identified 875 records. Of these, 37 studies met the study inclusion criteria (Figure 1). Two notable studies, the economic analyses performed alongside the Rate Control Versus Electrical Cardioversion (RACE) study and the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) trial6,7 were excluded because these were cost-effectiveness analyses rather than cost-of-illness studies, and resource use data collected within clinical trials may have been driven by protocol requirements. Table 1 presents the characteristics of the 37 included studies.
Characteristics of cost-of-illness studies for atrial fibrillation, arranged by study type
| Study type and methods | Type of reported cost data | Population type and number | Country | Author, date |
|---|---|---|---|---|
| 6-month multicentre, prospective observational study with 3-month retrospective data collection | Annual direct costs | 361 consecutive AF patients (75% with persistent AF); recruited from general or family practices (67%), internal medicine (26%), or cardiology practices (7%) | Germany | McBride, 20098 |
| Costs included physician visits, diagnostic and interventional procedures, medication, emergency transports, hospitalizations, and rehabilitation | ||||
| Prospective observational study | Cost of admission and annual cost of AF (direct and indirect) | 5333 consecutive patients recruited from outpatient cardiology clinics, cardiology wards, first (heart) aids, and inpatient wards | Europe (35 countries) | Ringborg, 2008 (Euro Heart Survey)9 |
| Costs included diagnostic and interventional procedures, medications, inpatient care, consultations, and work loss | Data reported for Greece, Italy, Netherlands, Poland, and Spain | |||
| Outpatient clinic did not have cost of admission | ||||
| Prospective observational study | Direct and indirect costs over a mean follow-up of 329 days | 671 consecutive AF patients recruited by 82 cardiologists in their general office practice | France | Le Heuzey, 2004 (COCAF)10 |
| Costs included consultation, diagnostic and interventional procedures, medication, hospitalizations, and loss of work | ||||
| Prospective observational study, patient interviews | Direct and indirect costs of warfarin | 402 consecutive new patients with paroxysmal or chronic non-valvular AF referred by the community and outpatient clinics and treated by the physicians in a single-centre anticoagulation clinic | UK | Abdelhafiz and Wheeldon, 200311 |
| Costs included medications, monitoring and bleed-related physician visits, hospitalizations, and interventional procedures | ||||
| Prospective observational study | Costs of inpatient and outpatient cardioversion | 185 consecutive patients with symptomatic AF recruited from a university hospital (inpatient or outpatient setting) | Germany | Gronefeld, 200312 |
| Costs included physician visits, diagnostic and interventional procedures and medications, and hospitalization and treatment for inpatient care | ||||
| Prospective observational study | 30-day direct costs for AF patients presenting to an emergency department, before and after implementation of a new guideline for the management of patients. | 446 consecutive AF patients in an emergency department | USA | Zimetbaum, 200313 |
| Costs included emergency room care, diagnostic interventional procedures, inpatient, and follow-up care, which included outpatient services, visits to primary care physicians and cardiologists, and outpatient diagnostic, and therapeutic procedures | ||||
| Prospective observational study | Comparison of length of stay for stroke in AF and non-AF patients | 4534 consecutive stroke patients (803 with AF) recruited from hospitals | Europe (seven countries) | Lamassa, 200114 |
| Prospective cohort study; costs based on medicare payments plus patient copayments | 1-year medicare costs | 26 753 newly diagnosed, hospitalized patients, 13 558 with AF and 13 195 without AF, with one other cardiovascular diagnosis | USA | Wolf, 199815 |
| Costs included hospitalizations, nursing facilities, home health care, outpatient care, and physician visits | ||||
| Observational study; patient interviews and inpatient register | Direct costs for year before and year after radiofrequency ablation | 26 patients with resistant AF recruited from a hospital | Sweden | Jensen, 199516 |
| Costs included interventional procedures, medication, and hospitalization | ||||
| Prospective, observational study; survey of 18 academic medical centres | Cost of digoxin treatment | 115 patients with AF (85%), AFL (7%), or both (8%), recruited from a university hospital and its emergency department | USA | Roberts, 199317 |
| Costs included interventional procedures, medication, and hospitalization | ||||
| Semistructured interviews with NHS staff | Annual costs of INR monitoring and laboratory procedures | Six monitoring services (secondary-care Trusts) responsible for average of 3459 warfarin patients | UK | Arya, 200518 |
| Survey of 306 cardiologists; 100 responded | Annual cost of AF | 100 private-sector cardiologists | France | Jeantet, 200119 |
| Costs included medications and diagnostic procedures | ||||
| Prospective, randomized multicentre study | Costs of electroanatomically guided and conventional catheter ablation (interventional procedure costs) | 210 patients with AFL (concomitant AF permitted) recruited in hospital | Europe (8 centres) | Hindricks, 200920 |
| Economic evaluation alongside clinical trial | Time and travelling costs in attending anticoagulation clinics | 381 AF patients enrolled in a stroke prevention RCT recruited in an outpatient setting | Worldwide* | Jowett, 2008 (SPORTIF III trial)21 |
| Prospective, randomized pilot study | Compared accelerated emergency-department strategy using LMWH with traditional hospital admission | 18 patients with newly diagnosed AF who presented at an outpatient emergency department-based disease management centre | USA | Kim, 200322 |
| Costs included medication and hospitalization | ||||
| Cross-sectional observational study, patient and physician questionnaires | Annual direct and indirect costs in primary and secondary care | 922 patients with AF (538 in Germany, 384 in Sweden) from primary or specialist care centres (inpatient and outpatient settings) | Europe (two countries) | Ericsson, 200723 |
| Costs included physician visits, interventional procedures, hospitalization, medication, travel costs, home care, and other indirect costs | ||||
| Cross-sectional study; continuous morbidity recording scheme data | Frequency of primary care visits | 3135 patients with AF in a primary care setting | UK (Scotland) | Murphy, 200724 |
| Retrospective database analysis | Incremental inpatient costs for AF patients minus matched controls | 691 897 patients with secondary AF in an inpatient setting | USA | Exuzides, 200825 |
| Costs included hospitalization, interventional procedures, and medication | ||||
| Longitudinal, matched cohort database study; regression analysis | Incremental annual costs of inpatient and outpatient care | 55 260 AF patients recruited in an inpatient and outpatient setting | USA | Lee, 200826 |
| Costs included hospitalization, outpatient visits, physician visits, interventional procedures, medication, and nursing and home care | ||||
| Database analysis, chart review, and patient interviews | 1-year direct and indirect costs of stroke in AF patients | 71 consecutive AF patients with stroke, from a cohort of 558 stroke patients who presented at a hospital in an inpatient or outpatient setting | Germany | Bruggenjurgen, 200727 |
| Costs included hospitalization, outpatient visits, physician visits, interventional procedures, medication, nursing care and rehabilitation, and other indirect costs | ||||
| Database analysis; case-control and regression analyses | National incremental direct cost of hospital care | 348 131 non-valvular AF patients in hospital inpatient, outpatient, or office-visit settings | USA | Coyne, 200628 |
| Costs included inpatient and outpatient physician services, hospitalization, interventional procedures, and medication | ||||
| Retrospective database study in a finnish communal health care setting | Direct costs of warfarin treatment over a 12-month period | 250 warfarin-treated AF patients in a primary care setting | Finland | Hallinen, 200629 |
| Costs included physician visits, diagnostic procedures, hospitalization, and medication | ||||
| Administrative claims database analysis | Annual direct costs for newly diagnosed AF patients | Newly diagnosed patients with AF in primary care: 6846 warfarin-treated, 40 849 untreated | USA | Fidan, 200530 |
| Costs included interventional procedures, medication, and other direct costs | ||||
| Database analysis: medicare | Annual AF-related medical costs for medicare beneficiaries | 59 648 patients aged ≥65 years with AF from hospital inpatient and outpatient settings | USA | Pelletier, 200531 |
| Costs included inpatient and outpatient physician services, hospitalization, diagnostic and interventional procedures, and medication | ||||
| Retrospective analysis of a privately insured database (16 employers in the USA) | Excess annual direct and indirect costs | 3944 AF patients from hospital inpatient and outpatient settings | USA | Wu, 200532 |
| Costs included inpatient and outpatient physician services, hospitalization, diagnostic and interventional procedures, and medication | ||||
| Database analysis: medicare | Length-of-stay and hospital costs for patients with AF or AFL | Medicare beneficiaries: 8454 with AF and 986 with AFL, from hospital or institutional settings | USA | Baine, 200133 |
| Two retrospective electronic medical record and two Delphi-panel studies | Direct cost of INR monitoring | 1721 chronic AF patients from primary care settings | Sweden | Bjorholt, 200734 |
| Retrospective medical record review | Direct cost of hospitalizations for bleeding | 2460 warfarin-treated patients; cost data collected for three AF patients identified from a hospital anticoagulation service | USA | Fanikos, 200535 |
| Costs included emergency care, physician and nursing visits and care, diagnostic and interventional procedures, hospitalization, and medication | ||||
| Retrospective, observational cohort study | Total direct costs before and after AF diagnosis and after a stroke or bleeding event | 3891 newly diagnosed patients with chronic non-valvular AF, identified from hospital inpatient and outpatient settings | USA | Stephenson, 200536 |
| Costs included hospitalization, diagnostic and interventional procedures, and medication | ||||
| Retrospective analysis; direct and indirect costs included | Cost of outpatient cardioversion | 532 consecutive patients with atrial tachyarrhythmia, identified from an outpatient department | USA | Botkin, 200337 |
| Retrospective medical record study combined with patient interviews | Direct costs of radiofrequency ablation and drug treatment | 118 consecutive patients with symptomatic paroxysmal AF, identified in an inpatient setting | France | Weerasooriya, 200338 |
| Costs included hospitalization, consultations, interventional procedures, and medication | ||||
| Retrospective chart review | Direct costs of a first episode of uncomplicated AF | 47 patients with a first episode of uncomplicated AF, in a university hospital (emergency department) setting | USA | Kim, 200139 |
| Costs included hospitalization and interventional procedures | ||||
| Retrospective chart review | Cost of acute treatment in an emergency department | 114 consecutive AF patients identified from hospital emergency departments; first documented episode = 47% | USA | Dell'Orfano, 199940 |
| Cost included hospitalization and interventional procedures | ||||
| Review of hospital bills; indirect costs were defined as overhead and malpractice insurance | Comparison of radiofrequency modification and ablation of the atrioventricular junction | 24 patients with chronic AF treated in a hospital; costs based on subgroup of 16 patients | USA | Knight, 199741 |
| Costs included consultations, diagnostic and interventional procedures, and hospitalization | ||||
| Registry study | Effect of AF on stroke-related direct inpatient costs | 1619 stroke patients also diagnosed with AF | Sweden | Ghatnekar and Glader, 200842 |
| Registry, chart review, patient interviews, and case report forms | Annual direct costs of hospital care and impact of AF recurrence | 973 AF patients | USA | Reynolds, 2007 (FRACTAL)43 |
| Costs included consultations, diagnostic and interventional procedures, ambulatory monitoring, and hospitalization | ||||
| Combination of available prevalence data and resource use or cost estimates | National direct-cost estimates for 1995; projections for 2000 | AF patients | UK | Stewart, 200444 |
| Costs included consultations, diagnostic and interventional procedures, ambulatory monitoring and hospitalization, nursing home care, and medication |
| Study type and methods | Type of reported cost data | Population type and number | Country | Author, date |
|---|---|---|---|---|
| 6-month multicentre, prospective observational study with 3-month retrospective data collection | Annual direct costs | 361 consecutive AF patients (75% with persistent AF); recruited from general or family practices (67%), internal medicine (26%), or cardiology practices (7%) | Germany | McBride, 20098 |
| Costs included physician visits, diagnostic and interventional procedures, medication, emergency transports, hospitalizations, and rehabilitation | ||||
| Prospective observational study | Cost of admission and annual cost of AF (direct and indirect) | 5333 consecutive patients recruited from outpatient cardiology clinics, cardiology wards, first (heart) aids, and inpatient wards | Europe (35 countries) | Ringborg, 2008 (Euro Heart Survey)9 |
| Costs included diagnostic and interventional procedures, medications, inpatient care, consultations, and work loss | Data reported for Greece, Italy, Netherlands, Poland, and Spain | |||
| Outpatient clinic did not have cost of admission | ||||
| Prospective observational study | Direct and indirect costs over a mean follow-up of 329 days | 671 consecutive AF patients recruited by 82 cardiologists in their general office practice | France | Le Heuzey, 2004 (COCAF)10 |
| Costs included consultation, diagnostic and interventional procedures, medication, hospitalizations, and loss of work | ||||
| Prospective observational study, patient interviews | Direct and indirect costs of warfarin | 402 consecutive new patients with paroxysmal or chronic non-valvular AF referred by the community and outpatient clinics and treated by the physicians in a single-centre anticoagulation clinic | UK | Abdelhafiz and Wheeldon, 200311 |
| Costs included medications, monitoring and bleed-related physician visits, hospitalizations, and interventional procedures | ||||
| Prospective observational study | Costs of inpatient and outpatient cardioversion | 185 consecutive patients with symptomatic AF recruited from a university hospital (inpatient or outpatient setting) | Germany | Gronefeld, 200312 |
| Costs included physician visits, diagnostic and interventional procedures and medications, and hospitalization and treatment for inpatient care | ||||
| Prospective observational study | 30-day direct costs for AF patients presenting to an emergency department, before and after implementation of a new guideline for the management of patients. | 446 consecutive AF patients in an emergency department | USA | Zimetbaum, 200313 |
| Costs included emergency room care, diagnostic interventional procedures, inpatient, and follow-up care, which included outpatient services, visits to primary care physicians and cardiologists, and outpatient diagnostic, and therapeutic procedures | ||||
| Prospective observational study | Comparison of length of stay for stroke in AF and non-AF patients | 4534 consecutive stroke patients (803 with AF) recruited from hospitals | Europe (seven countries) | Lamassa, 200114 |
| Prospective cohort study; costs based on medicare payments plus patient copayments | 1-year medicare costs | 26 753 newly diagnosed, hospitalized patients, 13 558 with AF and 13 195 without AF, with one other cardiovascular diagnosis | USA | Wolf, 199815 |
| Costs included hospitalizations, nursing facilities, home health care, outpatient care, and physician visits | ||||
| Observational study; patient interviews and inpatient register | Direct costs for year before and year after radiofrequency ablation | 26 patients with resistant AF recruited from a hospital | Sweden | Jensen, 199516 |
| Costs included interventional procedures, medication, and hospitalization | ||||
| Prospective, observational study; survey of 18 academic medical centres | Cost of digoxin treatment | 115 patients with AF (85%), AFL (7%), or both (8%), recruited from a university hospital and its emergency department | USA | Roberts, 199317 |
| Costs included interventional procedures, medication, and hospitalization | ||||
| Semistructured interviews with NHS staff | Annual costs of INR monitoring and laboratory procedures | Six monitoring services (secondary-care Trusts) responsible for average of 3459 warfarin patients | UK | Arya, 200518 |
| Survey of 306 cardiologists; 100 responded | Annual cost of AF | 100 private-sector cardiologists | France | Jeantet, 200119 |
| Costs included medications and diagnostic procedures | ||||
| Prospective, randomized multicentre study | Costs of electroanatomically guided and conventional catheter ablation (interventional procedure costs) | 210 patients with AFL (concomitant AF permitted) recruited in hospital | Europe (8 centres) | Hindricks, 200920 |
| Economic evaluation alongside clinical trial | Time and travelling costs in attending anticoagulation clinics | 381 AF patients enrolled in a stroke prevention RCT recruited in an outpatient setting | Worldwide* | Jowett, 2008 (SPORTIF III trial)21 |
| Prospective, randomized pilot study | Compared accelerated emergency-department strategy using LMWH with traditional hospital admission | 18 patients with newly diagnosed AF who presented at an outpatient emergency department-based disease management centre | USA | Kim, 200322 |
| Costs included medication and hospitalization | ||||
| Cross-sectional observational study, patient and physician questionnaires | Annual direct and indirect costs in primary and secondary care | 922 patients with AF (538 in Germany, 384 in Sweden) from primary or specialist care centres (inpatient and outpatient settings) | Europe (two countries) | Ericsson, 200723 |
| Costs included physician visits, interventional procedures, hospitalization, medication, travel costs, home care, and other indirect costs | ||||
| Cross-sectional study; continuous morbidity recording scheme data | Frequency of primary care visits | 3135 patients with AF in a primary care setting | UK (Scotland) | Murphy, 200724 |
| Retrospective database analysis | Incremental inpatient costs for AF patients minus matched controls | 691 897 patients with secondary AF in an inpatient setting | USA | Exuzides, 200825 |
| Costs included hospitalization, interventional procedures, and medication | ||||
| Longitudinal, matched cohort database study; regression analysis | Incremental annual costs of inpatient and outpatient care | 55 260 AF patients recruited in an inpatient and outpatient setting | USA | Lee, 200826 |
| Costs included hospitalization, outpatient visits, physician visits, interventional procedures, medication, and nursing and home care | ||||
| Database analysis, chart review, and patient interviews | 1-year direct and indirect costs of stroke in AF patients | 71 consecutive AF patients with stroke, from a cohort of 558 stroke patients who presented at a hospital in an inpatient or outpatient setting | Germany | Bruggenjurgen, 200727 |
| Costs included hospitalization, outpatient visits, physician visits, interventional procedures, medication, nursing care and rehabilitation, and other indirect costs | ||||
| Database analysis; case-control and regression analyses | National incremental direct cost of hospital care | 348 131 non-valvular AF patients in hospital inpatient, outpatient, or office-visit settings | USA | Coyne, 200628 |
| Costs included inpatient and outpatient physician services, hospitalization, interventional procedures, and medication | ||||
| Retrospective database study in a finnish communal health care setting | Direct costs of warfarin treatment over a 12-month period | 250 warfarin-treated AF patients in a primary care setting | Finland | Hallinen, 200629 |
| Costs included physician visits, diagnostic procedures, hospitalization, and medication | ||||
| Administrative claims database analysis | Annual direct costs for newly diagnosed AF patients | Newly diagnosed patients with AF in primary care: 6846 warfarin-treated, 40 849 untreated | USA | Fidan, 200530 |
| Costs included interventional procedures, medication, and other direct costs | ||||
| Database analysis: medicare | Annual AF-related medical costs for medicare beneficiaries | 59 648 patients aged ≥65 years with AF from hospital inpatient and outpatient settings | USA | Pelletier, 200531 |
| Costs included inpatient and outpatient physician services, hospitalization, diagnostic and interventional procedures, and medication | ||||
| Retrospective analysis of a privately insured database (16 employers in the USA) | Excess annual direct and indirect costs | 3944 AF patients from hospital inpatient and outpatient settings | USA | Wu, 200532 |
| Costs included inpatient and outpatient physician services, hospitalization, diagnostic and interventional procedures, and medication | ||||
| Database analysis: medicare | Length-of-stay and hospital costs for patients with AF or AFL | Medicare beneficiaries: 8454 with AF and 986 with AFL, from hospital or institutional settings | USA | Baine, 200133 |
| Two retrospective electronic medical record and two Delphi-panel studies | Direct cost of INR monitoring | 1721 chronic AF patients from primary care settings | Sweden | Bjorholt, 200734 |
| Retrospective medical record review | Direct cost of hospitalizations for bleeding | 2460 warfarin-treated patients; cost data collected for three AF patients identified from a hospital anticoagulation service | USA | Fanikos, 200535 |
| Costs included emergency care, physician and nursing visits and care, diagnostic and interventional procedures, hospitalization, and medication | ||||
| Retrospective, observational cohort study | Total direct costs before and after AF diagnosis and after a stroke or bleeding event | 3891 newly diagnosed patients with chronic non-valvular AF, identified from hospital inpatient and outpatient settings | USA | Stephenson, 200536 |
| Costs included hospitalization, diagnostic and interventional procedures, and medication | ||||
| Retrospective analysis; direct and indirect costs included | Cost of outpatient cardioversion | 532 consecutive patients with atrial tachyarrhythmia, identified from an outpatient department | USA | Botkin, 200337 |
| Retrospective medical record study combined with patient interviews | Direct costs of radiofrequency ablation and drug treatment | 118 consecutive patients with symptomatic paroxysmal AF, identified in an inpatient setting | France | Weerasooriya, 200338 |
| Costs included hospitalization, consultations, interventional procedures, and medication | ||||
| Retrospective chart review | Direct costs of a first episode of uncomplicated AF | 47 patients with a first episode of uncomplicated AF, in a university hospital (emergency department) setting | USA | Kim, 200139 |
| Costs included hospitalization and interventional procedures | ||||
| Retrospective chart review | Cost of acute treatment in an emergency department | 114 consecutive AF patients identified from hospital emergency departments; first documented episode = 47% | USA | Dell'Orfano, 199940 |
| Cost included hospitalization and interventional procedures | ||||
| Review of hospital bills; indirect costs were defined as overhead and malpractice insurance | Comparison of radiofrequency modification and ablation of the atrioventricular junction | 24 patients with chronic AF treated in a hospital; costs based on subgroup of 16 patients | USA | Knight, 199741 |
| Costs included consultations, diagnostic and interventional procedures, and hospitalization | ||||
| Registry study | Effect of AF on stroke-related direct inpatient costs | 1619 stroke patients also diagnosed with AF | Sweden | Ghatnekar and Glader, 200842 |
| Registry, chart review, patient interviews, and case report forms | Annual direct costs of hospital care and impact of AF recurrence | 973 AF patients | USA | Reynolds, 2007 (FRACTAL)43 |
| Costs included consultations, diagnostic and interventional procedures, ambulatory monitoring, and hospitalization | ||||
| Combination of available prevalence data and resource use or cost estimates | National direct-cost estimates for 1995; projections for 2000 | AF patients | UK | Stewart, 200444 |
| Costs included consultations, diagnostic and interventional procedures, ambulatory monitoring and hospitalization, nursing home care, and medication |
AF, atrial fibrillation; AFL, atrial flutter; COCAF, Cost of Care in Atrial Fibrillation trial; FRACTAL, fibrillation registry assessing costs, Therapies, Adverse Events and Lifestyle registry; INR, international normalized ratio; LMWH, low molecular-weight heparin; NHS, National Health Service (UK); RCT, randomized controlled trial; SPORTIF III, stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation trial; UK, United Kingdom; USA, United States of America.
*Australia, France, Portugal, Spain, Sweden, and the United Kingdom.
Characteristics of cost-of-illness studies for atrial fibrillation, arranged by study type
| Study type and methods | Type of reported cost data | Population type and number | Country | Author, date |
|---|---|---|---|---|
| 6-month multicentre, prospective observational study with 3-month retrospective data collection | Annual direct costs | 361 consecutive AF patients (75% with persistent AF); recruited from general or family practices (67%), internal medicine (26%), or cardiology practices (7%) | Germany | McBride, 20098 |
| Costs included physician visits, diagnostic and interventional procedures, medication, emergency transports, hospitalizations, and rehabilitation | ||||
| Prospective observational study | Cost of admission and annual cost of AF (direct and indirect) | 5333 consecutive patients recruited from outpatient cardiology clinics, cardiology wards, first (heart) aids, and inpatient wards | Europe (35 countries) | Ringborg, 2008 (Euro Heart Survey)9 |
| Costs included diagnostic and interventional procedures, medications, inpatient care, consultations, and work loss | Data reported for Greece, Italy, Netherlands, Poland, and Spain | |||
| Outpatient clinic did not have cost of admission | ||||
| Prospective observational study | Direct and indirect costs over a mean follow-up of 329 days | 671 consecutive AF patients recruited by 82 cardiologists in their general office practice | France | Le Heuzey, 2004 (COCAF)10 |
| Costs included consultation, diagnostic and interventional procedures, medication, hospitalizations, and loss of work | ||||
| Prospective observational study, patient interviews | Direct and indirect costs of warfarin | 402 consecutive new patients with paroxysmal or chronic non-valvular AF referred by the community and outpatient clinics and treated by the physicians in a single-centre anticoagulation clinic | UK | Abdelhafiz and Wheeldon, 200311 |
| Costs included medications, monitoring and bleed-related physician visits, hospitalizations, and interventional procedures | ||||
| Prospective observational study | Costs of inpatient and outpatient cardioversion | 185 consecutive patients with symptomatic AF recruited from a university hospital (inpatient or outpatient setting) | Germany | Gronefeld, 200312 |
| Costs included physician visits, diagnostic and interventional procedures and medications, and hospitalization and treatment for inpatient care | ||||
| Prospective observational study | 30-day direct costs for AF patients presenting to an emergency department, before and after implementation of a new guideline for the management of patients. | 446 consecutive AF patients in an emergency department | USA | Zimetbaum, 200313 |
| Costs included emergency room care, diagnostic interventional procedures, inpatient, and follow-up care, which included outpatient services, visits to primary care physicians and cardiologists, and outpatient diagnostic, and therapeutic procedures | ||||
| Prospective observational study | Comparison of length of stay for stroke in AF and non-AF patients | 4534 consecutive stroke patients (803 with AF) recruited from hospitals | Europe (seven countries) | Lamassa, 200114 |
| Prospective cohort study; costs based on medicare payments plus patient copayments | 1-year medicare costs | 26 753 newly diagnosed, hospitalized patients, 13 558 with AF and 13 195 without AF, with one other cardiovascular diagnosis | USA | Wolf, 199815 |
| Costs included hospitalizations, nursing facilities, home health care, outpatient care, and physician visits | ||||
| Observational study; patient interviews and inpatient register | Direct costs for year before and year after radiofrequency ablation | 26 patients with resistant AF recruited from a hospital | Sweden | Jensen, 199516 |
| Costs included interventional procedures, medication, and hospitalization | ||||
| Prospective, observational study; survey of 18 academic medical centres | Cost of digoxin treatment | 115 patients with AF (85%), AFL (7%), or both (8%), recruited from a university hospital and its emergency department | USA | Roberts, 199317 |
| Costs included interventional procedures, medication, and hospitalization | ||||
| Semistructured interviews with NHS staff | Annual costs of INR monitoring and laboratory procedures | Six monitoring services (secondary-care Trusts) responsible for average of 3459 warfarin patients | UK | Arya, 200518 |
| Survey of 306 cardiologists; 100 responded | Annual cost of AF | 100 private-sector cardiologists | France | Jeantet, 200119 |
| Costs included medications and diagnostic procedures | ||||
| Prospective, randomized multicentre study | Costs of electroanatomically guided and conventional catheter ablation (interventional procedure costs) | 210 patients with AFL (concomitant AF permitted) recruited in hospital | Europe (8 centres) | Hindricks, 200920 |
| Economic evaluation alongside clinical trial | Time and travelling costs in attending anticoagulation clinics | 381 AF patients enrolled in a stroke prevention RCT recruited in an outpatient setting | Worldwide* | Jowett, 2008 (SPORTIF III trial)21 |
| Prospective, randomized pilot study | Compared accelerated emergency-department strategy using LMWH with traditional hospital admission | 18 patients with newly diagnosed AF who presented at an outpatient emergency department-based disease management centre | USA | Kim, 200322 |
| Costs included medication and hospitalization | ||||
| Cross-sectional observational study, patient and physician questionnaires | Annual direct and indirect costs in primary and secondary care | 922 patients with AF (538 in Germany, 384 in Sweden) from primary or specialist care centres (inpatient and outpatient settings) | Europe (two countries) | Ericsson, 200723 |
| Costs included physician visits, interventional procedures, hospitalization, medication, travel costs, home care, and other indirect costs | ||||
| Cross-sectional study; continuous morbidity recording scheme data | Frequency of primary care visits | 3135 patients with AF in a primary care setting | UK (Scotland) | Murphy, 200724 |
| Retrospective database analysis | Incremental inpatient costs for AF patients minus matched controls | 691 897 patients with secondary AF in an inpatient setting | USA | Exuzides, 200825 |
| Costs included hospitalization, interventional procedures, and medication | ||||
| Longitudinal, matched cohort database study; regression analysis | Incremental annual costs of inpatient and outpatient care | 55 260 AF patients recruited in an inpatient and outpatient setting | USA | Lee, 200826 |
| Costs included hospitalization, outpatient visits, physician visits, interventional procedures, medication, and nursing and home care | ||||
| Database analysis, chart review, and patient interviews | 1-year direct and indirect costs of stroke in AF patients | 71 consecutive AF patients with stroke, from a cohort of 558 stroke patients who presented at a hospital in an inpatient or outpatient setting | Germany | Bruggenjurgen, 200727 |
| Costs included hospitalization, outpatient visits, physician visits, interventional procedures, medication, nursing care and rehabilitation, and other indirect costs | ||||
| Database analysis; case-control and regression analyses | National incremental direct cost of hospital care | 348 131 non-valvular AF patients in hospital inpatient, outpatient, or office-visit settings | USA | Coyne, 200628 |
| Costs included inpatient and outpatient physician services, hospitalization, interventional procedures, and medication | ||||
| Retrospective database study in a finnish communal health care setting | Direct costs of warfarin treatment over a 12-month period | 250 warfarin-treated AF patients in a primary care setting | Finland | Hallinen, 200629 |
| Costs included physician visits, diagnostic procedures, hospitalization, and medication | ||||
| Administrative claims database analysis | Annual direct costs for newly diagnosed AF patients | Newly diagnosed patients with AF in primary care: 6846 warfarin-treated, 40 849 untreated | USA | Fidan, 200530 |
| Costs included interventional procedures, medication, and other direct costs | ||||
| Database analysis: medicare | Annual AF-related medical costs for medicare beneficiaries | 59 648 patients aged ≥65 years with AF from hospital inpatient and outpatient settings | USA | Pelletier, 200531 |
| Costs included inpatient and outpatient physician services, hospitalization, diagnostic and interventional procedures, and medication | ||||
| Retrospective analysis of a privately insured database (16 employers in the USA) | Excess annual direct and indirect costs | 3944 AF patients from hospital inpatient and outpatient settings | USA | Wu, 200532 |
| Costs included inpatient and outpatient physician services, hospitalization, diagnostic and interventional procedures, and medication | ||||
| Database analysis: medicare | Length-of-stay and hospital costs for patients with AF or AFL | Medicare beneficiaries: 8454 with AF and 986 with AFL, from hospital or institutional settings | USA | Baine, 200133 |
| Two retrospective electronic medical record and two Delphi-panel studies | Direct cost of INR monitoring | 1721 chronic AF patients from primary care settings | Sweden | Bjorholt, 200734 |
| Retrospective medical record review | Direct cost of hospitalizations for bleeding | 2460 warfarin-treated patients; cost data collected for three AF patients identified from a hospital anticoagulation service | USA | Fanikos, 200535 |
| Costs included emergency care, physician and nursing visits and care, diagnostic and interventional procedures, hospitalization, and medication | ||||
| Retrospective, observational cohort study | Total direct costs before and after AF diagnosis and after a stroke or bleeding event | 3891 newly diagnosed patients with chronic non-valvular AF, identified from hospital inpatient and outpatient settings | USA | Stephenson, 200536 |
| Costs included hospitalization, diagnostic and interventional procedures, and medication | ||||
| Retrospective analysis; direct and indirect costs included | Cost of outpatient cardioversion | 532 consecutive patients with atrial tachyarrhythmia, identified from an outpatient department | USA | Botkin, 200337 |
| Retrospective medical record study combined with patient interviews | Direct costs of radiofrequency ablation and drug treatment | 118 consecutive patients with symptomatic paroxysmal AF, identified in an inpatient setting | France | Weerasooriya, 200338 |
| Costs included hospitalization, consultations, interventional procedures, and medication | ||||
| Retrospective chart review | Direct costs of a first episode of uncomplicated AF | 47 patients with a first episode of uncomplicated AF, in a university hospital (emergency department) setting | USA | Kim, 200139 |
| Costs included hospitalization and interventional procedures | ||||
| Retrospective chart review | Cost of acute treatment in an emergency department | 114 consecutive AF patients identified from hospital emergency departments; first documented episode = 47% | USA | Dell'Orfano, 199940 |
| Cost included hospitalization and interventional procedures | ||||
| Review of hospital bills; indirect costs were defined as overhead and malpractice insurance | Comparison of radiofrequency modification and ablation of the atrioventricular junction | 24 patients with chronic AF treated in a hospital; costs based on subgroup of 16 patients | USA | Knight, 199741 |
| Costs included consultations, diagnostic and interventional procedures, and hospitalization | ||||
| Registry study | Effect of AF on stroke-related direct inpatient costs | 1619 stroke patients also diagnosed with AF | Sweden | Ghatnekar and Glader, 200842 |
| Registry, chart review, patient interviews, and case report forms | Annual direct costs of hospital care and impact of AF recurrence | 973 AF patients | USA | Reynolds, 2007 (FRACTAL)43 |
| Costs included consultations, diagnostic and interventional procedures, ambulatory monitoring, and hospitalization | ||||
| Combination of available prevalence data and resource use or cost estimates | National direct-cost estimates for 1995; projections for 2000 | AF patients | UK | Stewart, 200444 |
| Costs included consultations, diagnostic and interventional procedures, ambulatory monitoring and hospitalization, nursing home care, and medication |
| Study type and methods | Type of reported cost data | Population type and number | Country | Author, date |
|---|---|---|---|---|
| 6-month multicentre, prospective observational study with 3-month retrospective data collection | Annual direct costs | 361 consecutive AF patients (75% with persistent AF); recruited from general or family practices (67%), internal medicine (26%), or cardiology practices (7%) | Germany | McBride, 20098 |
| Costs included physician visits, diagnostic and interventional procedures, medication, emergency transports, hospitalizations, and rehabilitation | ||||
| Prospective observational study | Cost of admission and annual cost of AF (direct and indirect) | 5333 consecutive patients recruited from outpatient cardiology clinics, cardiology wards, first (heart) aids, and inpatient wards | Europe (35 countries) | Ringborg, 2008 (Euro Heart Survey)9 |
| Costs included diagnostic and interventional procedures, medications, inpatient care, consultations, and work loss | Data reported for Greece, Italy, Netherlands, Poland, and Spain | |||
| Outpatient clinic did not have cost of admission | ||||
| Prospective observational study | Direct and indirect costs over a mean follow-up of 329 days | 671 consecutive AF patients recruited by 82 cardiologists in their general office practice | France | Le Heuzey, 2004 (COCAF)10 |
| Costs included consultation, diagnostic and interventional procedures, medication, hospitalizations, and loss of work | ||||
| Prospective observational study, patient interviews | Direct and indirect costs of warfarin | 402 consecutive new patients with paroxysmal or chronic non-valvular AF referred by the community and outpatient clinics and treated by the physicians in a single-centre anticoagulation clinic | UK | Abdelhafiz and Wheeldon, 200311 |
| Costs included medications, monitoring and bleed-related physician visits, hospitalizations, and interventional procedures | ||||
| Prospective observational study | Costs of inpatient and outpatient cardioversion | 185 consecutive patients with symptomatic AF recruited from a university hospital (inpatient or outpatient setting) | Germany | Gronefeld, 200312 |
| Costs included physician visits, diagnostic and interventional procedures and medications, and hospitalization and treatment for inpatient care | ||||
| Prospective observational study | 30-day direct costs for AF patients presenting to an emergency department, before and after implementation of a new guideline for the management of patients. | 446 consecutive AF patients in an emergency department | USA | Zimetbaum, 200313 |
| Costs included emergency room care, diagnostic interventional procedures, inpatient, and follow-up care, which included outpatient services, visits to primary care physicians and cardiologists, and outpatient diagnostic, and therapeutic procedures | ||||
| Prospective observational study | Comparison of length of stay for stroke in AF and non-AF patients | 4534 consecutive stroke patients (803 with AF) recruited from hospitals | Europe (seven countries) | Lamassa, 200114 |
| Prospective cohort study; costs based on medicare payments plus patient copayments | 1-year medicare costs | 26 753 newly diagnosed, hospitalized patients, 13 558 with AF and 13 195 without AF, with one other cardiovascular diagnosis | USA | Wolf, 199815 |
| Costs included hospitalizations, nursing facilities, home health care, outpatient care, and physician visits | ||||
| Observational study; patient interviews and inpatient register | Direct costs for year before and year after radiofrequency ablation | 26 patients with resistant AF recruited from a hospital | Sweden | Jensen, 199516 |
| Costs included interventional procedures, medication, and hospitalization | ||||
| Prospective, observational study; survey of 18 academic medical centres | Cost of digoxin treatment | 115 patients with AF (85%), AFL (7%), or both (8%), recruited from a university hospital and its emergency department | USA | Roberts, 199317 |
| Costs included interventional procedures, medication, and hospitalization | ||||
| Semistructured interviews with NHS staff | Annual costs of INR monitoring and laboratory procedures | Six monitoring services (secondary-care Trusts) responsible for average of 3459 warfarin patients | UK | Arya, 200518 |
| Survey of 306 cardiologists; 100 responded | Annual cost of AF | 100 private-sector cardiologists | France | Jeantet, 200119 |
| Costs included medications and diagnostic procedures | ||||
| Prospective, randomized multicentre study | Costs of electroanatomically guided and conventional catheter ablation (interventional procedure costs) | 210 patients with AFL (concomitant AF permitted) recruited in hospital | Europe (8 centres) | Hindricks, 200920 |
| Economic evaluation alongside clinical trial | Time and travelling costs in attending anticoagulation clinics | 381 AF patients enrolled in a stroke prevention RCT recruited in an outpatient setting | Worldwide* | Jowett, 2008 (SPORTIF III trial)21 |
| Prospective, randomized pilot study | Compared accelerated emergency-department strategy using LMWH with traditional hospital admission | 18 patients with newly diagnosed AF who presented at an outpatient emergency department-based disease management centre | USA | Kim, 200322 |
| Costs included medication and hospitalization | ||||
| Cross-sectional observational study, patient and physician questionnaires | Annual direct and indirect costs in primary and secondary care | 922 patients with AF (538 in Germany, 384 in Sweden) from primary or specialist care centres (inpatient and outpatient settings) | Europe (two countries) | Ericsson, 200723 |
| Costs included physician visits, interventional procedures, hospitalization, medication, travel costs, home care, and other indirect costs | ||||
| Cross-sectional study; continuous morbidity recording scheme data | Frequency of primary care visits | 3135 patients with AF in a primary care setting | UK (Scotland) | Murphy, 200724 |
| Retrospective database analysis | Incremental inpatient costs for AF patients minus matched controls | 691 897 patients with secondary AF in an inpatient setting | USA | Exuzides, 200825 |
| Costs included hospitalization, interventional procedures, and medication | ||||
| Longitudinal, matched cohort database study; regression analysis | Incremental annual costs of inpatient and outpatient care | 55 260 AF patients recruited in an inpatient and outpatient setting | USA | Lee, 200826 |
| Costs included hospitalization, outpatient visits, physician visits, interventional procedures, medication, and nursing and home care | ||||
| Database analysis, chart review, and patient interviews | 1-year direct and indirect costs of stroke in AF patients | 71 consecutive AF patients with stroke, from a cohort of 558 stroke patients who presented at a hospital in an inpatient or outpatient setting | Germany | Bruggenjurgen, 200727 |
| Costs included hospitalization, outpatient visits, physician visits, interventional procedures, medication, nursing care and rehabilitation, and other indirect costs | ||||
| Database analysis; case-control and regression analyses | National incremental direct cost of hospital care | 348 131 non-valvular AF patients in hospital inpatient, outpatient, or office-visit settings | USA | Coyne, 200628 |
| Costs included inpatient and outpatient physician services, hospitalization, interventional procedures, and medication | ||||
| Retrospective database study in a finnish communal health care setting | Direct costs of warfarin treatment over a 12-month period | 250 warfarin-treated AF patients in a primary care setting | Finland | Hallinen, 200629 |
| Costs included physician visits, diagnostic procedures, hospitalization, and medication | ||||
| Administrative claims database analysis | Annual direct costs for newly diagnosed AF patients | Newly diagnosed patients with AF in primary care: 6846 warfarin-treated, 40 849 untreated | USA | Fidan, 200530 |
| Costs included interventional procedures, medication, and other direct costs | ||||
| Database analysis: medicare | Annual AF-related medical costs for medicare beneficiaries | 59 648 patients aged ≥65 years with AF from hospital inpatient and outpatient settings | USA | Pelletier, 200531 |
| Costs included inpatient and outpatient physician services, hospitalization, diagnostic and interventional procedures, and medication | ||||
| Retrospective analysis of a privately insured database (16 employers in the USA) | Excess annual direct and indirect costs | 3944 AF patients from hospital inpatient and outpatient settings | USA | Wu, 200532 |
| Costs included inpatient and outpatient physician services, hospitalization, diagnostic and interventional procedures, and medication | ||||
| Database analysis: medicare | Length-of-stay and hospital costs for patients with AF or AFL | Medicare beneficiaries: 8454 with AF and 986 with AFL, from hospital or institutional settings | USA | Baine, 200133 |
| Two retrospective electronic medical record and two Delphi-panel studies | Direct cost of INR monitoring | 1721 chronic AF patients from primary care settings | Sweden | Bjorholt, 200734 |
| Retrospective medical record review | Direct cost of hospitalizations for bleeding | 2460 warfarin-treated patients; cost data collected for three AF patients identified from a hospital anticoagulation service | USA | Fanikos, 200535 |
| Costs included emergency care, physician and nursing visits and care, diagnostic and interventional procedures, hospitalization, and medication | ||||
| Retrospective, observational cohort study | Total direct costs before and after AF diagnosis and after a stroke or bleeding event | 3891 newly diagnosed patients with chronic non-valvular AF, identified from hospital inpatient and outpatient settings | USA | Stephenson, 200536 |
| Costs included hospitalization, diagnostic and interventional procedures, and medication | ||||
| Retrospective analysis; direct and indirect costs included | Cost of outpatient cardioversion | 532 consecutive patients with atrial tachyarrhythmia, identified from an outpatient department | USA | Botkin, 200337 |
| Retrospective medical record study combined with patient interviews | Direct costs of radiofrequency ablation and drug treatment | 118 consecutive patients with symptomatic paroxysmal AF, identified in an inpatient setting | France | Weerasooriya, 200338 |
| Costs included hospitalization, consultations, interventional procedures, and medication | ||||
| Retrospective chart review | Direct costs of a first episode of uncomplicated AF | 47 patients with a first episode of uncomplicated AF, in a university hospital (emergency department) setting | USA | Kim, 200139 |
| Costs included hospitalization and interventional procedures | ||||
| Retrospective chart review | Cost of acute treatment in an emergency department | 114 consecutive AF patients identified from hospital emergency departments; first documented episode = 47% | USA | Dell'Orfano, 199940 |
| Cost included hospitalization and interventional procedures | ||||
| Review of hospital bills; indirect costs were defined as overhead and malpractice insurance | Comparison of radiofrequency modification and ablation of the atrioventricular junction | 24 patients with chronic AF treated in a hospital; costs based on subgroup of 16 patients | USA | Knight, 199741 |
| Costs included consultations, diagnostic and interventional procedures, and hospitalization | ||||
| Registry study | Effect of AF on stroke-related direct inpatient costs | 1619 stroke patients also diagnosed with AF | Sweden | Ghatnekar and Glader, 200842 |
| Registry, chart review, patient interviews, and case report forms | Annual direct costs of hospital care and impact of AF recurrence | 973 AF patients | USA | Reynolds, 2007 (FRACTAL)43 |
| Costs included consultations, diagnostic and interventional procedures, ambulatory monitoring, and hospitalization | ||||
| Combination of available prevalence data and resource use or cost estimates | National direct-cost estimates for 1995; projections for 2000 | AF patients | UK | Stewart, 200444 |
| Costs included consultations, diagnostic and interventional procedures, ambulatory monitoring and hospitalization, nursing home care, and medication |
AF, atrial fibrillation; AFL, atrial flutter; COCAF, Cost of Care in Atrial Fibrillation trial; FRACTAL, fibrillation registry assessing costs, Therapies, Adverse Events and Lifestyle registry; INR, international normalized ratio; LMWH, low molecular-weight heparin; NHS, National Health Service (UK); RCT, randomized controlled trial; SPORTIF III, stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation trial; UK, United Kingdom; USA, United States of America.
*Australia, France, Portugal, Spain, Sweden, and the United Kingdom.
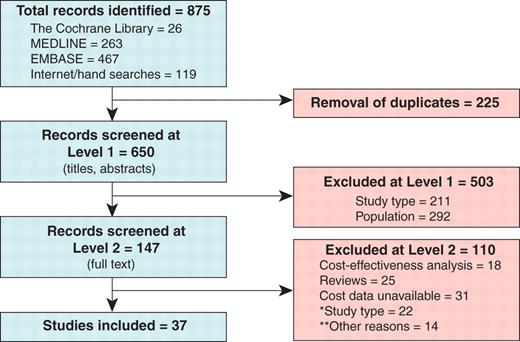
Flowchart for study inclusion and exclusion. AF, atrial fibrillation. *‘Study type’ includes studies with narrow cost perspectives. **‘Other reasons’ includes data not specific to atrial fibrillation patients, irrelevant of care management.
Of the 37 studies, 17 were prospective (10 observational studies,8–17 two surveys,18,19 three clinical trials20–22, and two cross-sectional studies),23,24 19 were retrospective (nine databases,25–33 eight medical records,34–41 and two registries),42,43 and one study was a synthesis of published data.44 Sixteen studies estimated annual costs, 15 estimated inpatient costs, and three estimated outpatient hospital costs.
The studies encompassed 16 countries: Australia,21 England,14 Finland,29 France,10,14,19,21,38 Germany,8,12,14,23,27 Greece,9 Hungary,14 Italy,9,14 the Netherlands,9 Poland,9 Portugal,14,21 Scotland,24 Spain,9,14,21 Sweden,16,21,23,34,42 the UK,11,18,21,44 and the USA.13,15,17,22,25,26,28,30–33,35–37,39–41,43 Most studies estimated costs associated with AF in the USA (18 studies) or Western Europe (14 studies) (Table 1). Cost-years ranged from 1991 to 2006.
Review results
National cost-of-illness estimates
Three national cost-of-illness estimates were identified.19,28,44 Stewart et al.44 combined published prevalence data, resource use, and cost estimates to estimate the national cost of illness in the United Kingdom for 1995. Costs were projected to 2000, adjusting for population ageing. The direct cost was £244 million or 0.62% of total National Health Service (NHS) expenditures in 1995. Hospitalizations and drug prescriptions accounted for 50 and 20% of this expenditure, respectively. Long-term nursing home care after hospital admission cost an additional £46.4 million. When projected to 2000, the direct cost approximately doubled to £459 million, equivalent to 0.97% of total NHS expenditures; nursing home costs rose to £111 million.
Coyne et al.28 estimated the national cost of hospital treatment of non-valvular AF in 2005 via a retrospective analysis of three federally funded US databases. Case–control comparison and regression analysis were performed to estimate the incremental costs associated with AF. The national cost of hospital treatment was estimated as $6.65 billion, including $2.93 billion (44%) for hospitalizations with a principal discharge diagnosis of AF, $1.95 billion (29%) for the incremental inpatient cost of AF as a comorbid diagnosis, $1.53 billion (23%) for outpatient treatment of AF, and $235 million (4%) for prescription drugs.
Jeantet et al.19 estimated the annual cost in France as €305 million in 2000 for treatment of the first two episodes of AF in the >65 age group alone. Disaggregated costs were not reported.
Annual cost per patient
Annual per-patient cost estimates were reported by 15 studies. Five studies included only the cost of International Normalized Ratio monitoring or warfarin treatment11,18,19,21,34Table 2 presents the remaining 10 studies. Of these, four studies considered special populations. Weerasooriya et al.38 studied patients undergoing catheter ablation, Fidan et al.30 studied patients with newly diagnosed AF, and Lee et al.26 and Pelletier et al.31 studied elderly patients (Medicare beneficiaries, i.e. those 65 years or older).
Annual cost estimates for atrial fibrillation and cost types includeda
| Author (date) | Ringborg (2008)9 | Weera-sooriya (2003)38 | Jeantet (2001)19 | Ericsson (2007)23 | McBride (2009)8 | Lee (2008)26 | Reynolds (2007)43 | Wu (2005)32 | Fidan (2005)30 | Pelletier (2005)31 |
|---|---|---|---|---|---|---|---|---|---|---|
| Country (cost-year) | Europe (five Countries) (2006) | France (2001) | France (2000) | Germany, Sweden (2005) | Germany (2004) | USA (2004) | USA (2004) | USA (2002) | USA (2001) | USA (1999) |
| Patient population | Consecu-tive outpatients and inpatients | Patients under-going catheter ablation | Patients managed in a community setting | Patients managed in primary care or specialist centres | Patients managed in general internal medicine or cardiology practices | Elderly patients (medicare beneficiaries) | Patients from 17 centres entered in the FRACTAL Registry | Privately insured patients | Newly diagnosed patients | Elderly patients(medicarebene-ficiaries) |
| Cost categories included | ||||||||||
| Hospitalizations | Yes AF | Yes | No | Yes AF C | Yes | Yes | Yes AF ST BL | Yes | NRb | Yes |
| Drugs | Yes AA AT | Yes AA | Yes AA AT | Yes | Yes | ? | Yes AA AT | Yes | NRb | No |
| Consultations | Yes | Yes D ER | No | Yes OP | Yes | Yes D OP ER | Yes OP | Yes OP | NRb | Yes OP |
| Diagnostics | Yes | ? | Yes | ? | Yes | ? | Yes | Yes | NRb | ? |
| INR testing | No | No | No | ? | Yes | ? | Yes | No | NRb | No |
| Residential care | No | No | No | Yes | No | Yes | No | No | NRb | No |
| Other direct | No | No | No | No | PT ADL | No | No | No | NRb | No |
| Work loss | Yes | No | No | Yes | No | No | No | Yes | No | No |
| Travel costs | No | No | No | Yes | Yes | No | No | No | No | No |
| Other indirect | No | No | No | HH DC HDM | No | No | No | No | No | No |
| Results | ||||||||||
| Direct cost | Gr: €1372 | €445–1590c | €659–1092d | NR | €827 | $14 199 | $2372–10 312e | $12,349 | $10,131–10,560f | $11,675 |
| It: €3019 | ||||||||||
| Nl: €1937 | ||||||||||
| Po: €971 | ||||||||||
| Sp: €2073 | ||||||||||
| Indirect cost | Gr: €135 | NI | NI | NR | NI | NI | NI | $2526 | NI | NI |
| It: €206 | ||||||||||
| Nl: €391 | ||||||||||
| Po: €39 | ||||||||||
| Sp: €242 | ||||||||||
| Total cost | Gr: €1507 | NA | NA | €5586g | NA | NA | NA | $14,875 | NA | NA |
| It: €3225 | ||||||||||
| Nl: €2328 | ||||||||||
| Po: €1010 | ||||||||||
| Sp: €2315 | ||||||||||
| Author (date) | Ringborg (2008)9 | Weera-sooriya (2003)38 | Jeantet (2001)19 | Ericsson (2007)23 | McBride (2009)8 | Lee (2008)26 | Reynolds (2007)43 | Wu (2005)32 | Fidan (2005)30 | Pelletier (2005)31 |
|---|---|---|---|---|---|---|---|---|---|---|
| Country (cost-year) | Europe (five Countries) (2006) | France (2001) | France (2000) | Germany, Sweden (2005) | Germany (2004) | USA (2004) | USA (2004) | USA (2002) | USA (2001) | USA (1999) |
| Patient population | Consecu-tive outpatients and inpatients | Patients under-going catheter ablation | Patients managed in a community setting | Patients managed in primary care or specialist centres | Patients managed in general internal medicine or cardiology practices | Elderly patients (medicare beneficiaries) | Patients from 17 centres entered in the FRACTAL Registry | Privately insured patients | Newly diagnosed patients | Elderly patients(medicarebene-ficiaries) |
| Cost categories included | ||||||||||
| Hospitalizations | Yes AF | Yes | No | Yes AF C | Yes | Yes | Yes AF ST BL | Yes | NRb | Yes |
| Drugs | Yes AA AT | Yes AA | Yes AA AT | Yes | Yes | ? | Yes AA AT | Yes | NRb | No |
| Consultations | Yes | Yes D ER | No | Yes OP | Yes | Yes D OP ER | Yes OP | Yes OP | NRb | Yes OP |
| Diagnostics | Yes | ? | Yes | ? | Yes | ? | Yes | Yes | NRb | ? |
| INR testing | No | No | No | ? | Yes | ? | Yes | No | NRb | No |
| Residential care | No | No | No | Yes | No | Yes | No | No | NRb | No |
| Other direct | No | No | No | No | PT ADL | No | No | No | NRb | No |
| Work loss | Yes | No | No | Yes | No | No | No | Yes | No | No |
| Travel costs | No | No | No | Yes | Yes | No | No | No | No | No |
| Other indirect | No | No | No | HH DC HDM | No | No | No | No | No | No |
| Results | ||||||||||
| Direct cost | Gr: €1372 | €445–1590c | €659–1092d | NR | €827 | $14 199 | $2372–10 312e | $12,349 | $10,131–10,560f | $11,675 |
| It: €3019 | ||||||||||
| Nl: €1937 | ||||||||||
| Po: €971 | ||||||||||
| Sp: €2073 | ||||||||||
| Indirect cost | Gr: €135 | NI | NI | NR | NI | NI | NI | $2526 | NI | NI |
| It: €206 | ||||||||||
| Nl: €391 | ||||||||||
| Po: €39 | ||||||||||
| Sp: €242 | ||||||||||
| Total cost | Gr: €1507 | NA | NA | €5586g | NA | NA | NA | $14,875 | NA | NA |
| It: €3225 | ||||||||||
| Nl: €2328 | ||||||||||
| Po: €1010 | ||||||||||
| Sp: €2315 | ||||||||||
AA, antiarrhythmic; ADL, aids for daily living; AF, atrial fibrillation; AT, antithrombotic; BL, bleeding; C, complications; CV, cardiovascular; D, doctor; DC, day care; ER, emergency room; Gr, Greece; HDM, home delivery meals; HH, home help; INR, international normalized ratio; It, Italy; NA, not applicable; NI, not included; Nl, Netherlands; NR, not reported; OP, outpatient; Po, Poland; PT, physiotherapy; Sp, Spain; ST, stroke; UK, United Kingdom; USA, United States of America; ?, unclear.
aNo annual per-patient cost estimates were identified for the UK.
bAbstract available only; detail not reported.
cYear prior to ablation = €1,590; year after ablation = €445.
dPersistent AF = €659–783; with previous CV disease = €755–1092.
eMean annual cost for permanent AF and ≥3 recurrences, respectively; estimate for no recurrence = $3385; 1–2 recurrences = $6331.
fCost estimate for warfarin-untreated and warfarin-treated cohorts, respectively.
gCost estimates were reported for Germany and Sweden. Data for Germany are shown. Total costs for Sweden were €7241.
Annual cost estimates for atrial fibrillation and cost types includeda
| Author (date) | Ringborg (2008)9 | Weera-sooriya (2003)38 | Jeantet (2001)19 | Ericsson (2007)23 | McBride (2009)8 | Lee (2008)26 | Reynolds (2007)43 | Wu (2005)32 | Fidan (2005)30 | Pelletier (2005)31 |
|---|---|---|---|---|---|---|---|---|---|---|
| Country (cost-year) | Europe (five Countries) (2006) | France (2001) | France (2000) | Germany, Sweden (2005) | Germany (2004) | USA (2004) | USA (2004) | USA (2002) | USA (2001) | USA (1999) |
| Patient population | Consecu-tive outpatients and inpatients | Patients under-going catheter ablation | Patients managed in a community setting | Patients managed in primary care or specialist centres | Patients managed in general internal medicine or cardiology practices | Elderly patients (medicare beneficiaries) | Patients from 17 centres entered in the FRACTAL Registry | Privately insured patients | Newly diagnosed patients | Elderly patients(medicarebene-ficiaries) |
| Cost categories included | ||||||||||
| Hospitalizations | Yes AF | Yes | No | Yes AF C | Yes | Yes | Yes AF ST BL | Yes | NRb | Yes |
| Drugs | Yes AA AT | Yes AA | Yes AA AT | Yes | Yes | ? | Yes AA AT | Yes | NRb | No |
| Consultations | Yes | Yes D ER | No | Yes OP | Yes | Yes D OP ER | Yes OP | Yes OP | NRb | Yes OP |
| Diagnostics | Yes | ? | Yes | ? | Yes | ? | Yes | Yes | NRb | ? |
| INR testing | No | No | No | ? | Yes | ? | Yes | No | NRb | No |
| Residential care | No | No | No | Yes | No | Yes | No | No | NRb | No |
| Other direct | No | No | No | No | PT ADL | No | No | No | NRb | No |
| Work loss | Yes | No | No | Yes | No | No | No | Yes | No | No |
| Travel costs | No | No | No | Yes | Yes | No | No | No | No | No |
| Other indirect | No | No | No | HH DC HDM | No | No | No | No | No | No |
| Results | ||||||||||
| Direct cost | Gr: €1372 | €445–1590c | €659–1092d | NR | €827 | $14 199 | $2372–10 312e | $12,349 | $10,131–10,560f | $11,675 |
| It: €3019 | ||||||||||
| Nl: €1937 | ||||||||||
| Po: €971 | ||||||||||
| Sp: €2073 | ||||||||||
| Indirect cost | Gr: €135 | NI | NI | NR | NI | NI | NI | $2526 | NI | NI |
| It: €206 | ||||||||||
| Nl: €391 | ||||||||||
| Po: €39 | ||||||||||
| Sp: €242 | ||||||||||
| Total cost | Gr: €1507 | NA | NA | €5586g | NA | NA | NA | $14,875 | NA | NA |
| It: €3225 | ||||||||||
| Nl: €2328 | ||||||||||
| Po: €1010 | ||||||||||
| Sp: €2315 | ||||||||||
| Author (date) | Ringborg (2008)9 | Weera-sooriya (2003)38 | Jeantet (2001)19 | Ericsson (2007)23 | McBride (2009)8 | Lee (2008)26 | Reynolds (2007)43 | Wu (2005)32 | Fidan (2005)30 | Pelletier (2005)31 |
|---|---|---|---|---|---|---|---|---|---|---|
| Country (cost-year) | Europe (five Countries) (2006) | France (2001) | France (2000) | Germany, Sweden (2005) | Germany (2004) | USA (2004) | USA (2004) | USA (2002) | USA (2001) | USA (1999) |
| Patient population | Consecu-tive outpatients and inpatients | Patients under-going catheter ablation | Patients managed in a community setting | Patients managed in primary care or specialist centres | Patients managed in general internal medicine or cardiology practices | Elderly patients (medicare beneficiaries) | Patients from 17 centres entered in the FRACTAL Registry | Privately insured patients | Newly diagnosed patients | Elderly patients(medicarebene-ficiaries) |
| Cost categories included | ||||||||||
| Hospitalizations | Yes AF | Yes | No | Yes AF C | Yes | Yes | Yes AF ST BL | Yes | NRb | Yes |
| Drugs | Yes AA AT | Yes AA | Yes AA AT | Yes | Yes | ? | Yes AA AT | Yes | NRb | No |
| Consultations | Yes | Yes D ER | No | Yes OP | Yes | Yes D OP ER | Yes OP | Yes OP | NRb | Yes OP |
| Diagnostics | Yes | ? | Yes | ? | Yes | ? | Yes | Yes | NRb | ? |
| INR testing | No | No | No | ? | Yes | ? | Yes | No | NRb | No |
| Residential care | No | No | No | Yes | No | Yes | No | No | NRb | No |
| Other direct | No | No | No | No | PT ADL | No | No | No | NRb | No |
| Work loss | Yes | No | No | Yes | No | No | No | Yes | No | No |
| Travel costs | No | No | No | Yes | Yes | No | No | No | No | No |
| Other indirect | No | No | No | HH DC HDM | No | No | No | No | No | No |
| Results | ||||||||||
| Direct cost | Gr: €1372 | €445–1590c | €659–1092d | NR | €827 | $14 199 | $2372–10 312e | $12,349 | $10,131–10,560f | $11,675 |
| It: €3019 | ||||||||||
| Nl: €1937 | ||||||||||
| Po: €971 | ||||||||||
| Sp: €2073 | ||||||||||
| Indirect cost | Gr: €135 | NI | NI | NR | NI | NI | NI | $2526 | NI | NI |
| It: €206 | ||||||||||
| Nl: €391 | ||||||||||
| Po: €39 | ||||||||||
| Sp: €242 | ||||||||||
| Total cost | Gr: €1507 | NA | NA | €5586g | NA | NA | NA | $14,875 | NA | NA |
| It: €3225 | ||||||||||
| Nl: €2328 | ||||||||||
| Po: €1010 | ||||||||||
| Sp: €2315 | ||||||||||
AA, antiarrhythmic; ADL, aids for daily living; AF, atrial fibrillation; AT, antithrombotic; BL, bleeding; C, complications; CV, cardiovascular; D, doctor; DC, day care; ER, emergency room; Gr, Greece; HDM, home delivery meals; HH, home help; INR, international normalized ratio; It, Italy; NA, not applicable; NI, not included; Nl, Netherlands; NR, not reported; OP, outpatient; Po, Poland; PT, physiotherapy; Sp, Spain; ST, stroke; UK, United Kingdom; USA, United States of America; ?, unclear.
aNo annual per-patient cost estimates were identified for the UK.
bAbstract available only; detail not reported.
cYear prior to ablation = €1,590; year after ablation = €445.
dPersistent AF = €659–783; with previous CV disease = €755–1092.
eMean annual cost for permanent AF and ≥3 recurrences, respectively; estimate for no recurrence = $3385; 1–2 recurrences = $6331.
fCost estimate for warfarin-untreated and warfarin-treated cohorts, respectively.
gCost estimates were reported for Germany and Sweden. Data for Germany are shown. Total costs for Sweden were €7241.
Direct-cost estimates ranged from ∼$10 100 to 14 200 in the USA (excluding one low outlier: Reynolds et al.43 for AF with no recurrence) and from €450 to 3000 in Western Europe per patient per year (Table 2). If indirect costs were included, costs increased by up to 20%. However, the scope of resources included varied widely (Table 2).
Figure 2 presents the contribution of hospitalizations, drugs, and other resource use to the annual direct costs of AF. Hospitalizations were the dominant cost driver, representing between 44%8 and 87%9 of total annual direct costs.
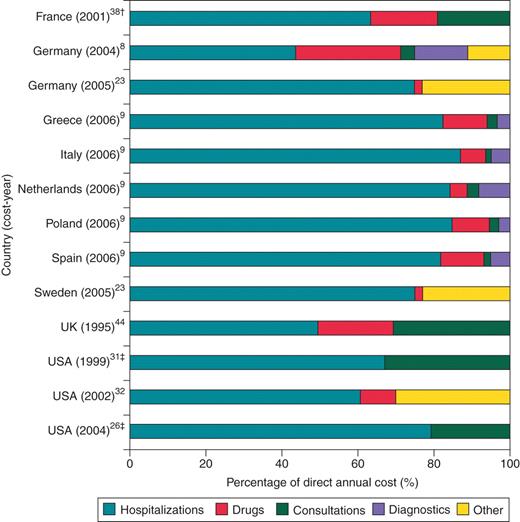
Contribution of hospitalizations, drugs, and other resource use to direct annual costs of atrial fibrillation*. AF, atrial fibrillation; UK, United Kingdom; USA, United States of America. *The following studies are not presented because disaggregated costs were not reported: Jeantet19; Reynolds43; Fidan.30 †For patients undergoing catheter ablation. ‡For elderly patients (medicare beneficiaries, i.e. those aged 65 years and older).
The Euro Heart Survey9 was the largest study identified, enrolling 5333 patients in 35 countries in 2003–2004. Ringborg et al.9 reported data for the five countries in which >200 patients were enrolled. The study estimated the cost of admission and the annual cost for the year after the admission (cost-year = 2006), based on prospective data collection, medical record review, and patient interviews. Mean costs of inpatient admission were estimated at €1363, 5252, 2322, 6360, and 6445, and mean costs incurred on an annual basis were estimated at €1507, 3225, 1010, 2315, and 2328 in Greece, Italy, Poland, Spain, and the Netherlands, respectively. Inpatient care and interventional procedures were identified as the main drivers of costs, accounting for >70% of total annual costs in all five countries.
In other studies, costs were higher for patients receiving rhythm-control treatment than for those receiving rate-control or no antiarrhythmic treatment.8 Costs increased with the number of AF recurrences43 and were higher for female vs. male patients,31 for younger vs. older patients,31 and for patients with comorbidity.23,31 In Germany, costs were lowest for patients with permanent AF and highest for those with persistent AF, while costs in Sweden were equally high for paroxysmal and persistent AF patients; the authors did not comment on these findings.23
Hospital costs
Direct hospitalization costs ranged from $170022 to 18 80041 in the USA and from ∼€13009 to 64009 in Western Europe (Figure 3). In the USA, the type of hospitalization varied widely, from first hospitalization for uncomplicated new-onset AF ($1700) 22 to complex procedures such as ablation of the atrioventricular junction in drug-refractory patients with an uncontrolled ventricular rate ($18 800).41 For studies enrolling consecutive AF patients with no particular characteristics or treatments specified, direct-cost estimates ranged from $256213 to 6692.40
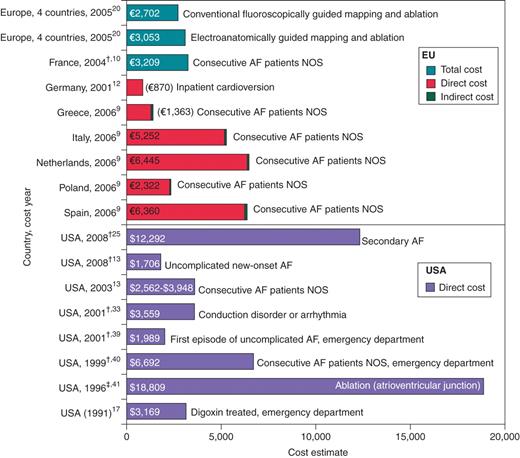
Inpatient cost estimates for atrial fibrillation*. AF, atrial fibrillation; EU, European union; NOS, not otherwise specified; USA, United States of America. *Cost estimate reported as USA $1000 has been converted to euros (exchange rate = 0.791, valid for 14 July 2010). †Cost-year not reported; date represents year of publication. ‡For ablation of the atrioventricular junction; radiofrequency modification: direct cost = £2644; indirect cost = $2082; total cost = $4726.
The cost of outpatient cardioversion was estimated at $46012 and $464 (direct = $304; indirect = $160.35).37 The direct cost of an accelerated emergency-department strategy using low-molecular-weight heparin was estimated at $879.28.22
Cost of hospitalization for bleeding complications
Four studies estimated the costs of bleeding complications in AF patients. Fanikos et al.35 reported a mean hospitalization cost for major bleeding complications of $15 988 in patients treated with warfarin in the USA between 2000 and 2003 (13 episodes in 12 patients). The average length of stay was 6 days. The incidence of major bleeding (defined by the thrombolysis in myocardial infarction criteria45) was 0.12% per year; therefore, the average annual cost per patient receiving warfarin treatment that was associated with management of major bleeding was $15 988 × 0.0012 = $19. Abdelhafiz and Wheeldon11 reported an average annual cost of £47.30 associated with management of bleeding per patient receiving warfarin therapy in the United Kingdom in 1999–2000. McBride et al.8 reported an average annual cost of €15 associated with inpatient care for bleeding per AF patient in Germany in 2004. Stephenson et al.36 estimated direct costs after a major bleed, transient ischaemic attack, or ischaemic stroke as $2311 for the USA in 2004.
Cost of stroke in atrial fibrillation patients
Two studies estimated the cost of stroke in AF patients, one in Germany27 and one in Sweden.42 One study14 reported length-of-stay estimates across seven European countries. Direct costs were estimated as €11 799 (1-year period in Germany; cost-year not reported)27 and €10 192 (3-year period in Sweden; cost-year = 2001).42 Neither estimate included indirect costs. The mean length-of-stay for stroke patients with AF was reported as 23.9 ± 26.6 days.14
The cost of stroke in patients with AF was significantly higher than in patients without AF: €11 799 vs. 8817 (P < 0.001; data for Germany; cost-year not reported)27 and €10 192 vs. 9374 (P < 0.01; data for Sweden; cost-year 2001).42 Controlling for baseline variables, stroke patients with AF had an almost 50% higher probability of remaining disabled or handicapped than stroke patients without AF.14
Costs were dominated by acute hospitalization (46%), inpatient rehabilitation (13%), readmission (12%), and nursing care (10%).27 Costs were highest in year 1 (€9012) and declined in years 2 (€5817) and 3 (€5079).42 Costs declined with increasing age, from €13 981 in patients aged 65 years or younger to €8852 in patients aged 84 years or older.42
Discussion
The cost of managing individual AF patients is high. Most estimates of the direct cost per patient-year ranged from ∼$10 100 to 14 200 in the USA and from €450 to 3000 in Western Europe.
These estimates are comparable with those reported from the economic analyses performed for the RACE and AFFIRM trials. In the RACE trial, the mean costs for rate- and rhythm-control strategies were estimated as €7386 and 8284, respectively, over a mean follow-up of 2.3 years.7 In the AFFIRM trial, the mean costs for rate- and rhythm-control strategies were estimated as $20 546 and 25 623 over a mean lifetime of 4.67 and 4.60 years, respectively.6
Inpatient care and interventional procedures represented the largest cost component (where reported), accounting for 50–70% of mean total costs. Inpatient costs ranged from $1700 to 18 800 in the USA and from €1300 to 6400 in Western Europe. The lower end of the range in the USA represented admissions for new-onset AF in patients without comorbidity22; the upper end represented ablation of the atrioventricular junction in drug-refractory patients with uncontrolled ventricular rates (this is higher than the highest cost per patient-year estimate because the latter represents the mean cost for all AF patients, including those who are not hospitalized).41
The direct cost of managing AF represented 0.9–2.4% of the national health care budget for the United Kingdom in 2000. In the USA, AF hospitalizations alone cost ∼$6.65 billion per annum in 2005. If indirect costs were included, cost estimates increased by up to 20% over direct costs alone.
The annual cost on a per-patient basis is comparable to estimates for diabetes (€5262 for Germany),46 chronic angina ($4949 for the USA),47 multiple sclerosis ($3868 for the USA),48 or psoriasis (€1173–4985 for Germany).49 However, compared with more prevalent diseases, such as diabetes, the economic burden of AF is expected to be lower on a national basis.
Costs have increased markedly over recent decades, due to ageing populations. In the United Kingdom in 1995, AF cost the NHS an estimated £243.9 million, accounting for 0.6 and 1.2% of NHS's total expenditure.44 The projected cost in 2000 was approximately double, at £459 million (0.9 and 2.4% of NHS expenditure).44 Atrial fibrillation-related hospitalizations have been increasing steadily over the last two decades4 and almost tripled in 2000 compared with two decades ago.5
The conclusions that may be drawn from this systematic review are limited by the nature of the studies identified. Costs ranged from 1991 to 2006 and across 16 countries. Very few national cost-of-illness estimates were identified, and comprehensive, current estimates were not available for many countries. Synthesis of cost estimates was confounded by substantial methodological heterogeneity between studies and by diversity of the populations studied and the scope of resource items included. Implementing guidelines to standardize methods and study designs for cost-of-illness studies would be worthwhile.50 However, this review provides an overview of the range of estimates reported in recent years, and the collated evidence provides greater certainty about the cost of illness associated with AF than is provided by individual studies. Studies consistently reported hospitalization as the key cost driver for AF.
In conclusion, this review of the cost of illness associated with AF has shown that hospitalizations represent the major cost driver, accounting for 50–70% of total costs. If indirect costs were included, costs increased by up to 20% over direct costs alone. Costs and hospitalizations attributable to AF have increased markedly over recent decades and are expected to increase, due to ageing populations. However, these costs are expected to remain low in comparison with other, more prevalent diseases, such as diabetes and hypertension.
Conflict of interest: RTI-HS has provided consulting services to sanofi-aventis and other pharmaceutical companies. Isabelle van Gelder has received research funding from, and has acted as a consultant to, sanofi-aventis and other pharmaceutical and medical companies.
Funding
This research was sponsored by sanofi-aventis R&D, France.

{kind=link}
{kind=link}
{kind=link}